(UroToday.com) The 2025 SUO annual meeting featured the Huggins Medal Lecture and presentation by this year’s recipient, Dr. Peter Carroll, discussing “What I did and What I am Doing”. Important themes in his presentation consisted of people (teams), data (information), and practice. As an editorial note, Dr. Carroll stated that “When I say I, I mean we. When I say we, I mean they.”
Dr. Carroll began by acknowledging the mentors who shaped his trajectory, particularly his formative years as a urologic oncology fellow at MSKCC in the mid-1980s. These early relationships carried forward into his decades at UCSF, where the scale of faculty and collaborators underscored the department’s growth into a modern powerhouse in clinical research, population science, health services work, and translational oncology. Dr. Carroll emphasized that nothing he accomplished was possible without teams that expanded capacity, expertise, and imagination.
One of the defining contributions of Dr. Carroll’s career was the early construction of urologic oncology data infrastructure. He recognized early that progress in prostate cancer required broad, linked datasets that captured clinical variables, tissue specimens, patient-reported outcomes, and longitudinal care patterns. The UCSF tissue bank ultimately amassed >9,000 specimens, including FFP, frozen tissue, urine, and blood. He also created two key registries:
- CaPSURE, a national prostate cancer registry covering 40 sites and >15,000 men, and ~1,000 variables
- UODB (Urologic Oncology Database) at UCSF, comprising 9,973 patients and ~500 variables, linked directly to the tissue bank
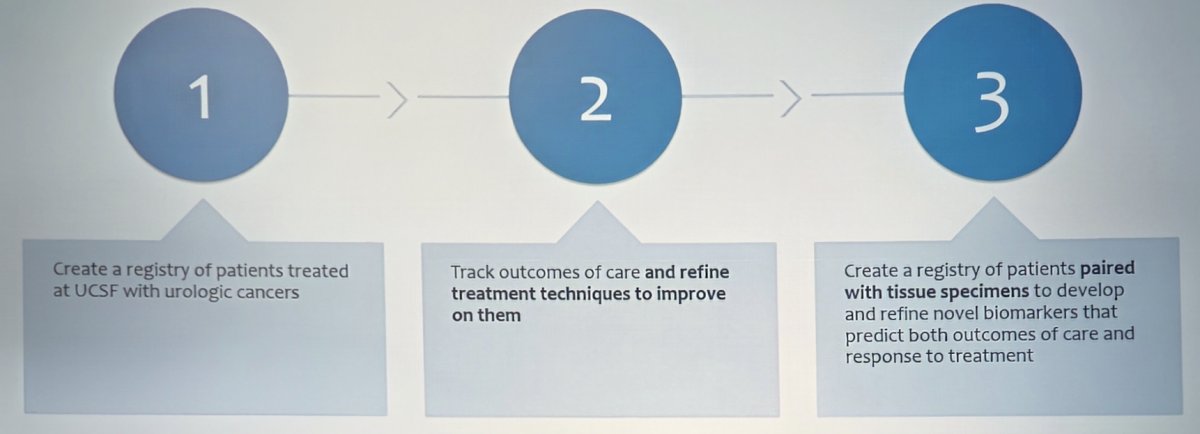
Dr. Carroll outlined the core objectives of the Urologic Oncology Database:
- Create a registry of patients treated at UCSF with urologic cancers
- Track outcomes of care to refine treatment techniques and improve them
- Pair clinical data with tissue specimens to develop biomarkers predictive of outcomes and treatment response
The Urologic Oncology Database matured into one of the most productive institutional registries in the field. The evolution included manual paper chart review, followed by manual EMR review, followed by automated EMR abstraction (in 2018). Dr. Carroll noted the next frontier: leveraging large language models to extract structured clinical data from EMRs, particularly in systems with large, heterogeneous medical records.
Dr. Carroll notes that we can learn a lot from what we have readily available if we use it. For this example, he discussed the UCSF CAPRA (Cancer of the Prostate Risk Assessment) Score, spearheaded by Dr. Matt Cooperberg. This tool remains among the most validated risk stratification tools in prostate cancer, built using readily available clinical variables, such as PSA, Gleason grade, T-stage, percent positive cores, and age:
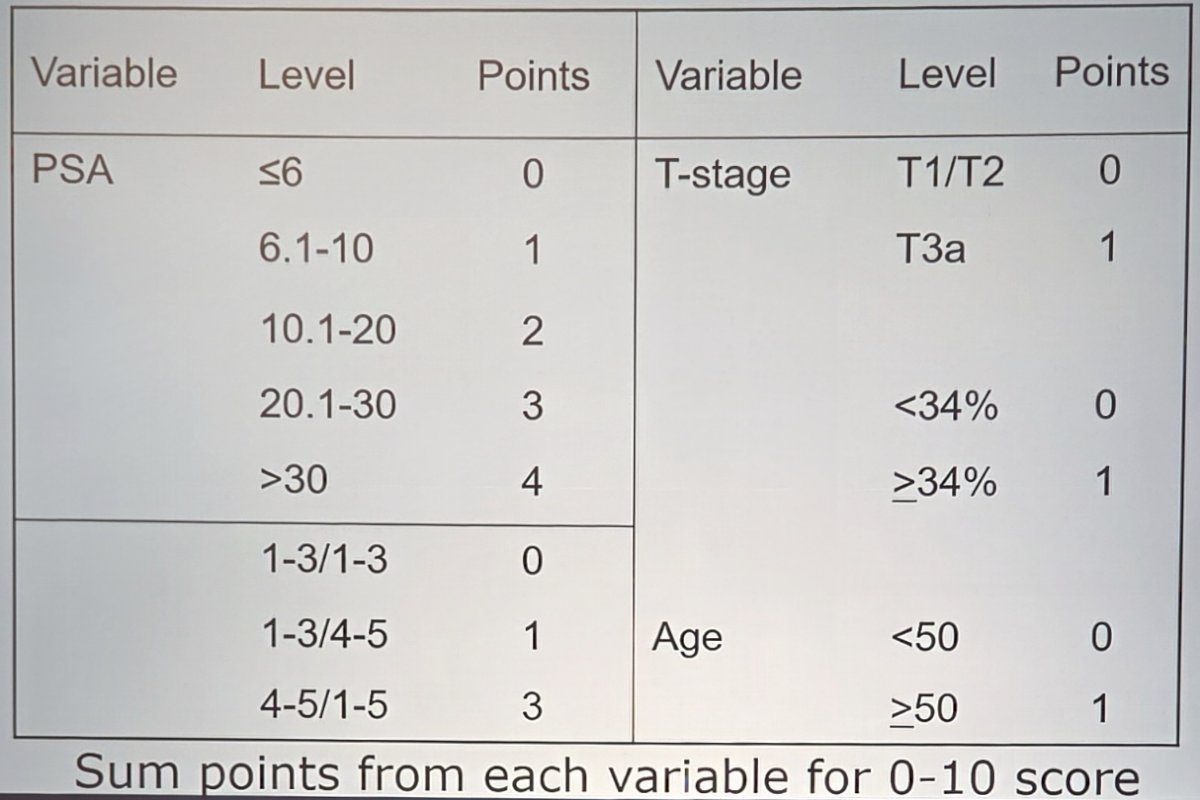
CAPRA developed strong discrimination for both cancer-specific survival (c-index = 0.80) and overall survival (c-index = 0.71), becoming the benchmark against which novel biomarkers are evaluated. How can we improve on CAPRA? Several molecular biomarkers have emerged, including Decipher, Prolaris, and Oncotype, in addition to the integration of mpMRI and PSMA PET into contemporary prostate cancer practice.
When discussing contemporary clinical science, Dr. Carroll highlighted the social vulnerability index and prostate cancer outcomes, work led by Dr. Sam Washington. Among individuals living in communities above the 75th percentile for social vulnerability nationally, this is associated with:
- 3.35x greater odds of receiving ADT monotherapy
- Lower use of active surveillance and watchful waiting for low-risk disease (versus surgery or radiation: OR 0.5, 95% CI 0.34-0.72)
- Less likelihood of receiving definitive local therapy (OR 0.77, 95% CI 0.63-0.94)
- Greater odds of meaningful declines in sexual function and post-treatment outcomes (OR 0.35, 95% CI 0.16-0.73 for decline in function or bother)
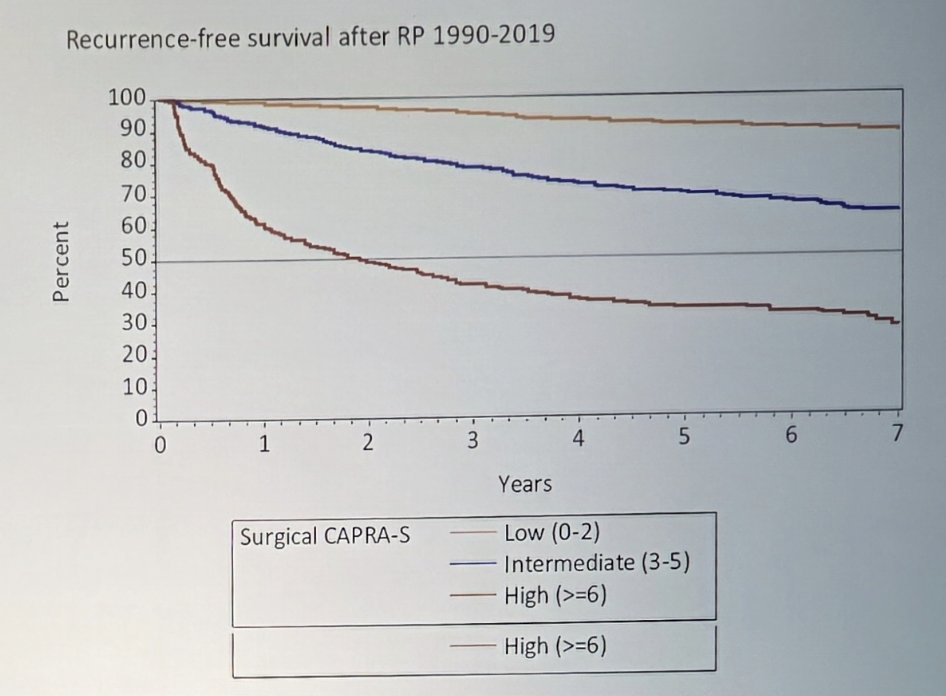
Dr. Carroll emphasized that it is important for clinicians (and specifically surgeons) to know their outcomes, learn from them, and be able to counsel patients and colleagues transparently:
UCSF was one of the earliest adopters of active surveillance. Today, the AUA, EAU, NCCN, etc, agree that low-risk prostate cancer should be managed with surveillance. Recently, there has been an ongoing debate around labeling Gleason Grade Group 1 (GG1) as “cancer.” While GG1 carries very low metastatic potential, Dr. Carroll noted that upgrading does occur, and active surveillance is not a “no follow-up” strategy. The goal remains to understand which men harbor indolent disease and which are at risk for meaningful progression.
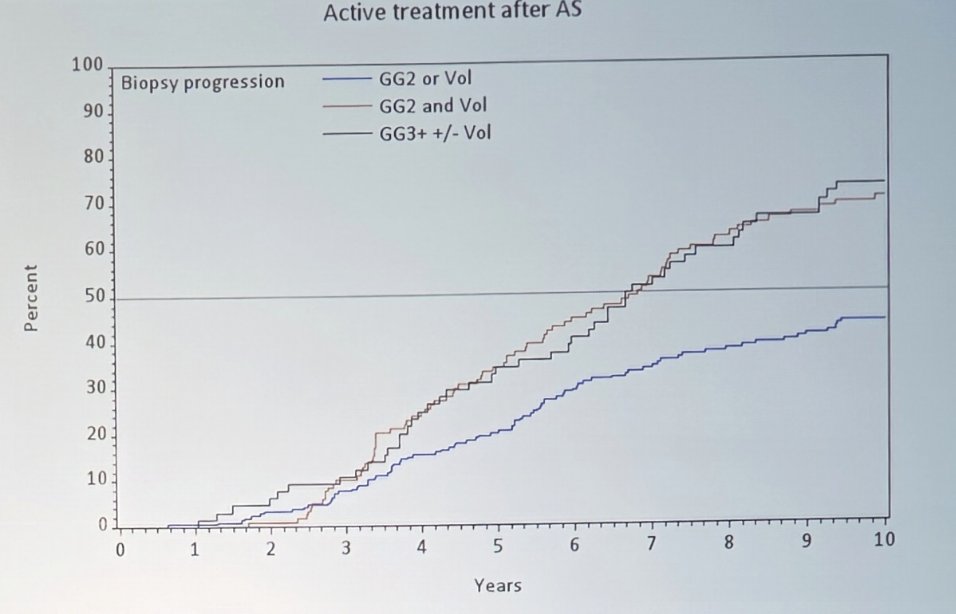
In a UCSF Urologic Outcomes Database study, Dr. Carroll’s team queried the database for men with cT1-2N0/xM0/x, PSA < 20 ng/mL, GG1 prostate cancer with <= 33% of the biopsy core positive, and with a minimum of 2 biopsies on active surveillance with at least one of the biopsies being mpMRI targeted. The outcomes included: any upgrading (GG2+), major upgrading (GG3+), an increase in the percentage of positive cores to >33%, and progression to active treatment.
Over a median follow-up of 114 months (IQR 75-157), men with GG1 on active surveillance who had a positive MRI-targeted biopsy had high rates of upgrading, moderate rates of increased core positivity and progression to active treatment, and low rates of major upgrade on subsequent biopsy. Additionally, there were low absolute rates of metastasis (1.9%). Patients with minor upgrade (GG2) and increased core positivity, and patients with major upgrade (GG3+) were more likely to progress to active treatment compared to patients with minor upgrade or increased core positivity alone (log-rank p < 0.01). Only patient age was associated with major upgrading, and high genomic risk was associated with upgrading, but not major upgrading. MRI positivity was not associated with any active surveillance outcomes.
Life table estimates for outcomes at 10 years are as follows:
- Any upgrading: 62%
- Increase in percent positive cores >50%: 34%
- Disease progression (either upgrade or percent positive cores >50%): 72%
- Development of intraductal carcinoma or EC: 47%
- Progression to active treatment: 65%
- Metastasis: 3.3%
Dr. Carroll highlighted the following stacked bar graph showing CAPRA risk profiles for men undergoing radical prostatectomy at UCSF over time. Early years were predominantly low-risk cases, but over time, the distribution shifted to high-risk and select intermediate-risk disease patients comprising the majority of surgical volume:
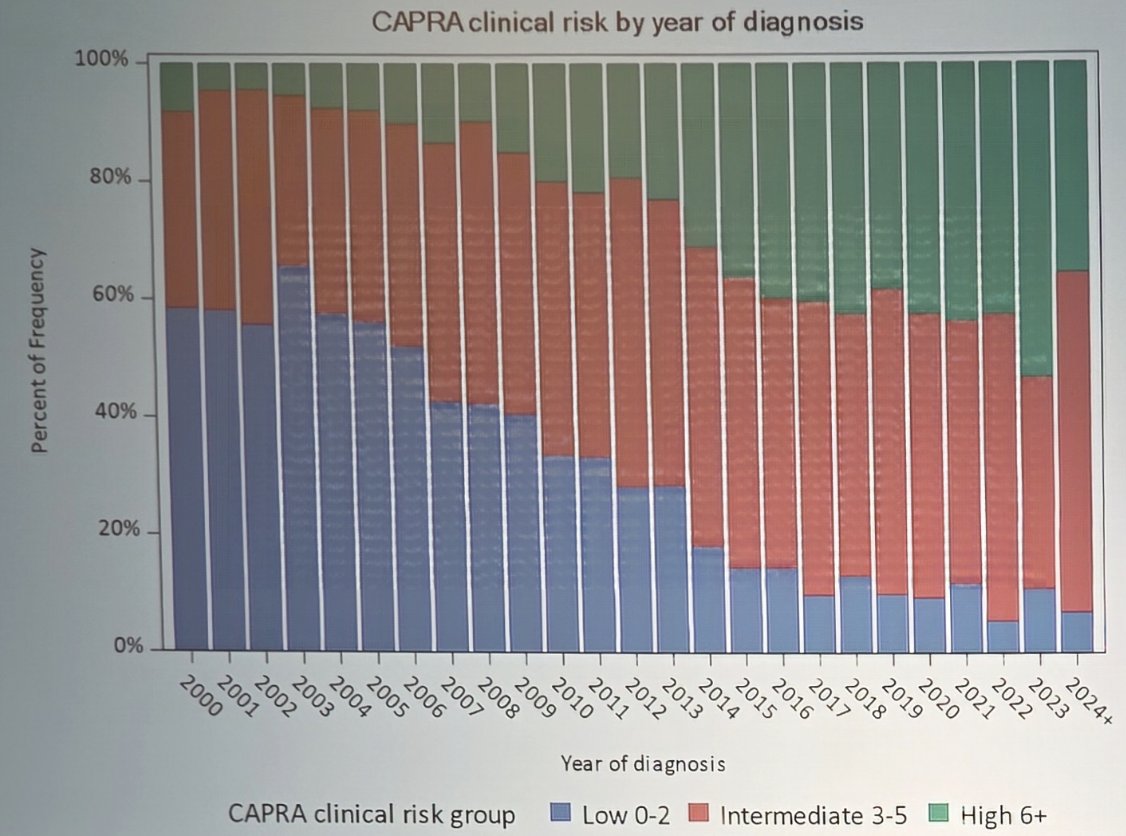
Thus, he notes that we should only operate on those who truly benefit.
Research and education are underfunded mandates, so Dr. Carroll developed a financial model that facilitated success, recruiting and retaining successful scientists, and understanding the role of philanthropy. Collaboration is also a catalyst for success, noting successful collaborations for CANARY – Pass, Movember GAP3, Loss of Y chromosome, and CEASAR:
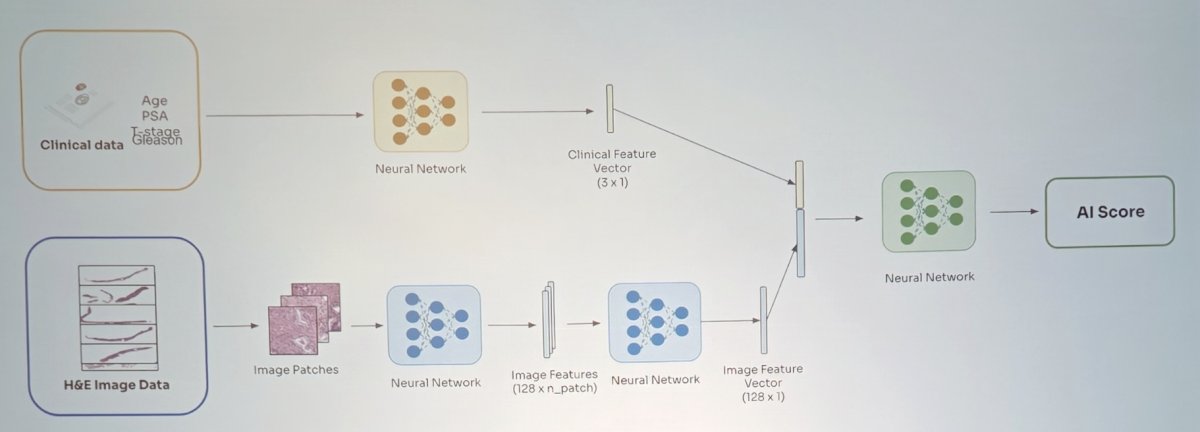
Discussing work presented at SUO 2025, Dr. Carroll highlighted Dr. McKay’s abstract presentation assessing validation of multimodal and image-only artificial intelligence digital pathology-based biomarkers using multi-institutional real-world data. This study further demonstrated the value of digital pathology through validation of:
- A multimodal artificial intelligence biomarker utilizing digital pathology images and key clinical variables (age, PSA, T-stage)
- A newly developed “image-only” artificial intelligence biomarker utilizing only digital pathology images
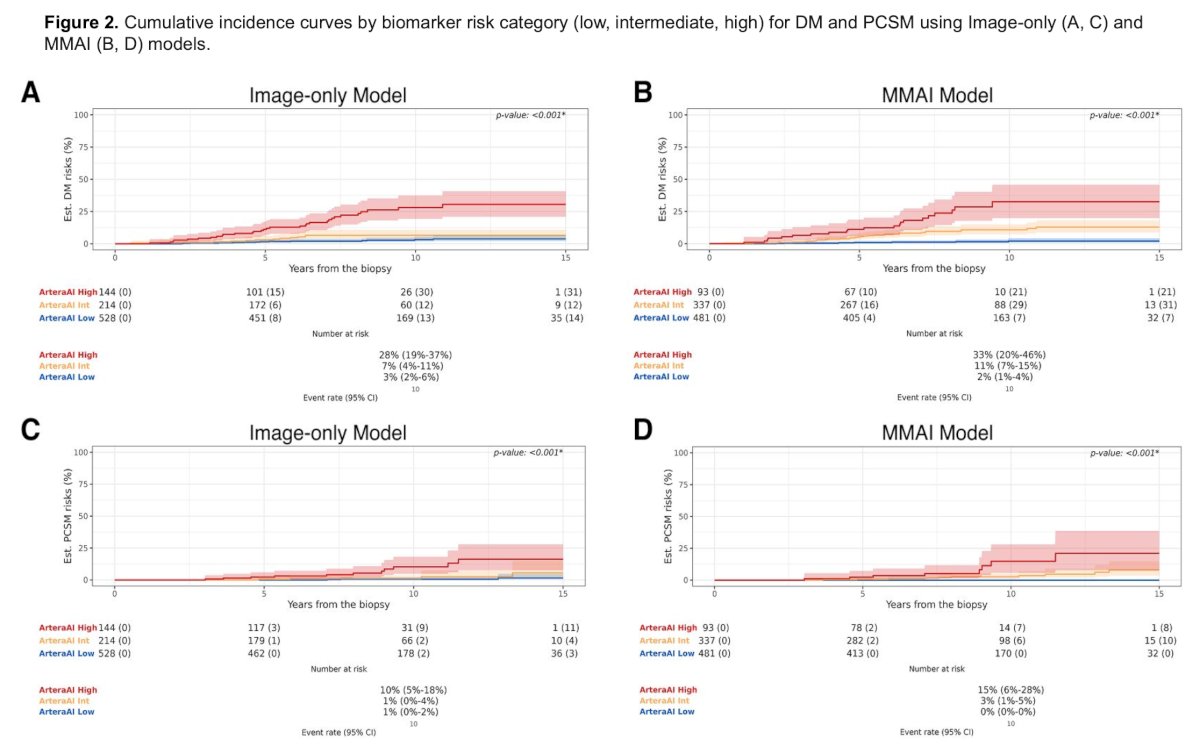
Both models were assessed for the prediction of the primary outcome of 10-year risk of distant metastasis and the secondary outcome of prostate cancer-specific mortality in a contemporary cohort of patients with localized prostate cancer treated at three US institutions:
- University of California, San Diego
- University of California, San Francisco
- University of Kansas Medical Center
The multimodal artificial intelligence (version 1.2) and image-only (version 1.3) models were previously trained and locked prior to this multicenter validation study:1
![The multimodal artificial intelligence (version 1.2) and image-only (version 1.3) models were previously trained and locked prior to this multicenter validation study [1]:](/images/com-doc-importer/241-suo-2025/suo-2025-huggins-medal-lecture-what-i-did-and-what-i-am-doing/image-7.jpg)
Retrospective clinical data and digital pathology from the first available routine prostate biopsies were compiled from each of the participating sites between February 2024 to September 2024. Eligible patients were diagnosed between 2005-2020 and had evaluable digital histopathology and complete clinical data. Due to different image pre-processing between the multimodal artificial intelligence and image-only models, multimodal artificial intelligence scores were generated for 991 patients and image-only scores for 886 patients. The multimodal artificial intelligence cohort was composed of 35% NCCN low-risk, 41% intermediate-risk, and 23% high-risk patients. Both multimodal artificial intelligence and image-only continuous and categorical scores were significantly associated with 10-year risk of distant metastasis and prostate cancer-specific mortality. Both models also remained significant when controlling for NCCN risk group or treatment. Finally, the models had similar categorical risk distribution:
Radical prostatectomy remains a preferred form of treatment for many patients, particularly those with higher-risk disease. Knowledge and technology have improved the procedure, and will continue to do so. However, surgery is overutilized and evaluation before surgery is often incomplete. Prostatectomy can be morbid, and residual disease in the pelvis is not uncommon based on biochemical recurrence rates, positive margins, and postoperative PSMA PET findings. In men with high-risk prostate cancer, 15–40% will have positive margins or missed metastatic disease in lymph nodes. Additionally, 30% of pelvic recurrences are often outside of the template.
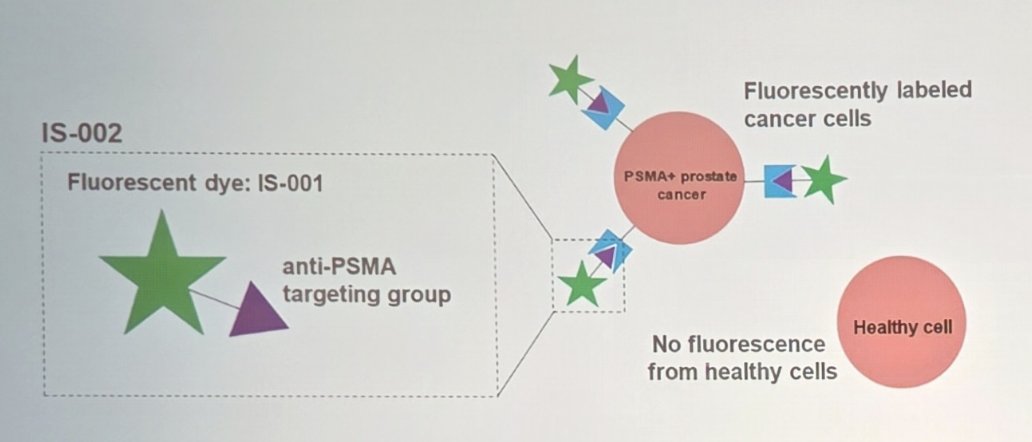
Dr. Carroll argues that for the surgical treatment of prostate cancer, better imaging may be (is?) critical. IS-002 consists of a PSMA-targeting group conjugated to a fluorescent dye detectable in the 785–804 nm near infrared spectrum. Because PSMA is overexpressed on prostate cancer cells and minimally expressed in surrounding healthy tissue, selective cancer imaging becomes feasible:
At UCSF, Dr. Carroll and colleagues undertook a phase I study using IS-002, with the primary objective of assessing safety and patient tolerance of IV-administered IS-002 on subjects undergoing robotic prostatectomy. The secondary objective was to evaluate the pharmacokinetics of IS-002, and an exploratory objective was to assess IS-002 efficacy in detecting prostate cancer. The population of patients for this study was high-risk men (CAPRA 6+). IS-002 enabled real-time visualization of residual prostate cancer not visible under standard white-light endoscopy, and biopsied fluorescent tissue confirmed adenocarcinoma:1


Dr. Carroll notes an upcoming phase 2 study evaluating the clinical impact on margin status and biochemical outcomes. The study will randomize 60 men with high-risk prostate cancer to the intervention arm of IS-002, given 24 hours +/- 6 hours prior to surgery, or the control arm of standard white-light endoscopy. The primary outcome is evaluation of surgical margins, and the secondary outcome is biochemical free survival. Potential biopsy locations include the apex, mid-gland, base, urethra, bladder neck, resection bed, or other (surgeon judgment):

- A non-proprietary SQL platform allowing fully integrated, multi-center data connectivity
- A structure built and guided by domain experts across urologic oncology, pathology, imaging, translational science, and data analytics
- Dedicated “cores” supporting:
- Pathology
- Radiology
- Clinical data
- Analytics
- Translational science
- Multi-omic biomarker integration
Dr. Carroll concluded his Huggins Medal Award lecture with the following take-home points emphasizing building infrastructure:
- Build infrastructure that informs clinicians and the patients they treat
- Measure and readjust, allowing teams to improve practice patterns and outcomes
- Enable testing of new technology now
- Value collaboration, emphasizing people and cross-disciplinary teamwork
- Leave something lasting
Presented by: Peter Carroll, MD, MPH, University of California, San Francisco (UCSF), San Francisco, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, Wed, Dec 3 – Fri, Dec 5, 2025.
Reference: