(UroToday.com) The 2025 SUO annual meeting featured a prostate cancer session and a presentation by Dr. Sagar Patel discussing results of a randomized controlled trial comparing relugolix versus leuprolide, specifically assessing coronary artery plaque progression among men with prostate cancer.
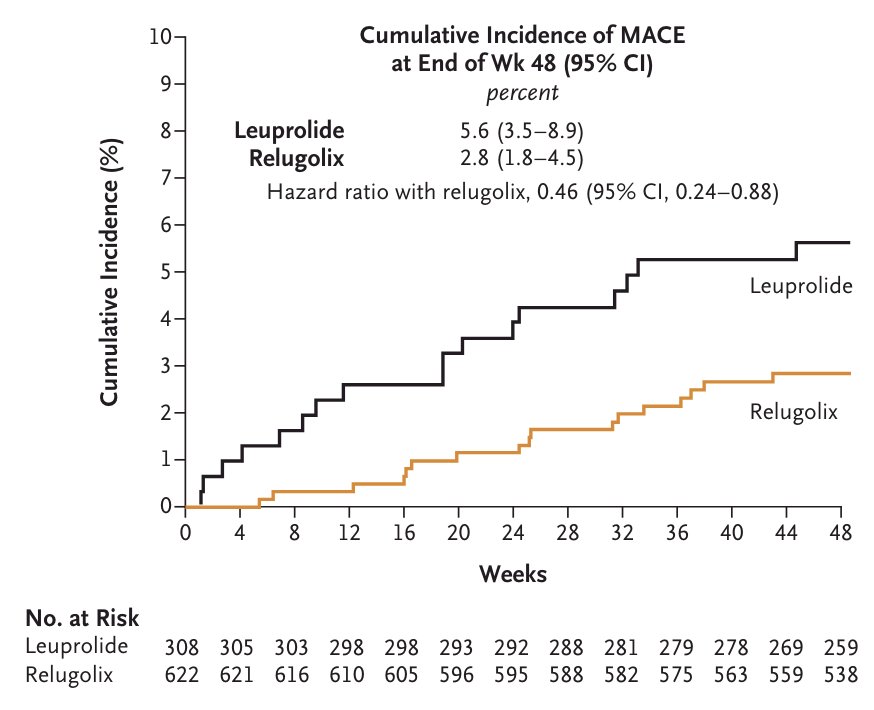
ADT for prostate cancer is associated with cardiovascular morbidity, yet the biological basis remains unclear. Recent studies have yielded conflicting results regarding the cardiovascular safety of gonadotropin-releasing hormone agonists versus antagonists. Previously, the HERO phase 3 trial1 showed a higher rate of major adverse cardiovascular events following leuprolide (5.6%) compared with relugolix:
Relugolix Versus Leuprolide Cardiac Trial (REVELUTION, NCT05320406) was designed to test the hypothesis that ADT-associated cardiovascular risk is mediated by accelerated coronary atherosclerosis and is more prominent with the gonadotropin-releasing hormone-agonist leuprolide compared with the gonadotropin-releasing hormone-antagonist relugolix.
This prospective three-arm trial enrolled men with treatment-naïve, localized prostate cancer pursuing pelvic radiotherapy alone or with concomitant ≥ 6 months ADT. Patients receiving ADT were randomized 1:1 to either leuprolide versus relugolix. Patients receiving radiotherapy alone without ADT served as a control. The trial design for REVELUTION is outlined as follows:
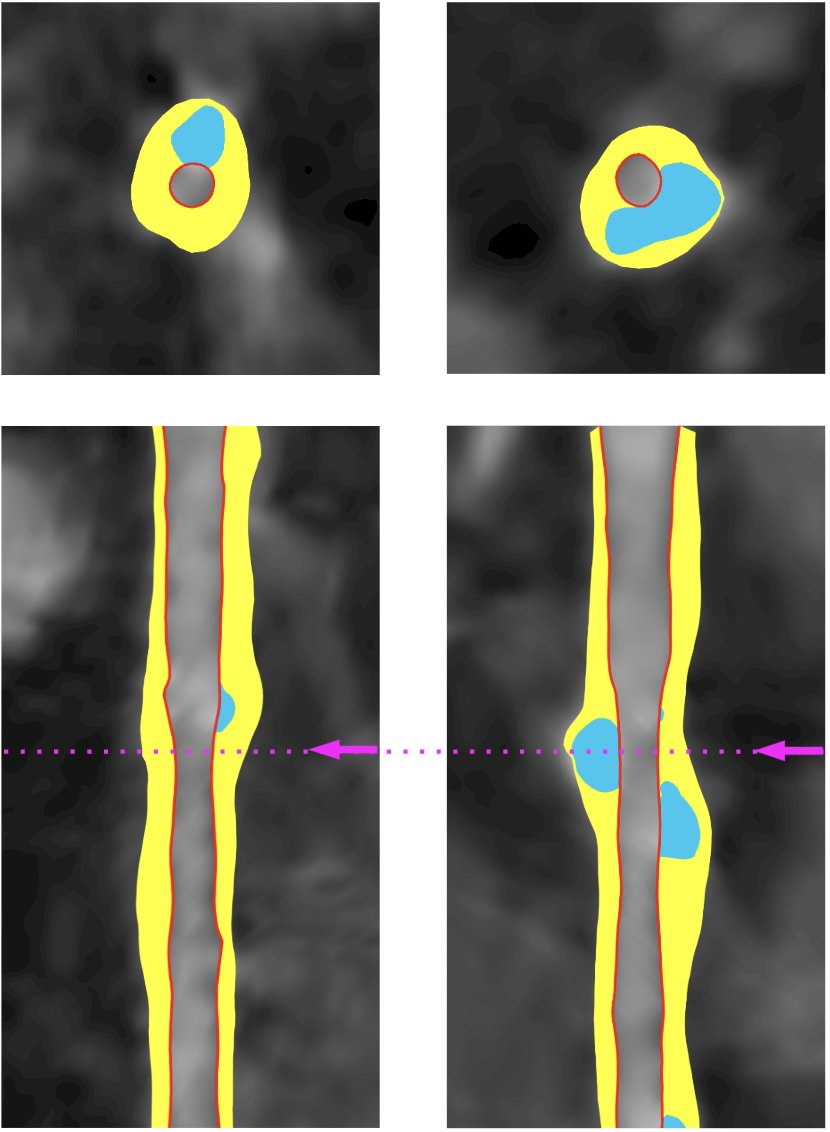
The primary endpoint was the change in total coronary artery plaque volume, measured by prospective coronary CT angiography completed at baseline and 12 months after treatment initiation. Other outcome measures included change in non-calcified plaque volume, calcified plaque volume, and low-attenuation plaque volume, as well as the incidence of major adverse cardiovascular events (stroke, myocardial infarction, coronary stent). The following figure highlights plaque assessment:
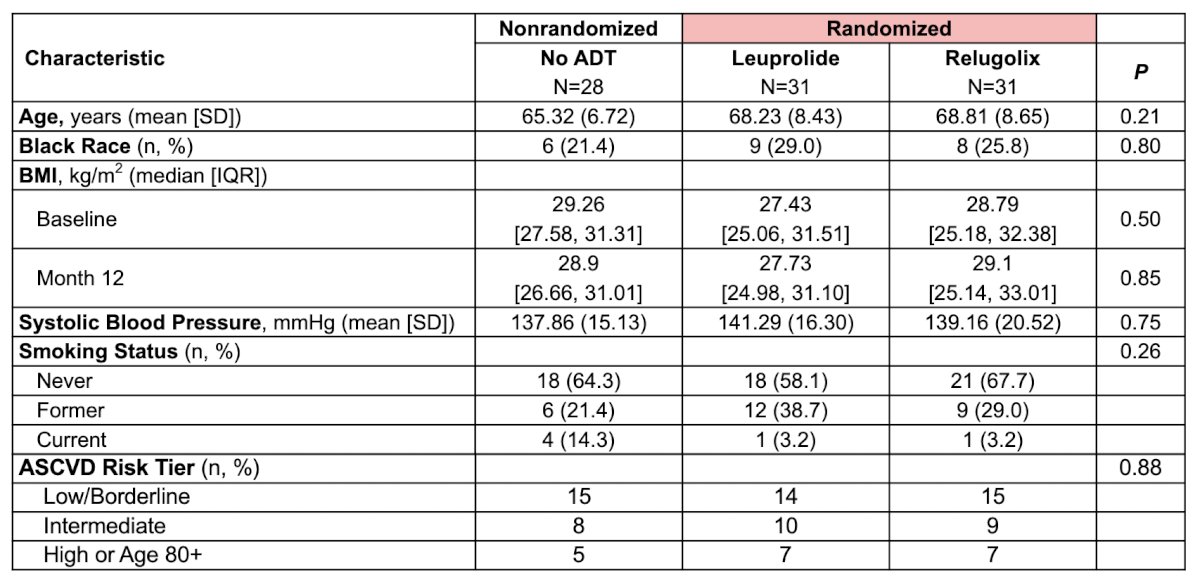
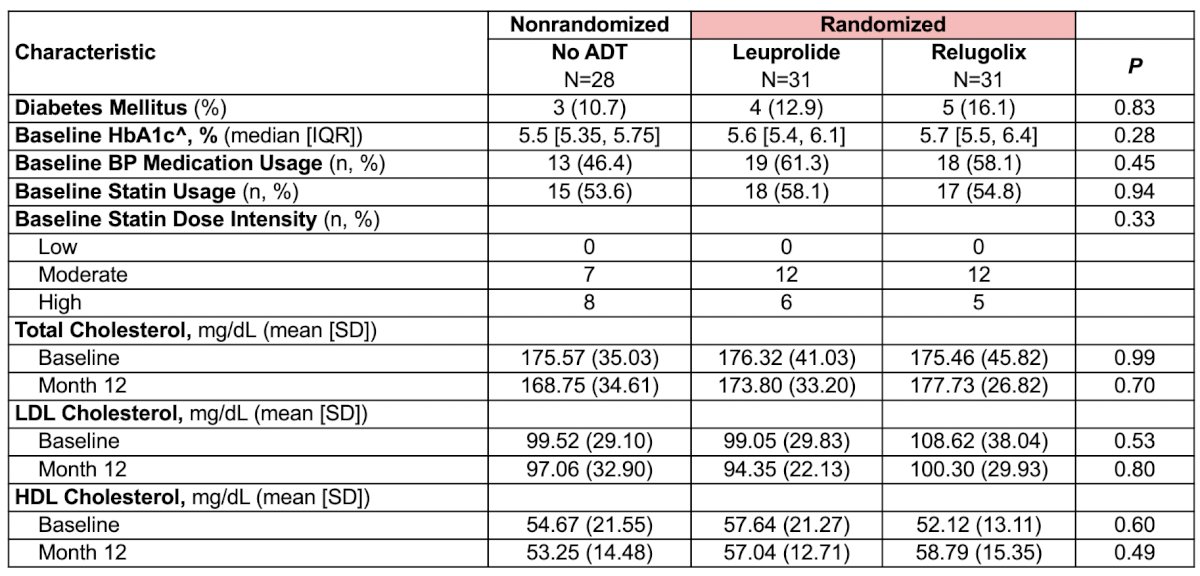
Of the 94 men enrolled from June 2022 to March 2024, 90 (28 radiotherapy alone, 31 radiotherapy + leuprolide, and 31 radiotherapy + relugolix) completed the study for analysis. The baseline characteristics were well balanced between the two groups:
The median change in total coronary artery plaque volume was higher (p = 0.02) with leuprolide (+52.0 [19.5-159.0] mm3) compared with relugolix (+25.0 [-6.0-46.0] mm3) and no ADT (+13.0 [-19.0-45.0] mm3). The 12-month change in coronary artery total plaque volume was +79.1 mm3 for leuprolide versus +10.5 mm3 for relugolix. Additionally, the 12-month change in coronary artery non-calcified plaque volume was +71.9 mm3 for leuprolide versus +7.2 mm3 for relugolix. Compared with no ADT, leuprolide was associated with a significantly greater increase in total coronary artery plaque volume (estimated difference +79.1 mm3, p = 0.004), non-calcified plaque volume (+71.9 mm3, p = 0.001), calcified plaque volume (calcified plaque volume +19.9 mm3, p = 0.04), and low-attenuation plaque volume (+5.1 mm3, p = 0.03) after adjusting for baseline plaque volume, age, and statin use. Compared with no ADT, relugolix did not result in a significant change in total coronary artery plaque volume (estimated difference +10.5 mm3, p = 0.69), non-calcified plaque volume (+7.2 mm3, p = 0.73), calcified plaque volume (+8.9 mm3, p = 0.34), or low-attenuation plaque volume (+1.3 mm3, p = 0.56):
![The median change in total coronary artery plaque volume was higher (p = 0.02) with leuprolide (+52.0 [19.5-159.0] mm3) compared with relugolix (+25.0 [-6.0-46.0] mm3) and no ADT (+13.0 [-19.0-45.0] mm3). The 12-month change in coronary artery total plaque volume was +79.1 mm3 for leuprolide versus +10.5 mm3 for relugolix. Additionally, the 12-month change in coronary artery non-calcified plaque volume was +71.9 mm3 for leuprolide versus +7.2 mm3 for relugolix. Compared with no ADT, leuprolide was associated with a significantly greater increase in total coronary artery plaque volume (estimated difference +79.1 mm3, p = 0.004), non-calcified plaque volume (+71.9 mm3, p = 0.001), calcified plaque volume (calcified plaque volume +19.9 mm3, p = 0.04), and low-attenuation plaque volume (+5.1 mm3, p = 0.03) after adjusting for baseline plaque volume, age, and statin use. Compared with no ADT, relugolix did not result in a significant change in total coronary artery plaque volume (estimated difference +10.5 mm3, p = 0.69), non-calcified plaque volume (+7.2 mm3, p = 0.73), calcified plaque volume (+8.9 mm3, p = 0.34), or low-attenuation plaque volume (+1.3 mm3, p = 0.56):](/images/com-doc-importer/241-suo-2025/suo-2025-coronary-artery-plaque-progression-after-adt-in-men-with-prostate-cancer-a-randomized-controlled-trial-comparing-relugolix-versus-leuprolide-revelution/image-5.jpg)
With a median follow-up of 23.3 (IQR 18.2-29.1) months, 3 patients (9.7%) in the leuprolide arm, 0 patients in the relugolix arm, and 1 patient (3.6%) in the no ADT arm experienced a major adverse cardiovascular event.
There are several clinical implications of these findings from REVELUTION, the first clinical trial to identify a biological basis of cardiovascular risk differences observed in the HERO trial. Leuprolide results in significant near-term coronary artery plaque progression, particularly non-calcified plaque volume, which is highly associated with major adverse cardiovascular events. This risk was not seen with relugolix. Additionally, there are peripheral GnRH/FSH-mediated pathways in the coronary endothelium, and immune effector responses can lead to plaque instability:2

Dr. Patel concluded his presentation discussing results of a randomized controlled trial comparing relugolix versus leuprolide and coronary artery plaque progression with the following take-home points:
- REVELUTION is the first clinical trial to identify a biological basis for cardiovascular risk differences observed between ADT drug pathways in men with prostate cancer
- GnRH-agonist leuprolide was associated with significant near-term coronary plaque progression, while GnRH-antagonist relugolix was not
- The total plaque volume increase is primarily driven by noncalcified plaque volume
- These results support the hypothesis that cardiovascular risk from ADT is, at least partly, driven by accelerated coronary atherosclerosis, which appears more prominent with leuprolide compared with relugolix
- This corroborates prior clinical data showing greater long-term major adverse cardiovascular event risk with gonadotropin-releasing hormone agonists
Presented by: Sagar Patel, MD, Emory University, Atlanta, GA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, Wed, Dec 3 – Fri, Dec 5, 2025.
Related content: Coronary Atherosclerosis Findings from the REVELUTION Trial of Leuprolide and Relugolix - Avirup Guha & Sagar Patel
References:
- Shore ND, Saad F, Cookson MS, et al. Oral Relugolix for Androgen-Deprivation Therapy in Advanced Prostate Cancer. N Engl J Med. 2020 Jun 4;382(23):2187-2196.
- Crawford ED, Schally AV, Pinthus JH, et al. The potential role of follicle-stimulating hormone in the cardiovascular, metabolic, skeletal, and cognitive effects associated with androgen deprivation therapy. Urol Oncol. 2017;35(5):183-191.