SUO 2025
SUO 2025
SUO 2025: Huggins Medal Lecture: What I Did and What I Am Doing
- Details
(UroToday.com) The 2025 SUO annual meeting featured the Huggins Medal Lecture and presentation by this year’s recipient, Dr. Peter Carroll, discussing “What I did and What I am Doing”. Important themes in his presentation consisted of people (teams), data (information), and practice. As an editorial note, Dr. Carroll stated that “When I say I, I mean we. When I say we, I mean they.”
SUO 2025: Emerging Frontiers in Metastatic Prostate Cancer: Approved, Advancing, and Ahead
- Details
(UroToday.com) The 2025 SUO annual meeting featured a prostate cancer session and a presentation by Dr. Rana McKay discussing emerging frontiers in metastatic prostate cancer. Dr. McKay started her presentation by making a plea for increasing genetic testing in metastatic prostate cancer, both somatic and germline testing, given that appropriate genetic testing will increasingly guide therapy moving forward. Somatic testing can be both prognostic and predictive (HRR, MSI). Germline testing can (i) be prognostic, (ii) be predictive, (iii) lead to cascade testing, and (iv) lead to secondary cancer screening.
SUO 2025: Primary Efficacy and Surgical Details in KEYNOTE-905: Neoadjuvant and Adjuvant Enfortumab Vedotin Plus Pembrolizumab in Participants with Muscle-invasive Bladder Cancer Who Are Cisplatin-ineligible
- Details
(UroToday.com) At the 2025 SUO Annual Meeting, Dr. Hristos Kaimakliotis presented the primary efficacy and surgical outcomes from KEYNOTE-905/EV-303, a phase III study evaluating perioperative enfortumab vedotin plus pembrolizumab (EV + pembro) versus radical cystectomy (RC) alone in cisplatin-ineligible patients with cT2–T4aN0M0 or T1–T4aN1M0 muscle-invasive bladder cancer.
Johnson & Johnson’s INLEXZO™ (Gemcitabine Intravesical System) Delivers 74 Percent Disease-Free Survival at One Year in BCG-Unresponsive, High-Risk, Papillary-Only NMIBC
- Details
- New data from Cohort 4 of the SunRISe-1 study show more than 95 percent of patients remained progression free at one year, with more than 92 percent not undergoing bladder removal
- Patients with this type of bladder cancer have limited choices beyond radical cystectomy, highlighting the need for newer therapies for bladder preservation
New Cretostimogene Grenadenorepvec Data Highlight its Potential to Become the Backbone Therapy for High-Risk Non-Muscle Invasive Bladder Cancer
- Details
- Cretostimogene demonstrated HG-EFS at 3- 6- and 9-months of 95.7%, 84.6% and 80.4%, respectively, in HR BCG UR Ta/T1 Disease in BOND-003 Cohort P
- CORE-008 Cohort A Data in HR BCG-Naïve NMIBC demonstrates 88% CR and favorable safety with optimized administration
- Robust clinical pipeline that spans multiple late-stage studies across intermediate- and high-risk NMIBC
Reno, Nevada (UroToday.com) -- CG Oncology, Inc. (NASDAQ: CGON), a late-stage clinical biopharmaceutical company focused on developing and commercializing a potential backbone bladder-sparing therapeutic for patients with bladder cancer, today announced topline data from BOND-003 Cohort P and first results from CORE-008 Cohort A which demonstrated promising efficacy, safety and tolerability. These data will be presented today as Late-Breaking Abstracts at the Society of Urologic Oncology (SUO) 26th Annual Meeting.
“For people living with bladder cancer, the need for primary treatment of newly diagnosed NMIBC and a durable, bladder-sparing option for those with BCG unresponsive disease is urgent. New data from BOND-003 Cohort P and CORE-008 Cohort A add to a growing body of evidence demonstrating cretostimogene’s potential to become a backbone treatment across the NMIBC spectrum, if approved. The topline efficacy, safety, and tolerability announced today are consistent with what we previously observed with the pivotal Phase 3 monotherapy data, but in an even more prevalent NMIBC population, notably BCG-UR papillary-only,” said Trinity J. Bivalacqua, M.D., Ph.D., Urologic Oncologist at University of Pennsylvania.
“We are delighted to share new and more mature data in different sub-groups, underscoring our commitment to address the broadest range of NMIBC patients. This sets us up for the future expansion and long-term success of cretostimogene. With its best-in-disease profile and dual MOA, we are confident that cretostimogene will continue to demonstrate differentiated data from current and investigational NMIBC therapies,” said Ambaw Bellete, President & Chief Operating Officer at CG Oncology.
TOPLINE BOND-003 COHORT P RESULTS
Results from the BOND-003 Cohort P clinical trial of cretostimogene monotherapy in patients with BCG-UR papillary-only NMIBC demonstrate encouraging HG-EFS and a consistent, well-tolerated safety profile. The study’s primary endpoint is High-Grade Event-Free Survival (HG-EFS). As of the September 1, 2025, data cut-off, in 51 efficacy evaluable patients, Kaplan-Meier estimates of HG-EFS at 3- 6- and 9-months are 95.7% (95% CI 83.8 – 98.9), 84.6% (95% CI 68.6 – 92.9%) and 80.4% (95% CI 62.3-90.4%), respectively.
A favorable safety and tolerability profile was observed with no Grade 3 or greater treatment-related adverse events (TRAEs) and no deaths reported. To date, no patients have undergone a radical cystectomy or progressed to MIBC. No treatment-related discontinuation of cretostimogene was observed. There were no missed doses, or dose delays due to TRAE. The most common TRAEs (≥10%) were bladder spasms, dysuria, pollakiuria, and hematuria.
The study has completed enrollment with 56 patients receiving cretostimogene across 35 clinical sites in the United States and Japan.
CORE-008 Cohort A Results
The first results from CORE-008 Cohort A demonstrate that cretostimogene monotherapy has promising clinical efficacy, tolerability, and safety in patients with high-risk, BCG-naïve NMIBC with CIS, compared with outcomes observed in historical BCG-naive trials. The primary endpoint is Complete Response (CR) at any time. As of the September 1, 2025, data cut off, the overall CR rate at any time in evaluable patients is 83.7% (41/49) (95% CI 70.3-92.7%) with the original administration achieving a 79.2% CR rate (57.8, 92.9) in 19 out of 24 patients as compared with the optimized administration which resulted in an 88.0% CR rate (68.8, 97.5) in 22 out of 25 patients.
The safety and tolerability profile is consistent with prior clinical trials of cretostimogene. The most common adverse events are low grade and localized to the bladder. There are no related serious adverse events (SAEs), Grade 3+ adverse events or treatment-related discontinuations. No patients progressed to MIBC or metastatic disease.
| CORE-008 Cohort A | CR Rate, % (95% CI) |
Safety (n=54) |
|
| Any Grade | Grade ≥ 3 | ||
| Original Administration (five-step) | 79.2% (57.8, 92.9)1 | 16 (59.3%)1 | 0 (0%) |
| Optimized Administration (two-step) | 88.0% (68.8, 97.5)2 | 13 (48.1%) | 0 (0%) |
| Overall | 83.7% | 29 (53.7%) | 0 (0%) |
1 CR rate in 19 out of 24 patients; safety in 27 patients
2 CR rate in 22 out of 25 patients; safety in 27 patients
Source: CG Oncology, Inc. (2025). New Cretostimogene Grenadenorepvec Data Highlight its Potential to Become the Backbone Therapy for High-Risk Non-Muscle Invasive Bladder Cancer [Press Release]
Related Content:
SUO 2025: Topline Results from BOND-003 Cohort P – A Multinational , Single-arm Study of Intravesical Cretostimogene Grenadenorepvec for Treatment of High-risk, Papillary-only, BCG-unresponsive NMIBC
Cohort P Data from the BOND-003 Study in BCG-Unresponsive Papillary Bladder Cancer - Mark Tyson
SUO 2025: First Results from CORE-008 Cohort A – A Phase 2 Study of Intravesical Cretostimogene Grenadenorepvec in Patients with High-risk, BCG-naïve, NMIBC
SUO 2025: Reducing Over Detection in Prostate Cancer: The Case for Reflex Biomarkers
- Details
(UroToday.com) The 2025 SUO annual meeting featured a state-of-the-art session on reducing over-detection in prostate cancer and a presentation by Dr. Jeffrey Tosoian discussing the case for reflex biomarkers. To begin, Dr. Tosoian acknowledges that a pre-biopsy MRI absolutely improves the detection of clinically significant prostate cancer. According to data from Ahdoot et al.1 and the body of literature, a combination of systematic and targeted biopsies leads to a 6-13% absolute increase in clinically significant prostate cancer detection. However, there are two important considerations for reflex biomarker testing:
- There are critical limitations of MRI as a rule-out test
- There is excellent rule-out accuracy of biomarkers
SUO 2025: Reducing Over Detection in Prostate Cancer: The Case for Reflex Imaging
- Details
(UroToday.com) The 2025 SUO annual meeting featured a state-of-the-art session on reducing over-detection in prostate cancer and a presentation by Dr. Peter Pinto discussing the case for reflex imaging, and why MRI, and emerging imaging tools, should guide first-line diagnostic pathways in prostate cancer.
SUO 2025: INLEXZO™ Monotherapy in Patients with BCG-unresponsive Papillary Disease-only, High-risk NMIBC: 1-year Disease-free Survival Results from SunRISe-1
- Details
(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a bladder cancer late-breaking abstract (LBA) session. Dr. Siamak Daneshmand presented the 1-year disease-free survival (DFS) results from SunRISe-1 evaluating the gemcitabine intravesical system (Gem-iDRS), INLEXZO™ (gemcitabine intravesical system; formerly TAR-200), as monotherapy in patients with BCG-unresponsive, papillary-only, high-risk, non-muscle invasive bladder cancer (NMIBC).
SUO 2025: Systemic Therapy & Defining MRD in Metastatic Urothelial Carcinoma
- Details
(UroToday.com) Minimal residual disease (MRD) is an area of significant interest in urothelial carcinoma, particularly with the emergence of ctDNA-based assays capable of detecting molecular disease long before visible radiographic recurrence. In this SUO 2025 presentation, Dr. Parminder Singh reviewed the evolving definitions of MRD in metastatic urothelial carcinoma, the biologic and analytic foundations of ctDNA detection, and the rapidly expanding body of clinical evidence supporting ctDNA as a prognostic, predictive, and potentially actionable biomarker across localized and advanced disease.
MRD refers to the presence of residual cancer following definitive therapy, detected through cellular, biomarker-based, or molecular evidence that remains undetectable to standard imaging or direct visualization.1 In urothelial carcinoma, ctDNA-based MRD detection represents the most mature and clinically applicable approach. Assays fall into two broad categories:
- Tumor-informed assays: requiring prior tumor tissue sequencing to generate personalized mutation panels. These assays typically offer higher sensitivity, making them most suitable for post-operative MRD detection and surveillance.
- Tumor-uninformed (tumor-agnostic) whole-genome sequencing (WGS) assays: enabling broader mutation detection and sometimes guiding precision-medicine strategies, though often with lower sensitivity for low-burden disease.
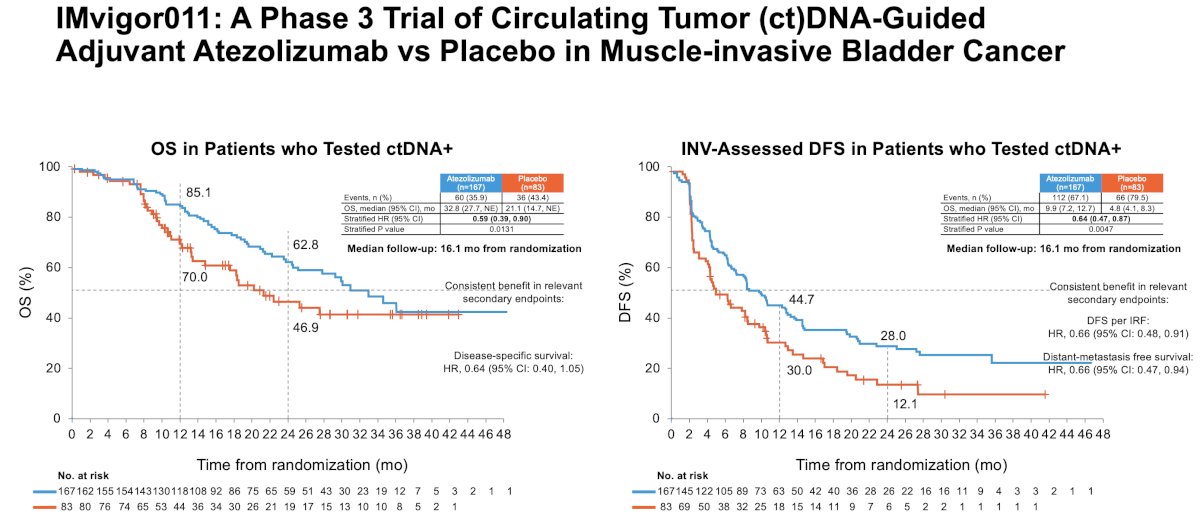
IMvigor011 is a global, randomized phase III trial that evaluated ctDNA-guided adjuvant atezolizumab versus placebo in patients with muscle-invasive urothelial carcinoma after radical surgery.3 Only patients who tested ctDNA-positive after surgery were randomized, providing the first large-scale evaluation of treatment selection based on molecular MRD status.
With a median follow-up of 16.1 months, ctDNA-positive patients treated with atezolizumab experienced significantly superior outcomes across multiple endpoints. Investigator-assessed disease-free survival curves demonstrated clear early separation, with durable benefit maintained over time (HR: 0.64, 95% CI: 0.47–0.87, p=0.0047). The OS curves similarly favored atezolizumab (median: 33 vs 21 months; HR: 0.59, 95% CI: 0.39–0.90, p=0.013). Other secondary endpoints similarly favored adjuvant atezolizumab in ctDNA+ patients:
- Distant metastasis-free survival: HR=0.66 (95% CI: 0.47–0.94)
- DFS per independent review: HR=0.66 (95% CI: 0.48–0.91)
- Disease-specific survival: HR=0.64 (95% CI: 0.40–1.05)
In contrast, ctDNA-positive patients receiving placebo had high and early recurrence rates, underscoring the prognostic significance of molecularly detectable MRD.
IMvigor011 participants who persistently tested ctDNA-negative during serial monitoring experienced favorable outcomes, with >95% DFS and OS at ~22 months post-cystectomy. Only a small fraction (4.2%) recurred during the surveillance phase, underlining the importance of ctDNA-negative status for identifying a ‘truly low-risk’ population.
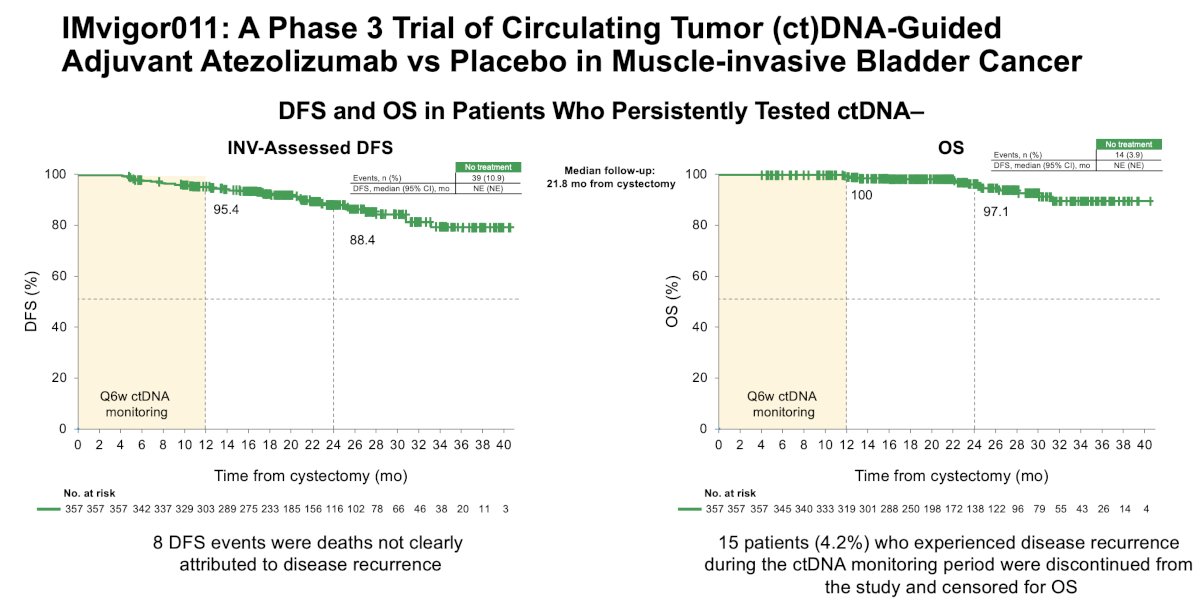
Notably, 8 DFS events in the ctDNA-negative cohort were deaths not clearly attributable to cancer recurrence, highlighting the need for careful adjudication of events in MRD-focused trials.
CheckMate 274: Post-hoc ctDNA AnalysesAdditional insight into the significance of ctDNA in the muscle-invasive urothelial carcinoma adjuvant setting comes from CheckMate 274, the landmark phase III trial of adjuvant nivolumab therapy.3 While ctDNA was evaluable in only 133 of the 709 randomized patients (19%), the findings were significant: baseline ctDNA detectability strongly correlated with worse DFS (52.1 vs 5 months; HR: 0.30, 95% CI: 0.18–0.48) and OS (not reached vs 28.2 months; HR: 0.44, 95% CI: 0.25–0.76). Patients with undetectable ctDNA had >10-fold longer median DFS than those with detectable ctDNA.
These post hoc analyses were limited by sample collection feasibility and small evaluable numbers, but they consistently reinforced the value of ctDNA as a powerful prognostic biomarker.

Dr. Singh then reviewed data from Sumiyoshi et al., which demonstrated the value of ctDNA fraction as a surrogate for tumor burden and its ability to reflect the impact of prior metastasectomy.4 ctDNA mutations showed substantial but incomplete concordance with tissue biopsies; 50.2% of mutations were shared between ctDNA and tumor tissue, while 17.6% and 32.2% were exclusive to ctDNA or tissue, respectively. These findings highlight the ability of ctDNA to capture clinically relevant mutational heterogeneity that may be missed by single-site tissue sampling.
Moreover, increases in ctDNA fraction consistently correlated with poor outcomes. In pembrolizumab-treated patients, increases or lack of decline in ctDNA were associated with significantly worse PFS and OS (both p<0.001), and substantially lower objective response rates⁵. These data suggest that early ctDNA kinetics may provide a timely indicator of immunotherapy response or resistance.

Whether ctDNA dynamics vary by treatment class remains a topic of ongoing investigation. Early data suggest that immune checkpoint inhibitors produce more variable ctDNA responses than chemotherapy, potentially reflecting delayed tumor clearance or immune-related fluctuations. In an exploratory analysis of KEYNOTE-36, ctDNA profiling demonstrated its ability to serve as a tumor tissue surrogate for genomic stratification and outcome prediction under pembrolizumab-based therapy.⁶

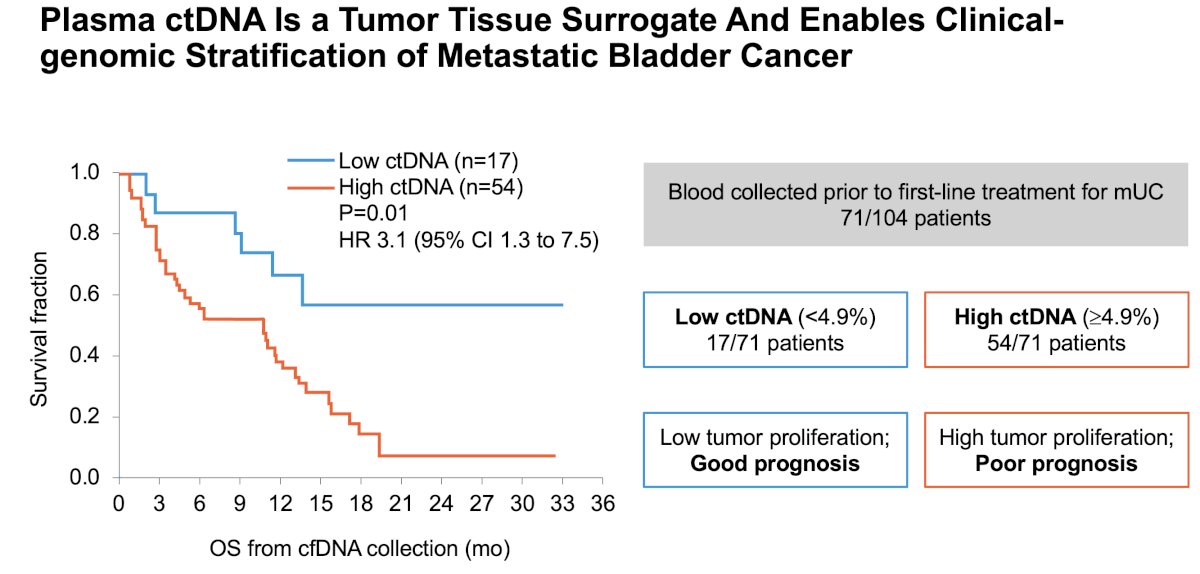
Baseline ctDNA as a Prognostic and Predictive Marker
Multiple studies have shown that high baseline ctDNA levels are linked with worse outcomes in metastatic urothelial carcinoma. Vandekerkhove et al. demonstrated that patients with high ctDNA had markedly worse OS (HR 3.1; 95% CI 1.3–7.5).7
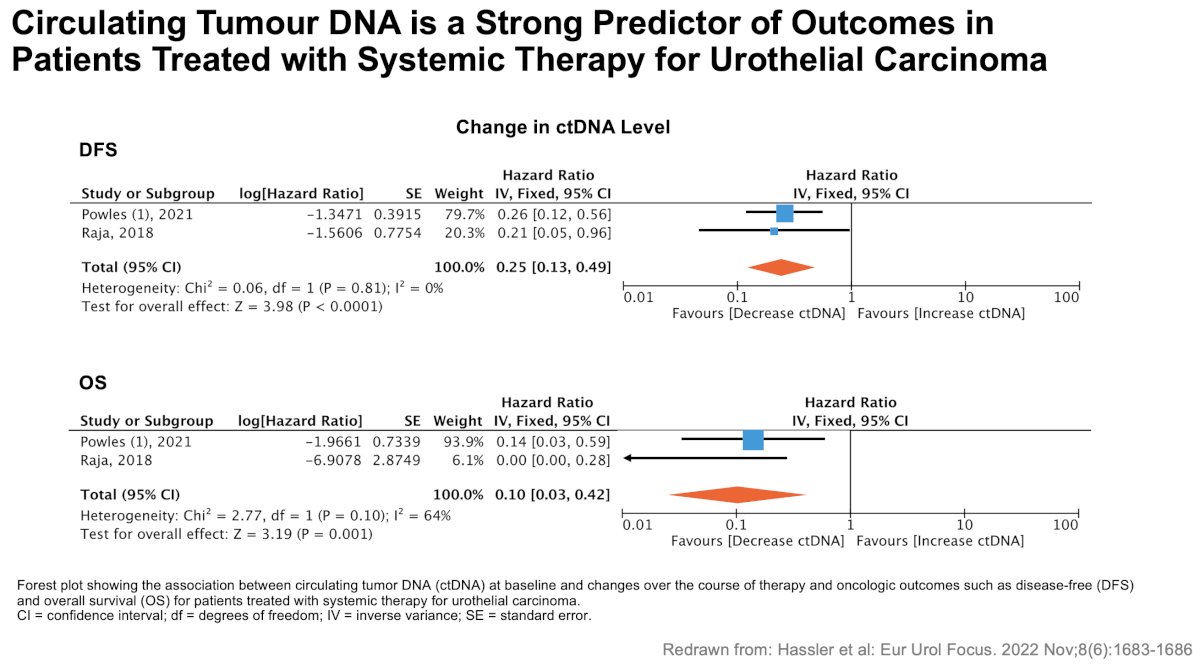
Hassler et al. further showed that both baseline ctDNA status and changes over treatment strongly correlated with DFS and OS across systemic therapies, supporting ctDNA as an independent prognostic marker.8
Dr. Singh highlighted four potential applications of ctDNA in advanced urothelial carcinoma:
- Prognosis — stratifying patients into high- and low-risk categories
- Predictive value — potentially guiding treatment selection (e.g., chemotherapy vs immunotherapy)
- Therapy escalation/de-escalation — MRD-positive patients may benefit from intensification, whereas MRD-negative patients may avoid unnecessary treatment
- Genomic evolution — ctDNA enables monitoring of emerging resistance mechanisms and identification of new therapeutic targets
As ctDNA technologies mature, prospective ctDNA-guided trials—similar to IMvigor011—will be essential to validate how MRD detection and kinetics should influence patient management in both localized and metastatic urothelial carcinoma. Further work is needed to define optimal testing intervals, thresholds for clinical action, and integration with imaging and clinical assessment.
Presented by: Parminder Singh, MD, Department of Internal Medicine, Mayo Clinic Arizona, Phoenix, AZ
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, December 2nd–5th, 2025
References:- Alvarez J, Patel VG, Singla N, et al. Minimal residual disease in urothelial carcinoma: Definitions and emerging biomarkers. Urol Oncol. 2024; 42:113-121.
- Powles T, Kann AG, Davarpanah NN, et al. IMvigor011: A phase III trial of ctDNA-guided adjuvant atezolizumab in muscle-invasive bladder cancer. ESMO 2025 Congress.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Long-term outcomes of adjuvant nivolumab in high-risk muscle-invasive urothelial carcinoma: ctDNA exploratory analyses from CheckMate 274. J Clin Oncol. 2024; 42:1105-1115.
- Sumiyoshi T, Sakamoto N, Fukumoto K, et al. Genomic heterogeneity captured through cfDNA in metastatic urothelial carcinoma. JCO Precis Oncol. 2025; 9:e2400472.
- Mehra R, Pal SK, Agarwal N, et al. ctDNA kinetics and outcomes with pembrolizumab in advanced urothelial carcinoma. Cancer. 2024; 130:2110-2120.
- Grivas P, Plimack ER, Petrylak DP, et al. KEYNOTE-361 exploratory ctDNA analyses: Genomic stratification and dynamic changes under pembrolizumab-based therapy. Nat Med. 2024; 30:2508-2516.
- Vandekerkhove G, Lavoie JM, Annala M, et al. Prognostic significance of baseline ctDNA in metastatic bladder cancer. Nat Commun. 2021; 12:184.
- Hassler MR, Hjorth L, Filipovic A, et al. ctDNA as a predictor of survival in urothelial carcinoma receiving systemic therapy. Eur Urol Focus. 2022; 8:1683-1686.
SUO 2025: First Results from CORE-008 Cohort A – A Phase 2 Study of Intravesical Cretostimogene Grenadenorepvec in Patients with High-risk, BCG-naïve, NMIBC
- Details
(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a bladder cancer late-breaking abstract (LBA) session. Dr. Trinity Bivalacqua presented the first results from CORE-008 Cohort A, a phase II trial of intravesical Cretostimogene Grenadenorepvec in patients with high-risk (HR), BCG-naïve, non-muscle invasive bladder cancer (NMIBC).
SUO 2025: Joseph A. Smith, Jr. Mentorship Award Lecture: Level 5 Mentorship - Moving from Transaction to Transformation
- Details
(UroToday.com) The 2025 SUO annual meeting featured the Joseph A. Smith Mentorship Award Lecture, presented by Dr. Cheryl Lee, who discussed level 5 mentorship and moving from transaction to transformation. Dr. Lee started her presentation by highlighting that the pillars of academia are akin to a stool in that mentorship strengthens with each leg (clinical service, research, education, and administration). However, we rarely think about ways to enhance mentoring nor do we strive for transformation. As part of her presentation, Dr. Lee inserted anecdotes from colleagues she sees as level 5 mentors. The first is Dr. Jay Smith, asking him how he became one of the most important mentors to so many leaders. Dr. Smith’s responses were humble and as follows:
SUO 2025: Stratifying Risk in Active Surveillance for Prostate Cancer Using Decipher Genomic Classifiers and Gleason Grade Group
- Details
(UroToday.com) The 2025 SUO Annual Meeting featured a prostate cancer poster session where Anthony Zhang and colleagues presented a retrospective analysis evaluating whether the Decipher genomic classifier may improve risk stratification for men on active surveillance (AS) when combined with Gleason Grade Group (GG). The authors hypothesized that genomic risk could further differentiate progression patterns within the same GG and help personalize AS intensity.
SUO 2025: Topline Results from BOND-003 Cohort P – A Multinational , Single-arm Study of Intravesical Cretostimogene Grenadenorepvec for Treatment of High-risk, Papillary-only, BCG-unresponsive NMIBC
- Details
(UroToday.com) At the 2025 SUO Annual Meeting, Dr. Mark Tyson presented the topline data from BOND-003 Cohort P evaluating intravesical cretostimogene grenadenorepvec in a population of patients with high-risk, papillary-only, BCG-unresponsive NMIBC.
SUO 2025: Coronary Artery Plaque Progression After ADT in Men with Prostate Cancer: A Randomized Controlled Trial Comparing Relugolix Versus Leuprolide (REVELUTION)
- Details
(UroToday.com) The 2025 SUO annual meeting featured a prostate cancer session and a presentation by Dr. Sagar Patel discussing results of a randomized controlled trial comparing relugolix versus leuprolide, specifically assessing coronary artery plaque progression among men with prostate cancer.
SUO 2025: Validation of Multimodal and Image-Only Artificial Intelligence Digital Pathology-Based Biomarkers Using Multi-Institutional Real-World Data
- Details
(UroToday.com) The 2025 SUO annual meeting featured a prostate cancer session and a presentation by Dr. Rana McKay discussing validation of multimodal and image-only artificial intelligence digital pathology-based biomarkers using multi-institutional real-world data. Artificial intelligence digital pathology-based biomarkers are gaining adoption in clinical practice for their ability to practically and efficiently personalize patient care. At SUO 2025, Dr. McKay and colleagues further demonstrated the value of digital pathology through validation of:
SUO 2025: PSMAddition: Top Line Results from a Phase 3 Trial of ADT and ARPI +/- 177Lu-PSMA-617 in Patients with PSMA-Positive mHSPC
- Details
(UroToday.com) The 2025 SUO annual meeting featured a prostate cancer session and a late breaking abstract presentation by Dr. Scott Tagawa discussing top line results from PSMAddition, a Phase 3 Trial of ADT and ARPI +/- 177Lu-PSMA-617 in Patients with PSMA-Positive Metastatic Hormone Sensitive Prostate Cancer. The PSMA-targeted radioligand therapy 177Lu-PSMA-617 prolongs radiographic progression free survival with a manageable safety profile in patients with PSMA-positive metastatic castration-resistant prostate cancer (mCRPC) in post-taxane (VISION1) and taxane-naive (PSMAfore2) settings. PSMAddition is the first phase III study of targeted radioligand therapy in patients with mHSPC.
SUO 2025: The 2025 AUA Hematuria Guidelines: Overview of Recommendations and Risk Stratification
- Details
(UroToday.com) The 2025 SUO annual meeting featured a bladder cancer session and a presentation by Dr. Yair Lotan discussing an overview of recommendations and risk stratification from the 2025 AUA Hematuria Guidelines. Hematuria is one of the most common urologic diagnoses, with a prevalence of 6.5% (3.4 to 12.2%).
SUO 2025: Baseline Urinary Tumor DNA, Minimal Residual Disease and Genomic Disease Burden in Relation to Clinical Response to INLEXZO™ in the Phase 2b SunRISe-1 Trial
- Details
(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a bladder cancer poster session. Dr. Girish Kulkarni presented an ad hoc analysis of the phase 2b SunRISe-1 Trial evaluating baseline urinary tumor DNA (utDNA), minimal residual disease (MRD), and genomic disease burden in relation to clinical response to INLEXZO™ (gemcitabine intravesical system; formerly TAR-200).
SUO 2025: Development and Validation of a CHAI-based Biomarker to Prognosticate High Grade Progression risk in Low-Grade NMIBC
- Details
(UroToday.com) The 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix between December 2 and December 5, 2025, was host to the Poster Session. Dr. Roger Li presented poster #197: Development and Validation of a Computational Histology AI (CHAI)-based biomarker to Prognosticate High Grade Progression risk in Low-Grade Non-muscle Invasive Bladder Cancer.
SUO 2025: RECURxNCE-BCa – An Artificial Intelligence-Based Tool to Predict Recurrence in NMIBC and Comparison with Current Risk Stratification Tools for Intermediate-Risk Disease
- Details
(UroToday.com) The 2025 Society of Urologic Oncology (SUO) annual meeting, held in Phoenix between December 2 and December 5, 2025, was host to the Poster Session. Dr. Jethro Kwong presented poster #199: RECURxNCE-BCa – an artificial intelligence-based tool to predict recurrence in non-muscle invasive bladder cancer and comparison with current risk stratification tools for intermediate-risk disease.