(UroToday.com) At the 2025 SUO Annual Meeting, Dr. Mark Tyson presented the topline data from BOND-003 Cohort P evaluating intravesical cretostimogene grenadenorepvec in a population of patients with high-risk, papillary-only, BCG-unresponsive NMIBC.
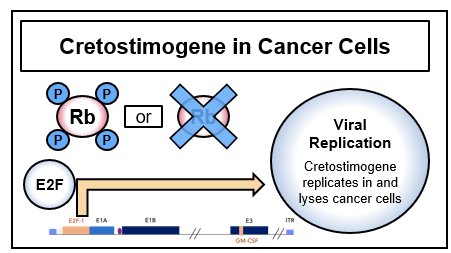
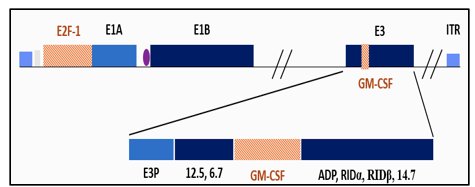
Cretostimogene grenadenorepvec is a conditionally replicating, highly immunogenic adenovirus driven by the E2F-1 human promoter, selectively targeting tumors with RB–E2F pathway alterations. The vector also encodes a GM-CSF transgene. As an oncolytic immunotherapy, it has dual mechanisms of action, producing direct tumor lysis through viral replication and stimulating tumor-directed immune activation.
Dr. Tyson noted that there remains a significant unmet need for clinically effective, well-tolerated bladder-sparing treatment options for patients with BCG-unresponsive, papillary-only NMIBC. The current FDA-approved agents for patients with high-risk, BCG-unresponsive NMIBC are specifically for those patients with CIS +/- papillary disease. However, patients commonly present with HG Ta/T1 NMIBC. The benchmarks reported from a recent meta-analysis for BCG-unresponsive papillary-only NMIBC are as follows:1
- 3 months: 73%
- 6 months: 58%
- 12 months: 48%

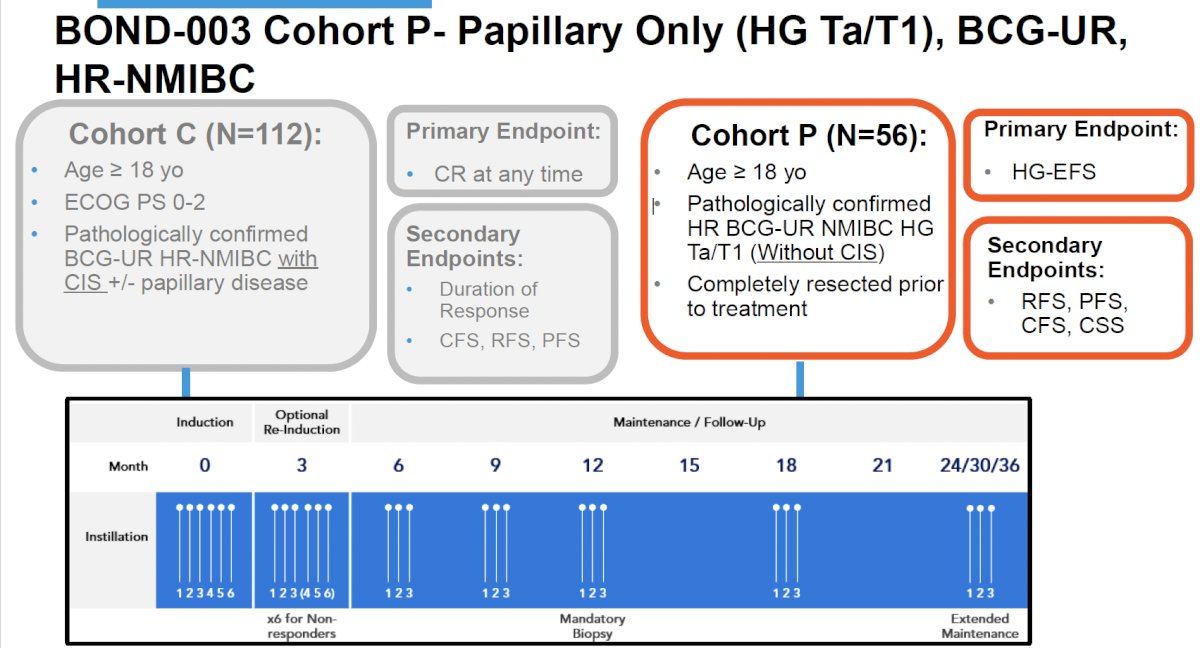
BOND-003 includes two primary cohorts. Cohort C (N=112) enrolled patients with BCG-unresponsive CIS ± papillary disease. Data from this cohort has been previously reported2 and demonstrated an overall complete response of 75.5%, with 12- and 24-month rates of 46.4% and 41.8%, respectively. 96.4% of patients were free from progression to MIBC, and 83.6% of patients did not undergo radical cystectomy post recurrence or progression. Among those patients who underwent a radical cystectomy post recurrence or progression, 83.3% (15/18) were T0 or NMIBC. There were no reported Grade ≥3 treatment-related adverse events (TRAEs) or death, and no treatment-related discontinuations.

Cohort P (N=56), the focus of this presentation, included patients aged ≥18 years with pathologically confirmed high-grade Ta/T1 BCG-unresponsive NMIBC without CIS. All patients underwent a complete resection prior to treatment. The primary endpoint for Cohort P was high-grade event-free survival (HG-EFS), with secondary endpoints including recurrence-free survival (RFS), progression-free survival (PFS), cystectomy-free survival (CFS), and cancer-specific survival (CSS).
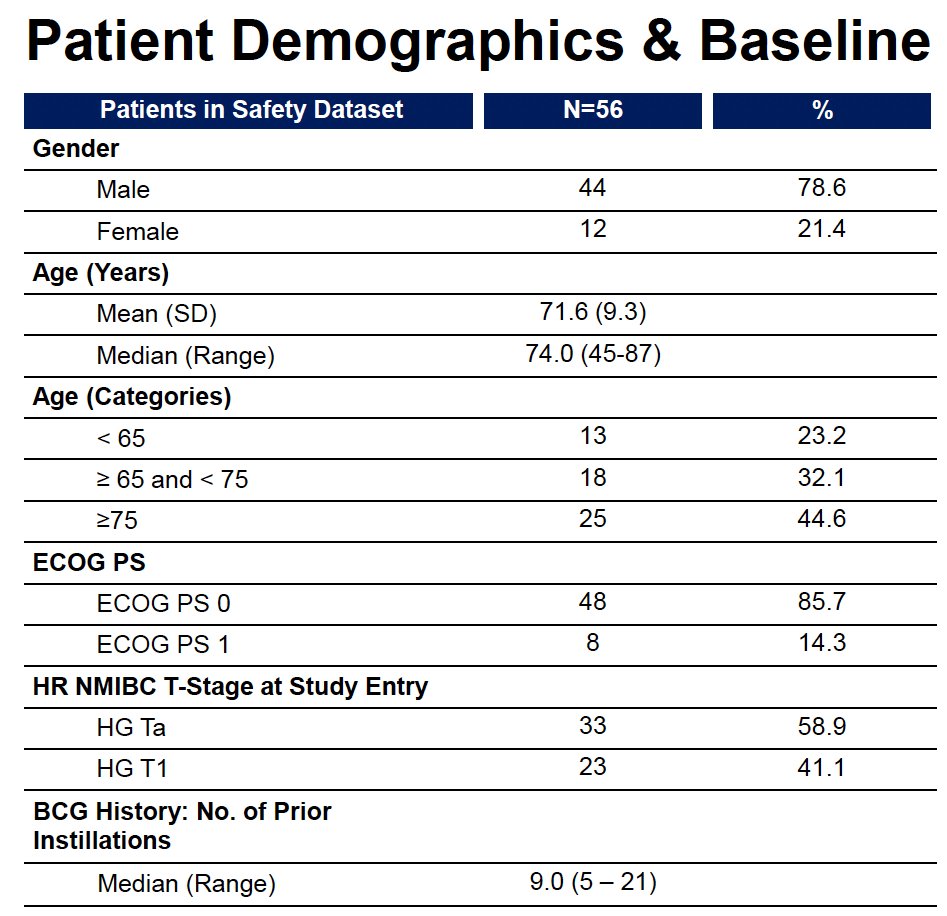
The baseline characteristics are summarized below. 78.6% of patients were male, 75% were older than 65 years, and 96.4% were treated in the United States. Forty-one percent had HG T1 disease at study entry, and the median number of prior BCG instillations was 9. This reflects a high-risk population consistent with real-world BCG-unresponsive papillary disease.
With a median follow-up of 6 months, Cohort P demonstrated consistent and high HG-EFS rates:
- HG Ta:
- 3 months: 92.8%
- 6 months: 75.9%
- 9 months: 75.9%
- HG T1:
- 3 months: 100%
- 6 months: 100%
- 9 months: 87.5%
The Kaplan–Meier–estimated HG-EFS across the entire cohort showed 95.7% at 3 months (95% CI 83.8–98.9), 84.6% at 6 months (95% CI 68.6–92.9), and 80.4% at 9 months (95% CI 62.3–90.4). Eight patients underwent re-induction.

Notably, no patients in the cohort underwent radical cystectomy during the follow-up period, and no progression to muscle-invasive disease was observed. One patient progressed to metastatic urothelial carcinoma despite achieving a clinical complete response in the bladder.
Safety findings were favorable, with most TRAEs being Grade 1–2. There were no Grade ≥3 TRAEs, serious TRAEs, deaths, dose delays, or treatment discontinuations. A total of 98.2% of patients received all protocol-defined treatments. The most common TRAEs were bladder spasms (46.4%), dysuria (39.3%), pollakiuria (25%), and urgency (19.6%).

Dr. Tyson concluded his presentation of the late-breaking results from BOND-003 Cohort P, as follows:
- Topline results with cretostimogene in BOND-003 Cohort P consistently demonstrate
- Strong HG-EFS at 3, 6, and 9 months
- Responses are maintained across HG Ta and the higher-risk HGT1 populations
- This intravesical regimen has a well-tolerated safety profile
- Longer-term treatment and follow up ongoing
Presented by: Mark Tyson, MD, MPH, Associate Professor, Department of Urology, Mayo Clinic, Phoenix, AZ
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
Related content: Cohort P Data from the BOND-003 Study in BCG-Unresponsive Papillary Bladder Cancer - Mark Tyson
References:
- Rose KM, Smith A, Johnson B, et al. High-risk papillary non–muscle invasive bladder cancer outcomes following BCG-unresponsive disease: A systematic analysis. SIUJ. 2022; 3(5):333-339.
- UroToday. Updated clinical-translational results from BOND-003 Cohort C: a phase 3 single-arm study of intravesical cretostimogene grenadenorepvec for high-risk BCG-unresponsive NMIBC with CIS. UroToday. 2025. https://www.urotoday.com/conference-highlights/eau-2025/eau-2025-bladder-cancer/159231-eau-2025-updated-clinical-translational-results-bond-003-cohort-c-a-phase-3-single-arm-study-of-intravesical-cretostimogene-grenadenorepvec-for-high-risk-bcg-unresponsive-nmibc-with-cis.html