(UroToday.com) The 2025 Society of Urologic Oncology (SUO) Annual Meeting was host to a bladder cancer late-breaking abstract (LBA) session. Dr. Trinity Bivalacqua presented the first results from CORE-008 Cohort A, a phase II trial of intravesical Cretostimogene Grenadenorepvec in patients with high-risk (HR), BCG-naïve, non-muscle invasive bladder cancer (NMIBC).
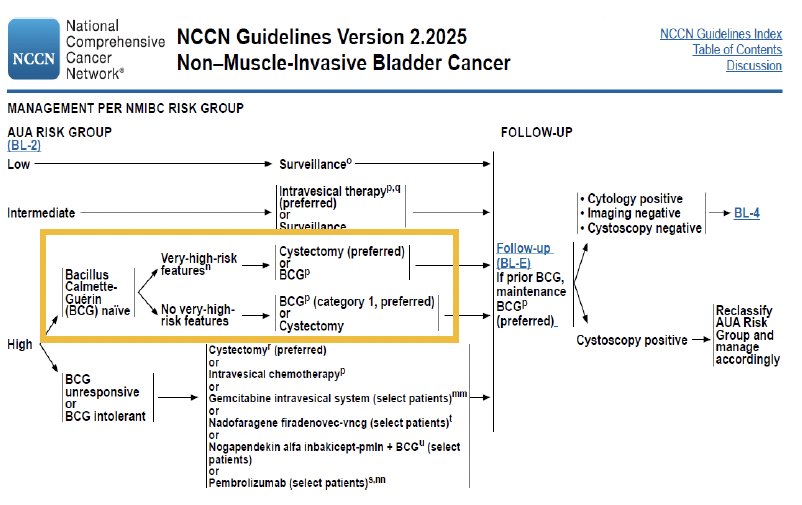
There is a considerable unmet need in HR NMIBC, with Dr. Bivalacqua noting that although guidelines recommend intravesical BCG or radical cystectomy, durability remains a challenge. Historical data show that over 50% of patients recur and 20–40% progress,1-3 although more contemporary series report improved durability with 3-year event-free survival (EFS) and disease-free survival (DFS) rates ≥75%.4 Up to 70% of patients experience BCG-related side effects leading to discontinuation,5-7 and ongoing BCG shortages further complicate disease management.8 Radical cystectomy carries substantial morbidity8,9 and quality-of-life impact.10
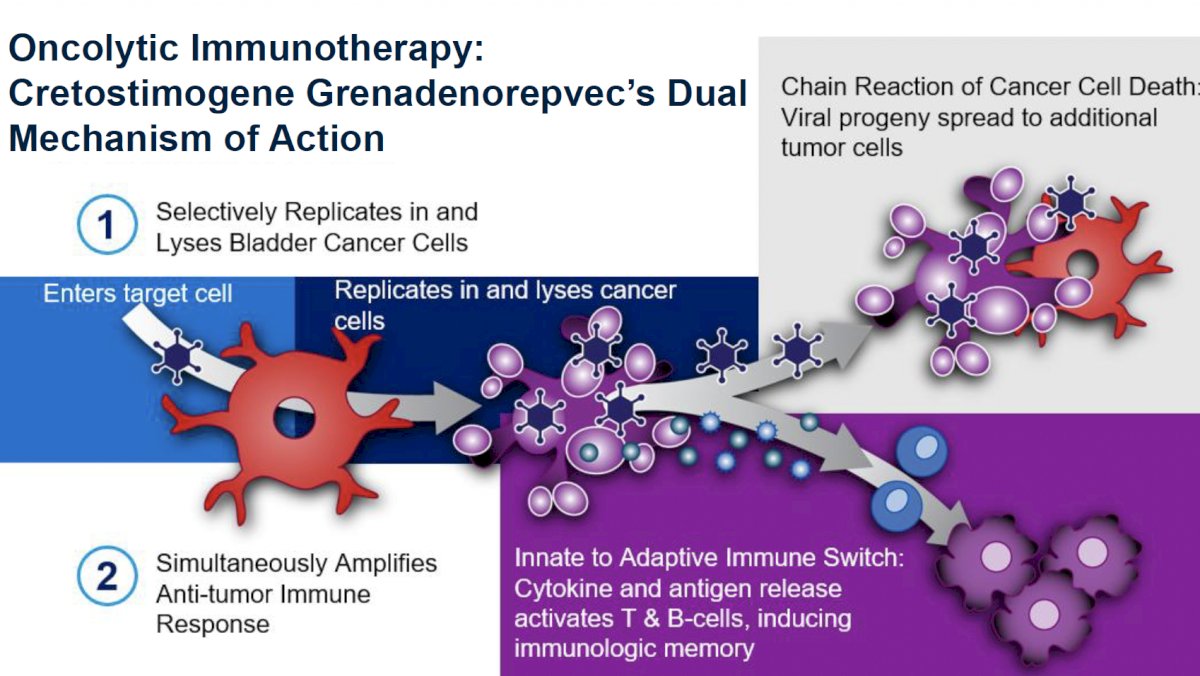
Cretostimogene is a conditionally replicating, highly immunogenic adenovirus driven by the E2F-1 promoter and encoding GM-CSF, enabling dual mechanisms of direct oncolysis and immune activation.
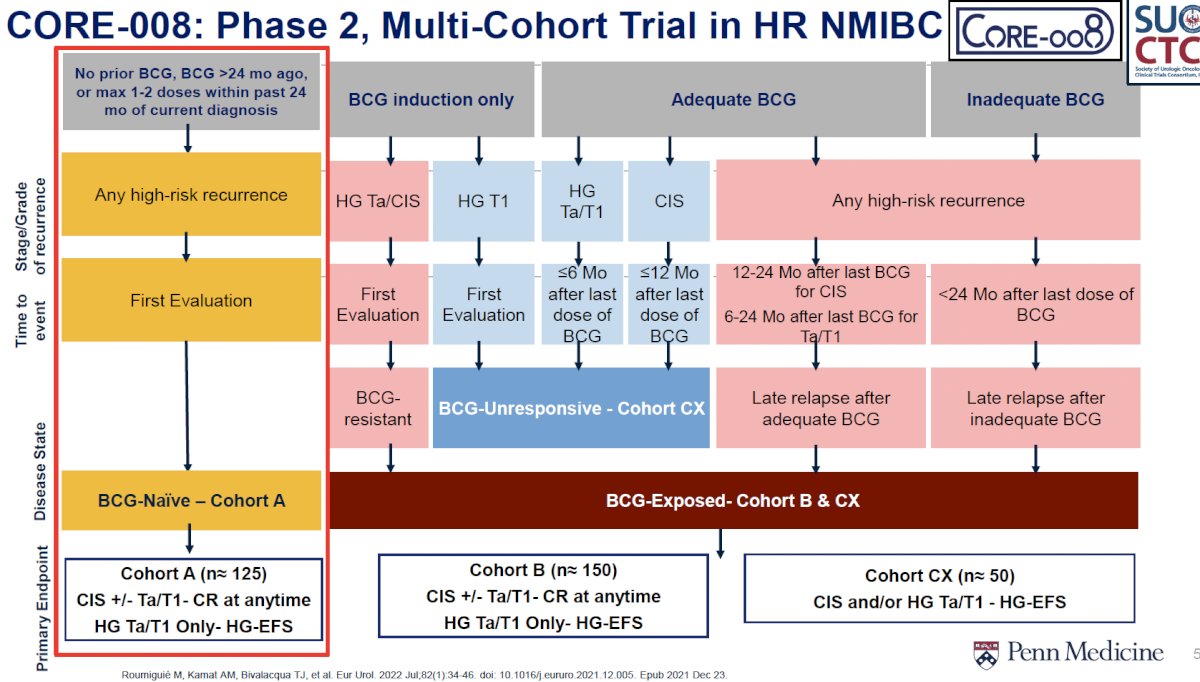
CORE-008 is a multi-cohort trial enrolling BCG-naïve (Cohort A), BCG-exposed (Cohort B), and BCG-unresponsive (Cohort CX) patients. Cohort A includes patients with CIS ± papillary disease or HG Ta/T1 disease, with primary endpoints of complete response in CIS and high-grade event-free survival (HG-EFS) for papillary patients.
The treatment schedule incorporates induction followed by maintenance, with re-induction permitted at Month 3 for persistent CIS or HG Ta. Patients were randomized 1:1 to either the original 5-step administration or an optimized 2-step administration. Cystoscopy and cytology were performed every 3 months with mandatory mapping biopsies at 12 months. A CT or MR urogram was performed every 6 months.

Baseline characteristics (n=54) showed a predominantly male (90.7%) and White (92.6%) cohort, with 88.8% older than 65 years. All patients were enrolled from the United States. HR NMIBC stage distribution included CIS alone (44.4%), CIS with HG Ta (31.5%), and CIS with HG T1 (24.1%). Most patients had no prior BCG exposure (87%), and 13% had received prior adjuvant intravesical chemotherapy.

With a median follow-up of 4.6 months, Cohort A demonstrated high initial efficacy. The overall complete response (CR) was 83.7% (95% CI 70.3–92.7), with 41 centrally confirmed CRs. Response rates were consistent across administration approaches: 79.2% (19/24; 95% CI 57.8–92.9) with the original method and 88% (22/25; 95% CI 68.8–97.5) with optimized administration. No patients required radical cystectomy, and no treatment-related progression to muscle-invasive or metastatic disease occurred. Three patients experienced NMIBC stage reclassification.

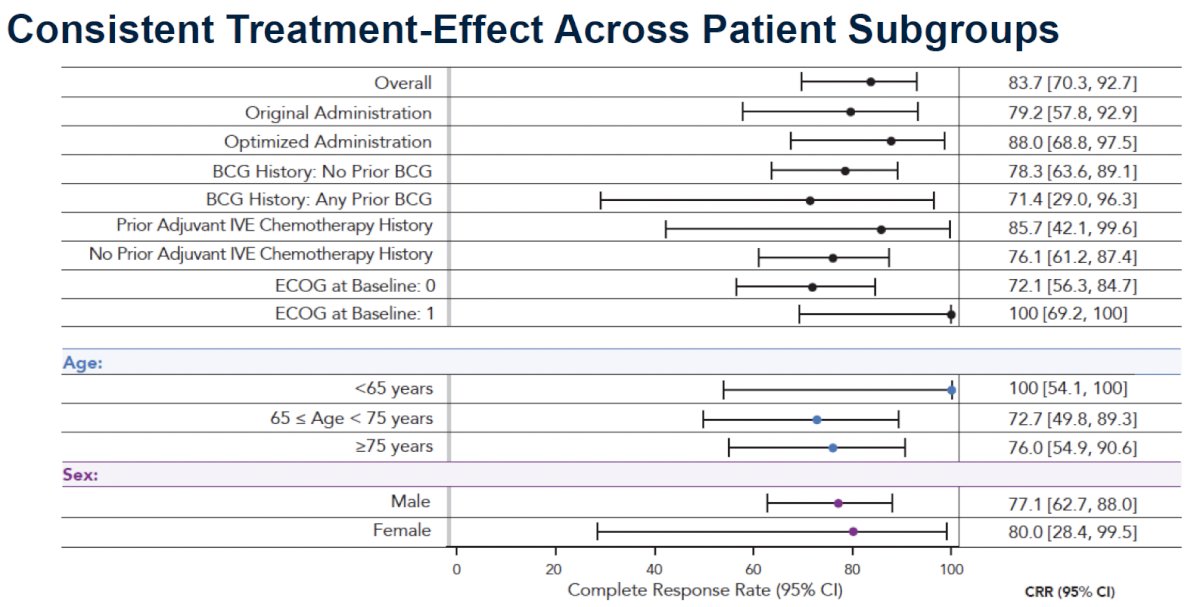
Subgroup analyses demonstrated consistent treatment effects across extensive clinical subsets, including ECOG performance status, age categories, sex, BCG history, and prior intravesical chemotherapy exposure. Complete response rates across subgroups ranged broadly but consistently overlapped with the overall CR estimate (95% CI 70.3–92.7).
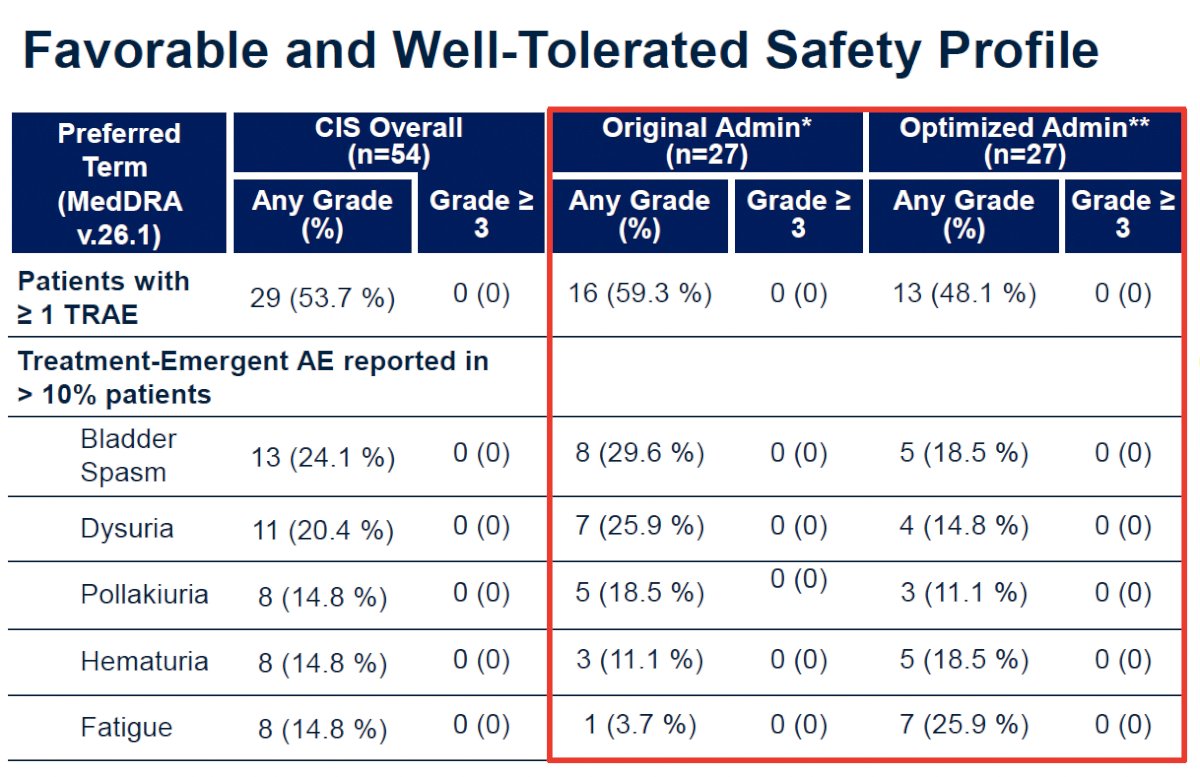
Safety findings were favorable. No Grade ≥3 treatment-related adverse events (TRAEs), serious adverse events, deaths, or treatment-related discontinuations were reported. A total of 98.1% (53/54) completed all protocol-defined treatments, including 96.3% in the original administration arm and 100% in the optimized arm. The most common TRAEs were bladder spasm (24.1%), dysuria (20.4%), pollakiuria (14.8%), hematuria (14.8%), and fatigue (14.8%), all Grade 1–2 in severity.
Dr. Bivalacqua concluded his presentation of the first results from CORE-008 Cohort A evaluating intravesical Cretostimogene Grenadenorepvec in patients with HR, BCG-naïve NMIBC as follows:
- Cretostimogene monotherapy demonstrates consistent efficacy, safety, and tolerability in HR BCG-Naïve NMIBC with CIS
- This regimen is aligned with current urology workflows: intravesical, bladder-sparing, no systemic toxicities
- Flexibility permitted with optimized administration
- These findings support continued development of cretostimogene across NMIBC disease states
- Additional treatment arms are planned for HR BCG-Naïve NMIBC
Presented by: Trinity Bivalacqua, MD, PhD, Professor, Department of Urology, University of Pennsylvania Perelman School of Medicine, Philadelphia, PA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) annual meeting held in Phoenix, AZ, between the 2nd and 5th of December 2025.
Related content: CORE-008 Cohort A First Results on Cretostimogene Grenadenorepvec for BCG-Naive Bladder Cancer - Shane Pearce
References:
- Sylvester RJ, van der Meijden APM, Lamm DL, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables. Eur Urol. 2006;49:466.
- Kamat AM, Li R, O’Donnell MA, et al. Predicting response to intravesical BCG therapy using clinical and tumor characteristics in high-risk non–muscle invasive bladder cancer. J Clin Oncol. 2016;34(16):1935-44. doi:10.1200/JCO.2015.64.4070.
- Roumiguie M, Colin P, Pignot G, et al. Updated management and outcomes in high-risk non–muscle invasive bladder cancer: A contemporary review. Eur Urol. 2022;82:34–46.
- Longoni M, Shkolyar E, Wright J, et al. Three-year recurrence and progression outcomes in high-risk NMIBC: Updated evidence from contemporary cohorts. Eur Urol Oncol. 2025;8:S2588-9311(25)00081-1.
- Brausi M, Oddens J, Sylvester R, et al. Side effects and treatment withdrawal in intravesical BCG therapy for NMIBC: Results from the EORTC Genito-Urinary Group. Eur Urol. 2014;65(1):69-76.
- Tapiero S, Sternberg IA, Ghandour R, et al. Adverse events and compliance patterns to BCG therapy in a contemporary cohort of NMIBC patients. Urology. 2018;118:107-113.
- Van der Meijden APM, Sylvester R, Oosterlinck W, et al. Maintenance BCG therapy for Ta T1 bladder cancer: Results from a randomized EORTC trial. Eur Urol. 2003;44(4):429-434.
- Holzbeierlein J, Cookson MS, Weiner AB, et al. National impact of the BCG shortage on NMIBC treatment patterns and outcomes. J Urol. 2024;10.1097/JU.0000000000003846.
- Maibom SL, Møller H, Vedsted P, et al. Early complications, readmissions, and mortality after radical cystectomy: A population-based study. BMJ Open. 2021;11(4):e043266.
- Clements M, Foster C, Witherspoon L, et al. Patient-reported outcomes and quality of life following radical cystectomy: A contemporary evaluation. Eur Urol. 2021;81(3):294-304.