(UroToday.com) The 2025 SUO annual meeting featured a prostate cancer session and a presentation by Dr. Rana McKay discussing emerging frontiers in metastatic prostate cancer. Dr. McKay started her presentation by making a plea for increasing genetic testing in metastatic prostate cancer, both somatic and germline testing, given that appropriate genetic testing will increasingly guide therapy moving forward. Somatic testing can be both prognostic and predictive (HRR, MSI). Germline testing can (i) be prognostic, (ii) be predictive, (iii) lead to cascade testing, and (iv) lead to secondary cancer screening.
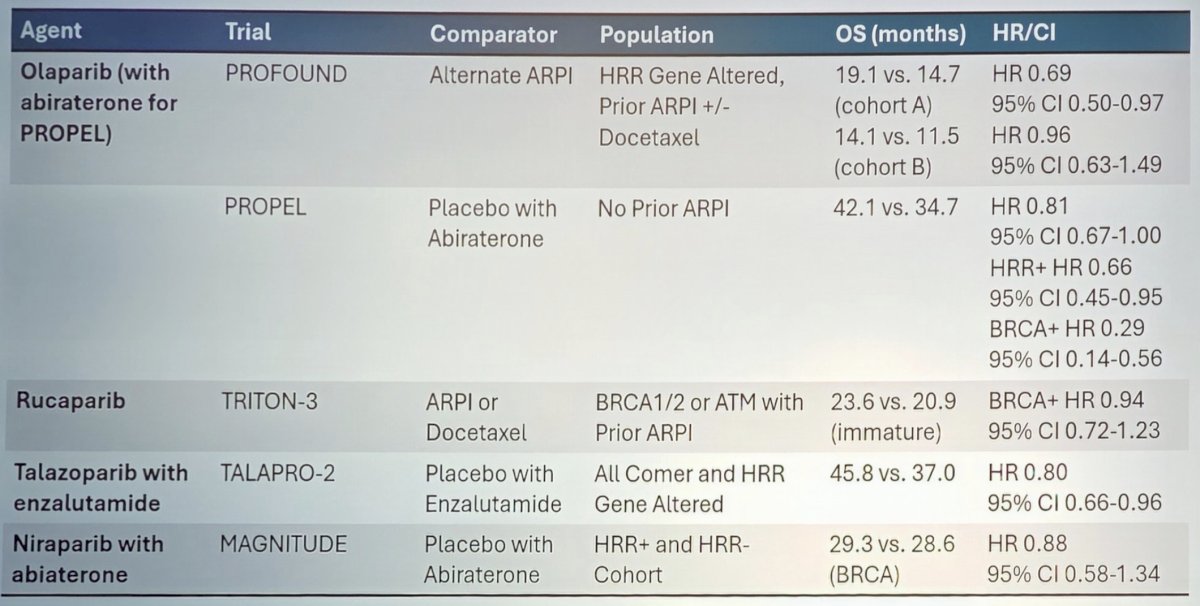
Dr. McKay then provided a high level overview of approved agents in metastatic prostate cancer. As follows is topline results table of approved PARP inhibitor agents:
177Lu-PSMA-617 is a beta emitting radioligand conjugated to PSMA binding peptide. PSMA is a cell surface receptor involved in folate uptake and cell migration, proliferation, and survival, which is overexpressed in ~80% of mCRPC. It is also expressed in normal prostate, proximal renal tubules, small intestines, and salivary glands.
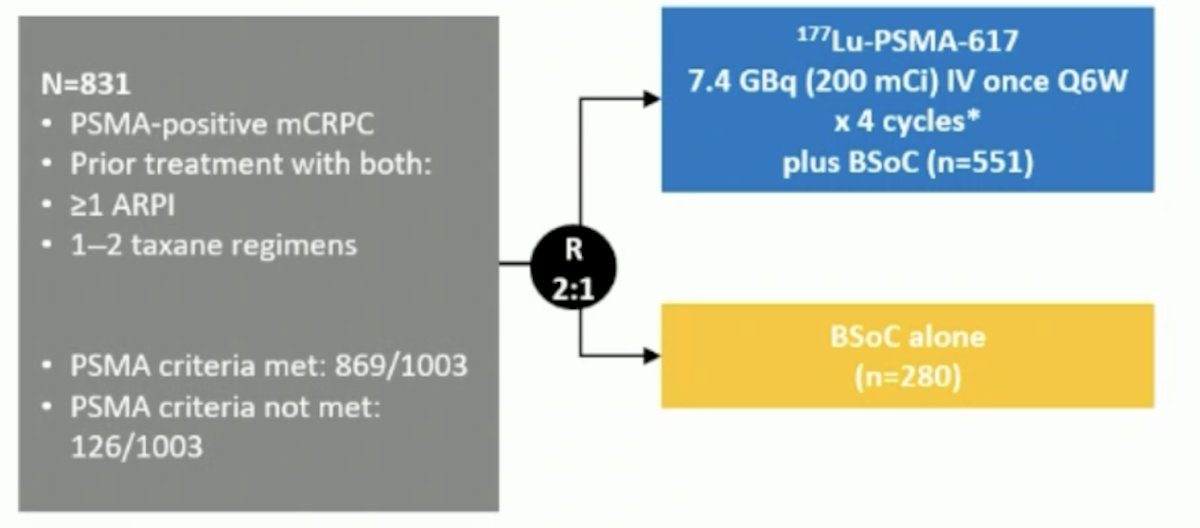
The phase 3 VISION trial evaluated 177Lu-PSMA-617 in men with PSMA-positive mCRPC who had previously received treatment with a next-generation androgen receptor signaling inhibition (abiraterone, enzalutamide, etc) and one or two prior lines of taxane chemotherapy:
There were two alternate primary endpoints: radiographic progression free survival and overall survival. Treatment with 177Lu-PSMA-617 + standard of care significantly improved radiographic progression free survival, treatment with 177Lu-PSMA-617 + standard of care significantly improved radiographic progression free survival by a median 5.3 months (median radiographic progression free survival, 8.7 versus 3.4 months; HR 0.40, 99.2% CI 0.29 to 0.57; p < 0.001). For overall survival, 177Lu-PSMA-617 improved overall survival by a median of 4.0 months (median overall survival: 15.3 versus 11.3 months; HR 0.62, 95% CI 0.52 to 0.74; p < 0.001), compared to standard of care alone:
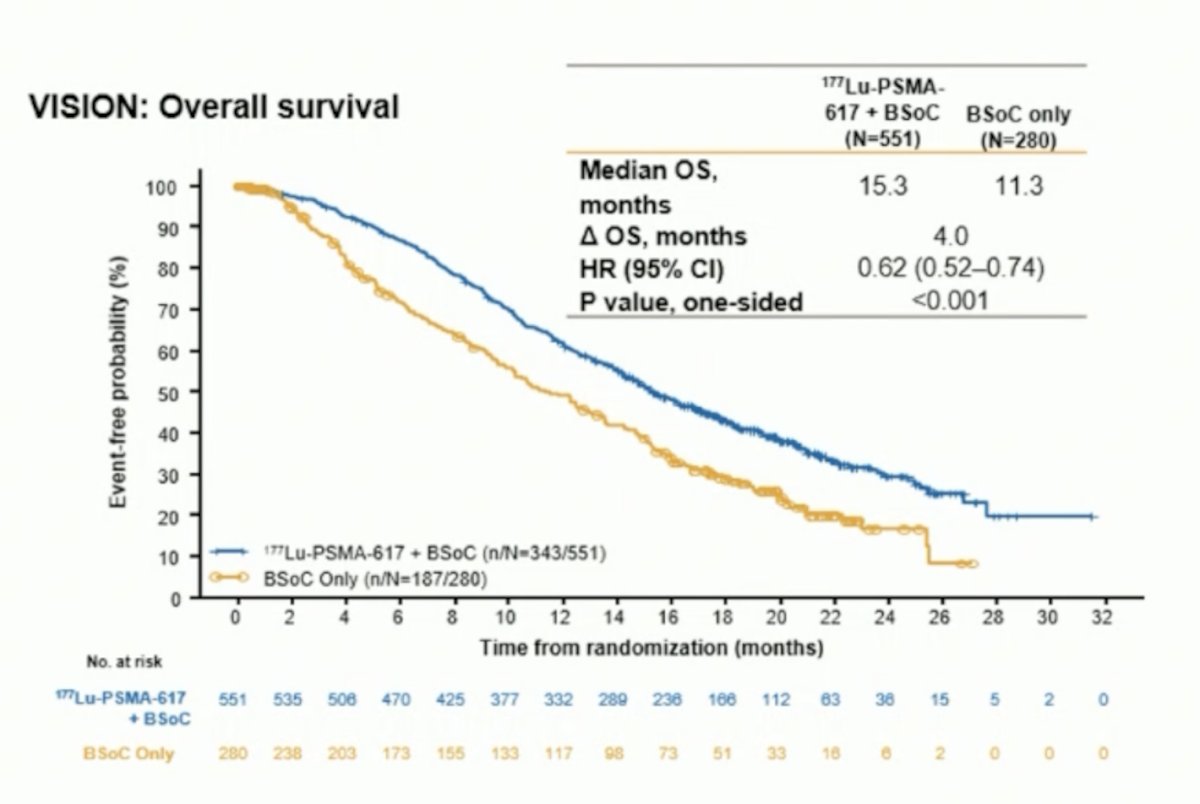
Dr. McKay notes that this trial was approved by the FDA in March 2022 for mCRPC patients post androgen receptor pathway inhibitor and chemotherapy.
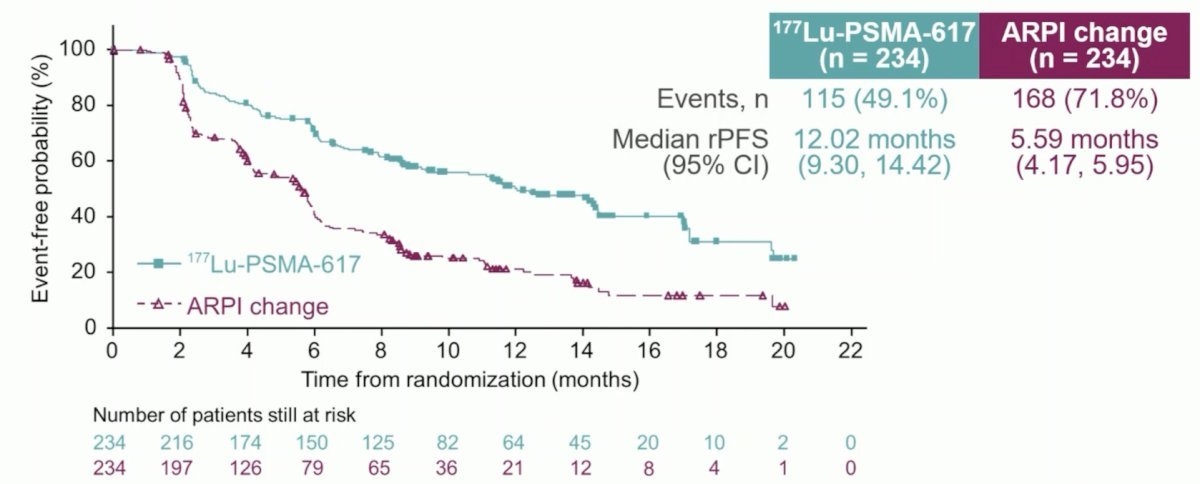
Eligible adults for PSMAfore had mCRPC, were candidates for an androgen receptor pathway inhibitor change after one progression on prior androgen receptor pathway inhibitor, and had ≥1 PSMA positive lesions and no exclusionary PSMA negative lesions by 68Ga-PSMA-11 PET/CT. Candidates for PARP inhibition and patients with prior systemic radiotherapy (<6 months ago), immunotherapy (except sipuleucel-T), or chemotherapy (except [neo]adjuvant >12 months ago) were ineligible. Randomization was 1:1 to open-label 177Lu-PSMA-617 (7.4 GBq every 6 weeks for 6 cycles) or androgen receptor pathway inhibitor change (abiraterone or enzalutamide). Importantly, patients randomized to androgen receptor pathway inhibitor could crossover to 177Lu-PSMA-617 following centrally reviewed radiographic progression.
At the primary analysis (median follow-up, 7.3 months; n = 467), the primary endpoint of radiographic progression free survival was met (HR 0.41, 95% CI 0.29 to 0.56), which was similar to second interim analysis (HR 0.43, 95% CI 0.33 to 0.54):
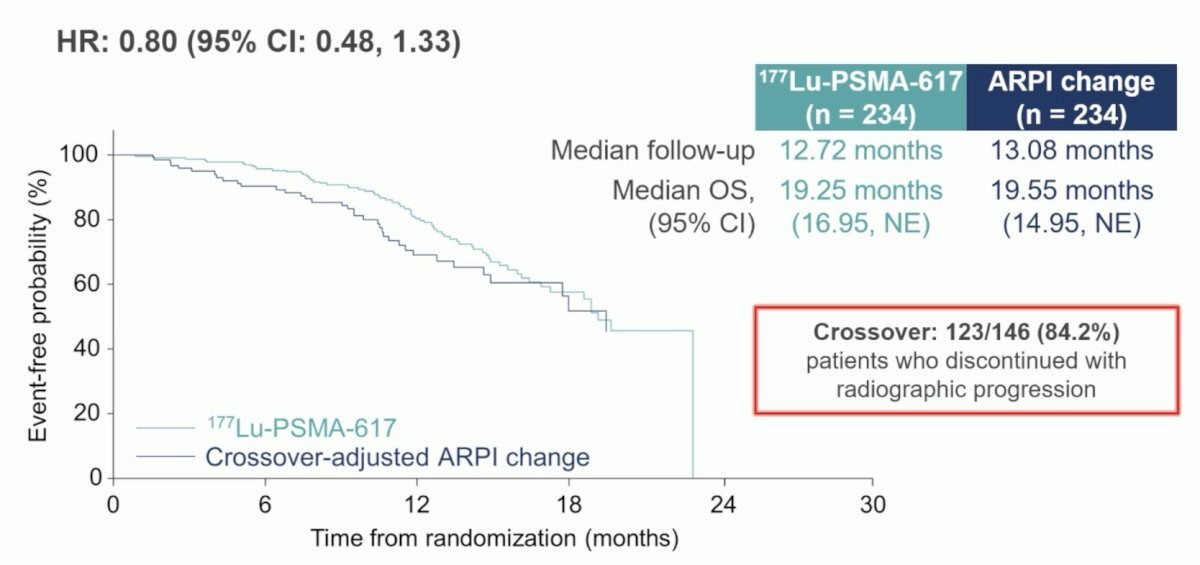
Additionally, at the second interim analysis (45.1% of target deaths), 123/146 (84.2%) patients with reviewed radiographic progression who discontinued androgen receptor pathway inhibitor crossed over to receive 177Lu-PSMA-617. In the pre-specified cross-over adjusted analysis, there was a trend favoring 177Lu-PSMA-617, but no statistical difference in overall survival between the groups:
Dr. McKay notes that in March 2025, the FDA approved 177Lu-PSMA-617 for post- androgen receptor pathway inhibitor patients considered appropriate for delayed taxane-based chemotherapy.
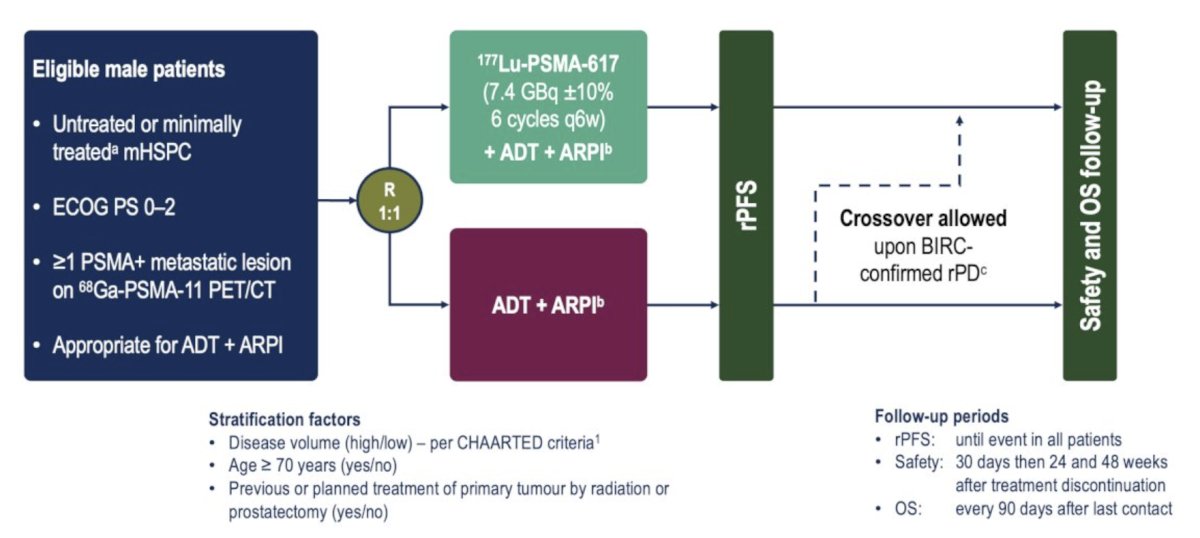
Next, Dr. McKay discussed treatments that are advancing for metastatic prostate cancer patients, but are not yet FDA approved. PSMAddition is a phase III trial of 177Lu-PSMA-617 combined with ADT + an androgen receptor pathway inhibitor in patients with PSMA-positive mHSPC, which was first presented at ESMO 2025. This trial randomized men with untreated or minimally treated mHSPC and ≥1 PSMA-positive metastatic lesion on 68Ga-PSMA-11 PET/CT to:
- Experimental arm: 177Lu-PSMA 617 (7.4 GBq ±10% 6 cycles q6w) + ADT + androgen receptor pathway inhibitor
- Control arm: ADT + androgen receptor pathway inhibitor
- Crossover to the 177Lu-PSMA 617 arm was permitted upon radiographic progression
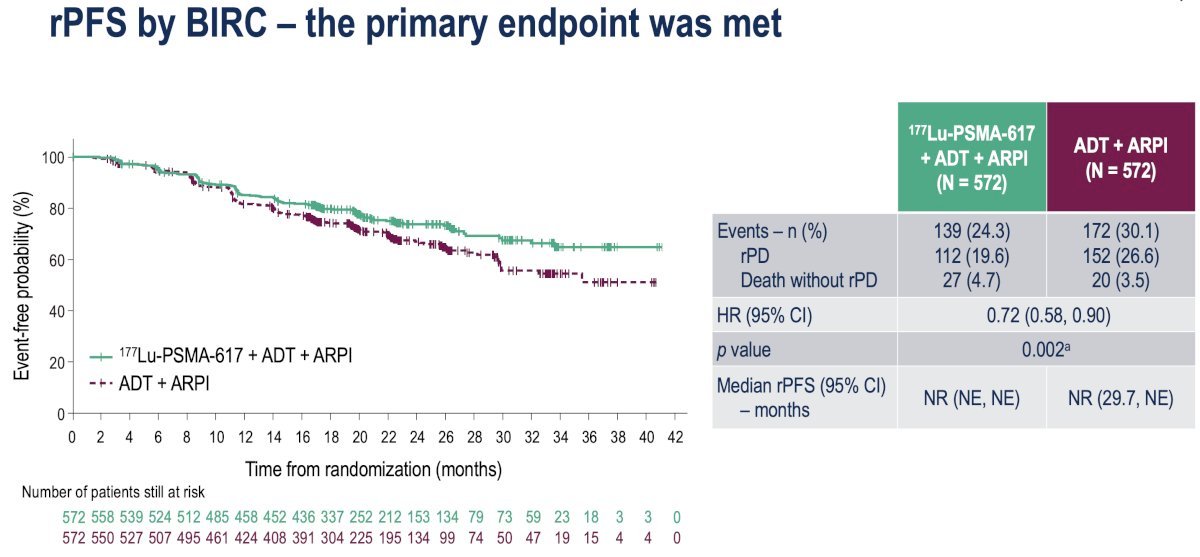
The study met its primary endpoint with radiographic progression free survival significantly prolonged with the addition of 177Lu-PSMA-617 (HR 0.72, 95% CI 0.58-0.90, p = 0.002). Median radiographic progression free survival has not been reached in either arm yet:
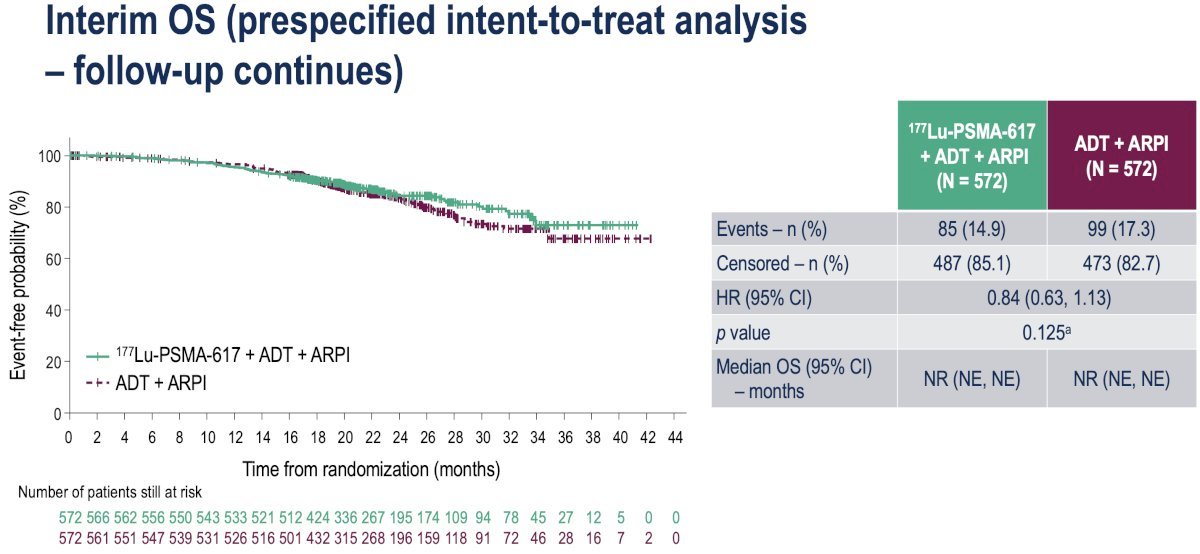
Overall survival analysis to date demonstrates a trend towards an overall survival benefit in the intervention arm (HR 0.84, 95% CI 0.64-1.13, p = 0.125):
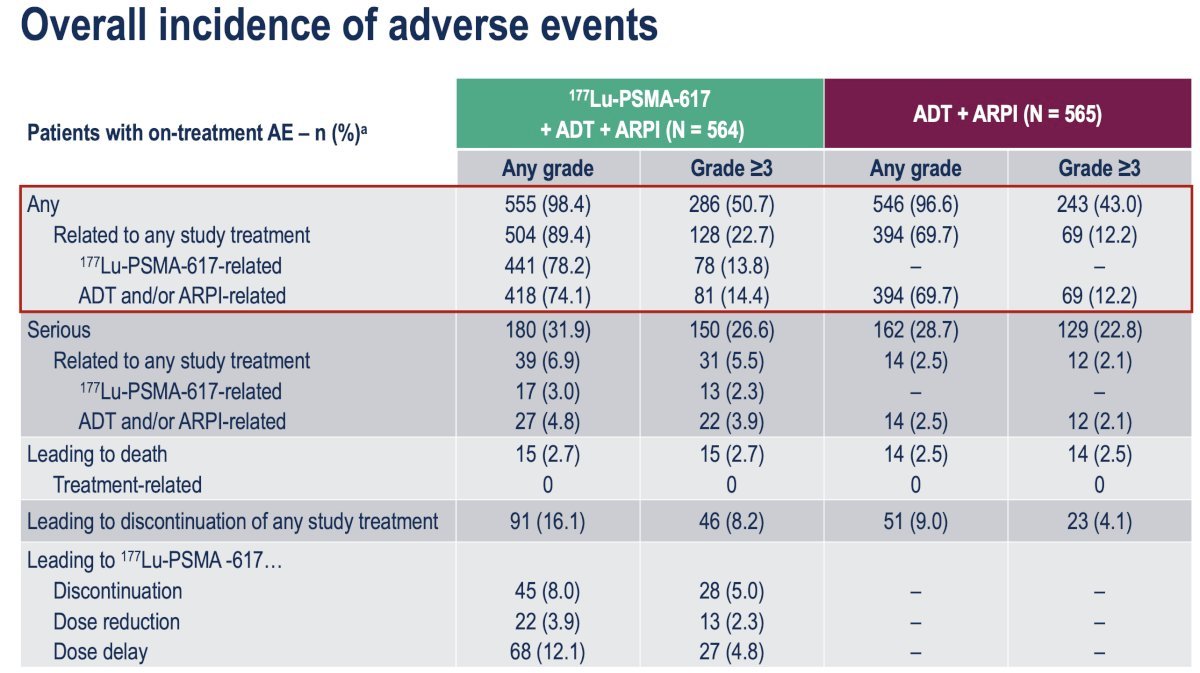
Any adverse event was observed in 98.4% and 96.6% of patients in the experimental and control arms, respectively. Grade ≥3 events were observed in 51% and 43%, respectively. Serious adverse events related to any study treatment were observed in 6.9% and 2.5% of patients, respectively (Grade ≥3: 5.5% versus 2.1%).
The AMPLITUDE trial was initially presented at ASCO 2025, a randomized, double-blind, placebo-controlled phase 3 study evaluating the efficacy of a fixed daily tablet of niraparib (200 mg) in combination with abiraterone acetate plus prednisone (1000 mg + 5 mg) and continuous ADT in patients with mHSPC harboring at least one HRR mutation in one of these genes: BRCA1, BRCA2, BRIP1, CDK12, CHEK2, FANCA, PALB2, RAD51B, RAD54L.
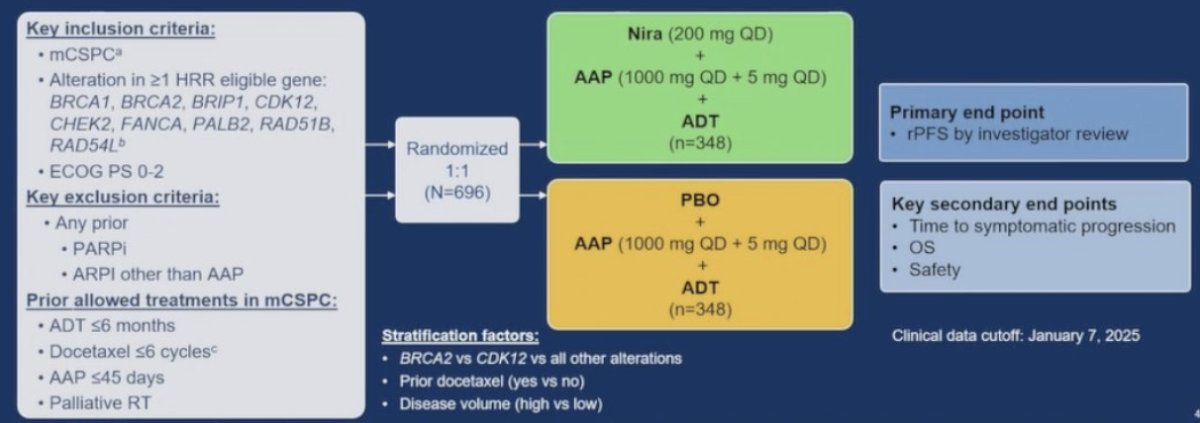
AMPLITUDE met its primary endpoint, demonstrating that the combination of niraparib and abiraterone acetate plus prednisone significantly reduced the risk of radiographic progression or death by 48% in the BRCA mutation group (HR 0.52, 95% CI 0.37–0.72; p < 0.0001) and by 37% in the broader HRR mutation population (HR 0.63, 95% CI 0.49–0.80; p = 0.0001).
The combination of niraparib and abiraterone acetate plus prednisone was associated with a 25% reduction in the risk of death in the BRCA mutations group (HR 0.75, 95% CI, 0.51–1.11; p = 0.15) and a 21% reduction in the HRR mutation group (HR 0.79, 95% CI, 0.59–1.04; p = 0.10). However, overall survival analysis remains immature, as fewer than 50% of the required events have occurred in either group.
Most participants remained on treatment, and the adverse event profile was generally manageable. Treatment emergent adverse events were reported in nearly all patients 99% in the niraparib + abiraterone acetate plus prednisone arm and 98% in the placebo + abiraterone acetate plus prednisone arm. Serious adverse events occurred in 39% of patients receiving the combination therapy compared to 28% in the control group. Treatment emergent adverse events leading to treatment discontinuation were observed in 15% of patients in the niraparib + abiraterone acetate plus prednisone group versus 10% in the placebo arm, showing a difference of less than 1%.
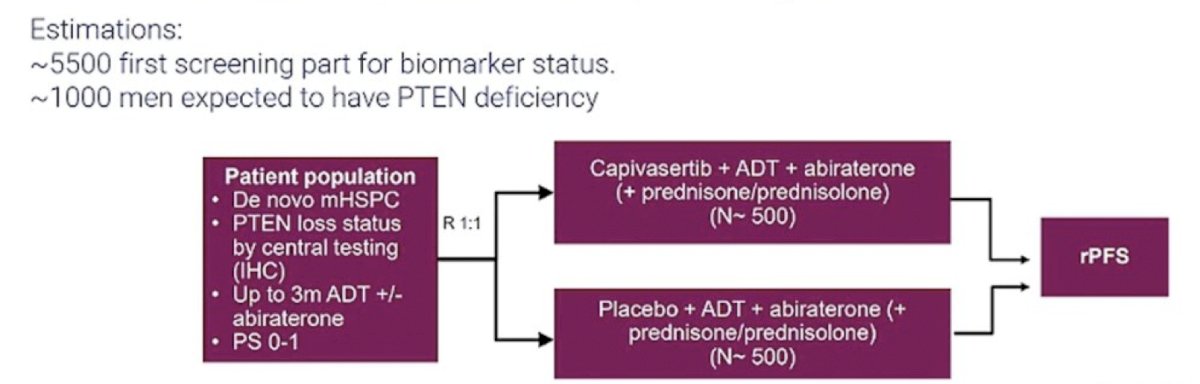
The next trial discussed by Dr. McKay was the CAPItello-281 trial, presented at ESMO 2025. CAPItello-281 is a global, multicenter, randomized, double-blind, phase III trial that included patients meeting the following eligibility criteria: (i) de novo mHSPC and (ii) PTEN deficiency (≤10% of cells expressing PTEN by IHC). Eligible participants (n = 1,012) were randomized 1:1 to capivasertib (400 mg BID, 4 days on and 3 days off) + abiraterone acetate (1,000 mg daily) + prednisone (5 mg daily) + ADT versus placebo + abiraterone acetate + prednisone + ADT. The primary endpoint was investigator-assessed radiographic progression free survival:
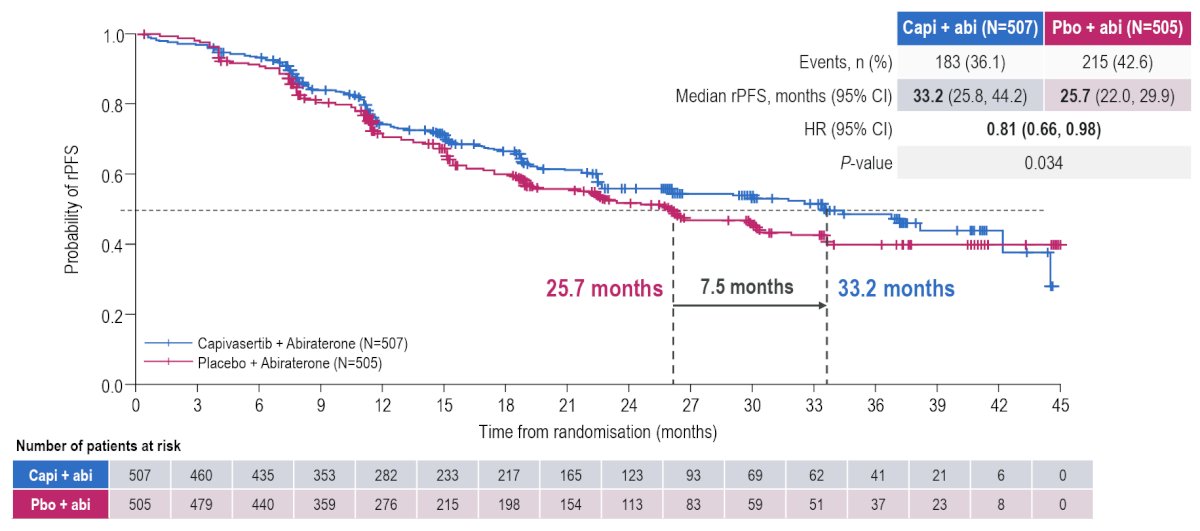
The study met its primary endpoint with capivasertib prolonging radiographic progression free survival by 7.5 months (median: 33.2 versus 25.7 months; HR 0.81, 95% CI 0.66-0.98, p = 0.034):
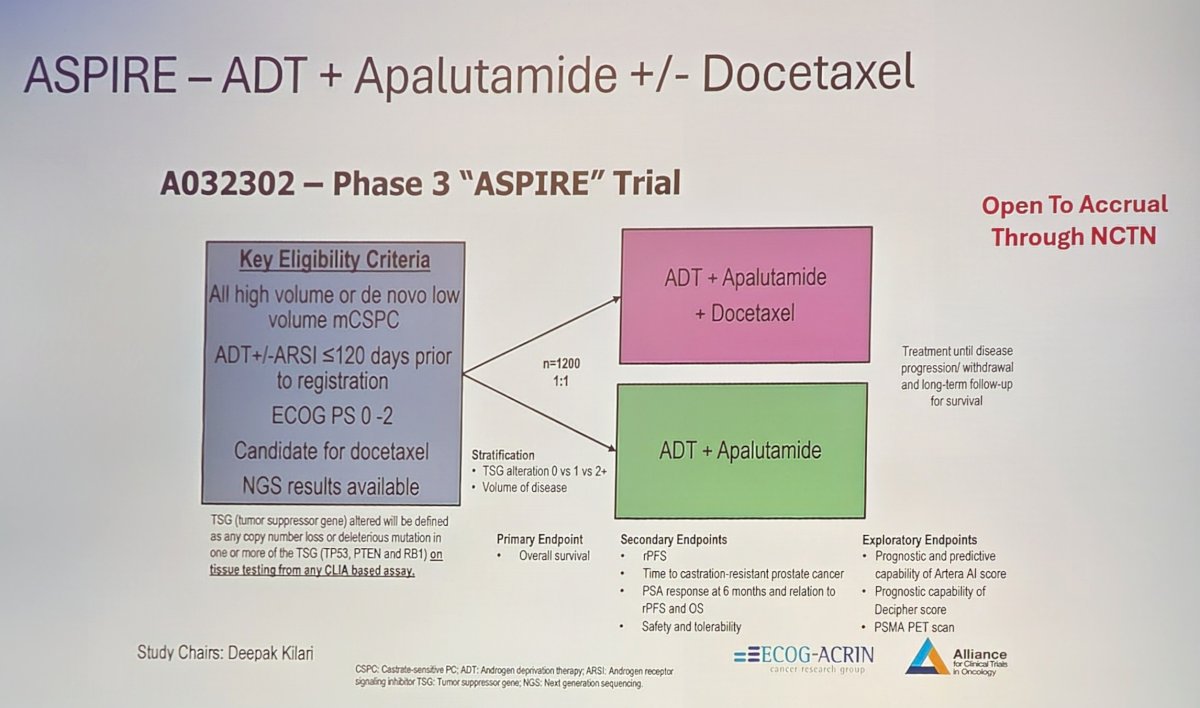
Dr. McKay also discussed three trials in progress she is excited about, first noting the ASPIRE trial, which is testing ADT + apalutamide +/- docetaxel in all high volume and low volume de novo mHSPC. The primary endpoint for this trial is radiographic progression free survival:
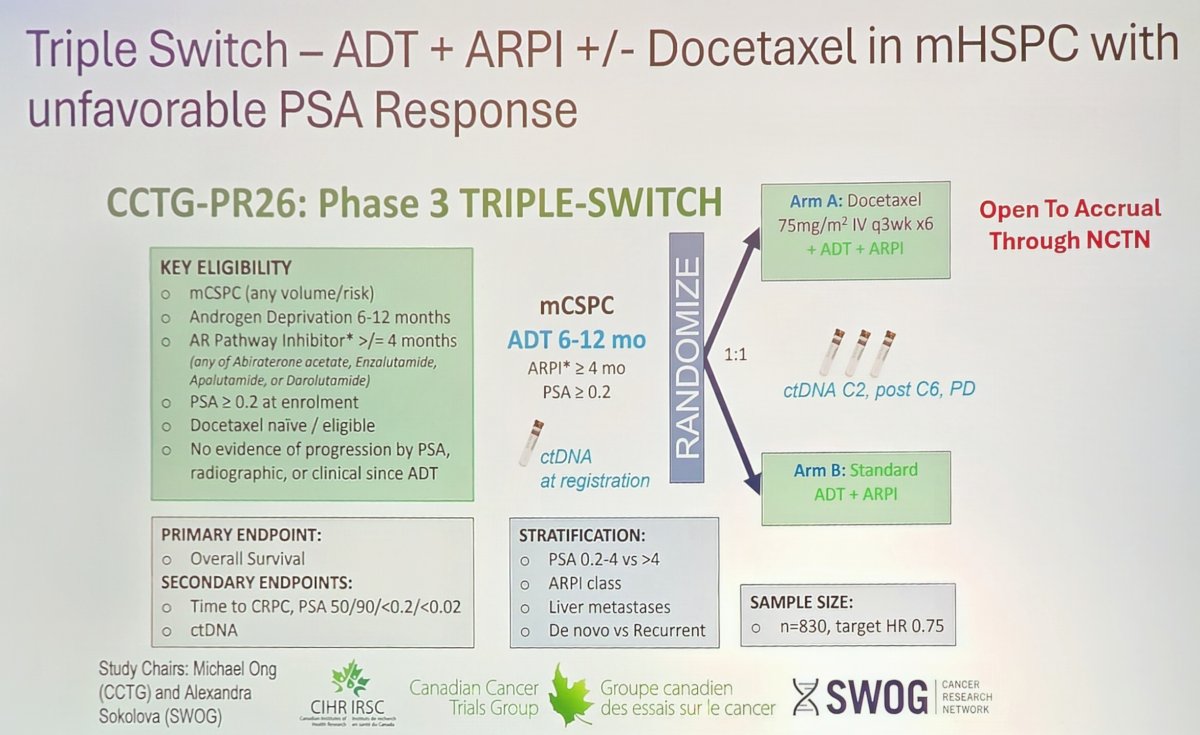
The second trial is the Triple Switch trial, which assesses ADT + androgen receptor pathway inhibitor +/- docetaxel in mHSPC with an unfavorable PSA response on doublet therapy. The primary endpoint for this trial is overall survival:
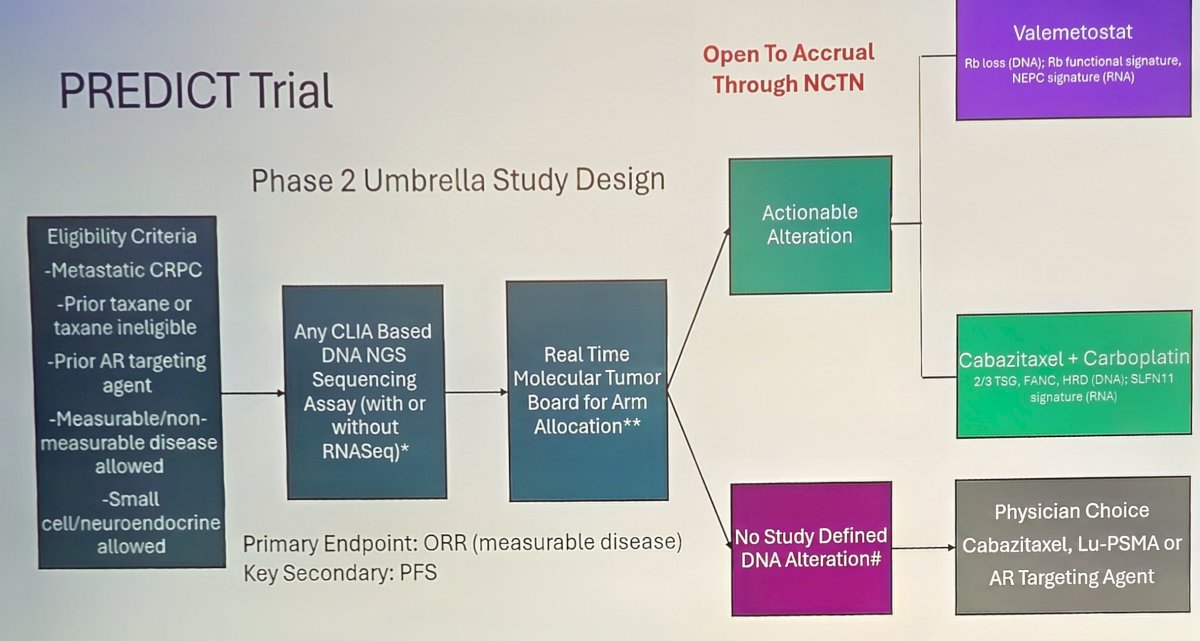
Third, the PREDICT trial, which is a phase 2 umbrella study in mCRPC:
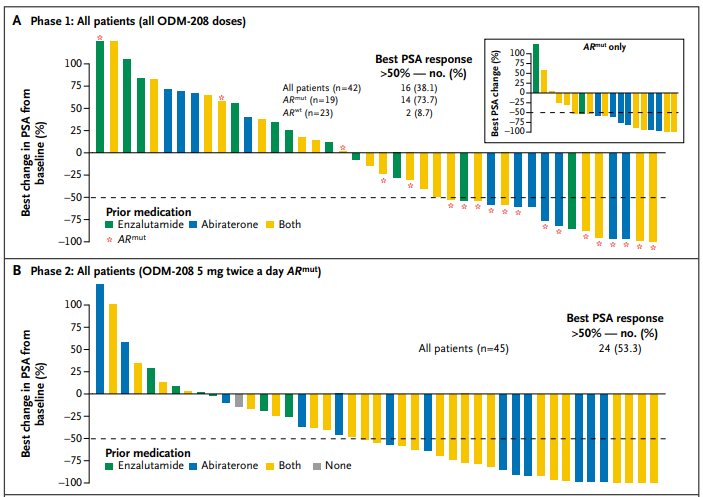
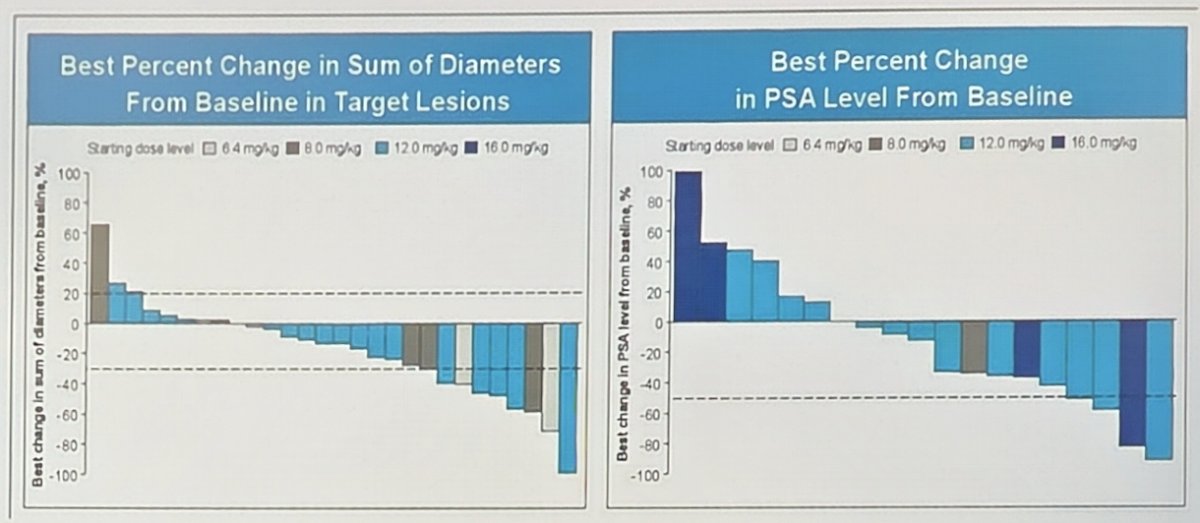
To conclude her presentation, Dr. McKay discussed several therapeutic agents that we are looking ahead to. Opevesostat (ODM-208) inhibits the first step of steroidogenesis, targeting CYP11A1. CYPIDES was the first-in-human phase 1 (3 + 3 design) and phase 2 study,3 administering ODM-208 twice daily with glucocorticoid/mineralocorticoid replacement and ongoing ADT to adults with previously treated mCRPC, regardless of androgen receptor gene ligand-binding domain mutations (phase 1) and with activating androgen receptor ligand-binding domain mutations (phase 2). Overall, there were 92 patients who received one or more doses of ODM-208: 47 in phase 1 (42.6% with an activating androgen receptor ligand-binding domain mutation) and 45 in phase 2. Treatment related adrenal insufficiency was the most common toxicity in phase 1 (n = 17, 36.2%; necessitating ODM-208 discontinuation in one patient). Adrenal insufficiency occurred in six patients (13.3%) at 5 mg twice a day in phase 2. A PSA50 response occurred in 14 of 19 (73.7%) patients with an activating androgen receptor ligand-binding domain mutation, and 2 of 23 (8.7%) patients with androgen receptor wild type in phase 1, and in 24 of 45 (53.3%) patients with an activating androgen receptor ligand-binding domain mutation in phase 2:
ARV-766/JSB462 (luxdegalutamide) is an androgen receptor degrader, with initial results presented by Dr. Petrylak at ASCO 2024. This agent is a novel, potent, orally administered PROTAC androgen receptor degrader that targets wild-type androgen receptor and clinically relevant androgen receptor ligand-binding domain mutants, including the most prevalent androgen receptor L702H, H875Y, and T878A mutations:
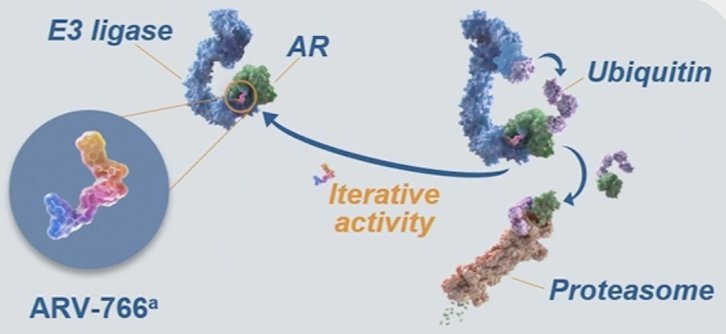
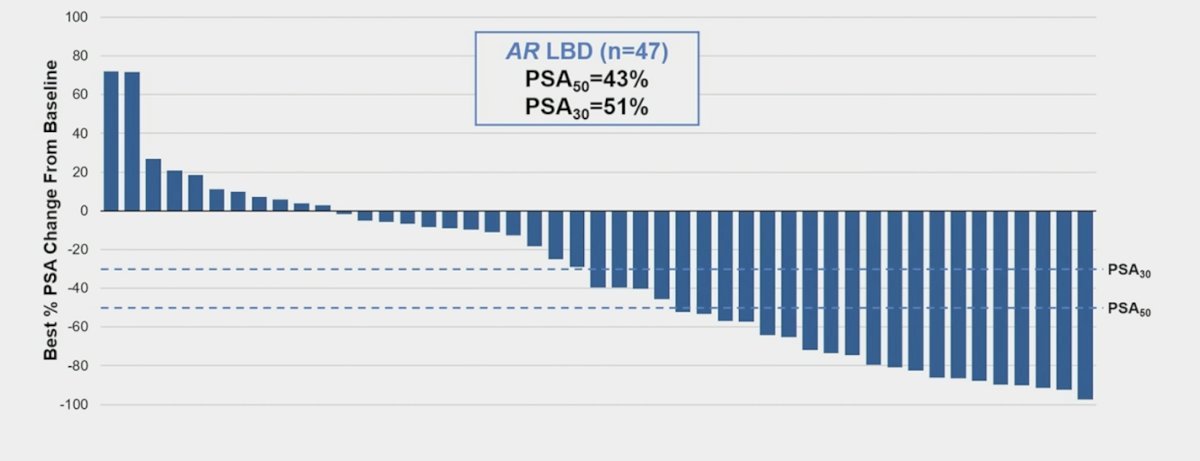
In the initial phase I/II study, eligible patients had progressive mCRPC and ongoing ADT. The phase 1 dose escalation portion evaluated the safety and tolerability of escalating doses of ARV-766 (20–500 mg once daily) in patients who had progressed on ≥2 prior systemic therapies (including ≥1 novel hormonal agents). The phase 2 cohort expansion portion is evaluating the clinical activity and safety of 2 doses of ARV-766 (100 or 300 mg once daily) in patients who had received 1–3 prior novel hormonal agents and ≤2 prior chemotherapy regimens. This study found that among patients with androgen receptor ligand-binding domain mutations, PSA50 was 43% and PSA30 was 51%:
Infinatamab deruxtecan (DS-7300/MK-2400) is a B7H3 directed antibody drug conjugate with a topoisomerase I inhibitor payload. Among 29 patients, 19 (65.5%) of patients with RECIST-evaluable lesions experienced tumor shrinkage. Additionally, there was a 31.0% confirmed or unconfirmed partial response rate, and the disease control rate was 72.4%. Moreover, 63.2% of patients with PSA data experienced a decrease in PSA, and 21.1% had a PSA50 response.
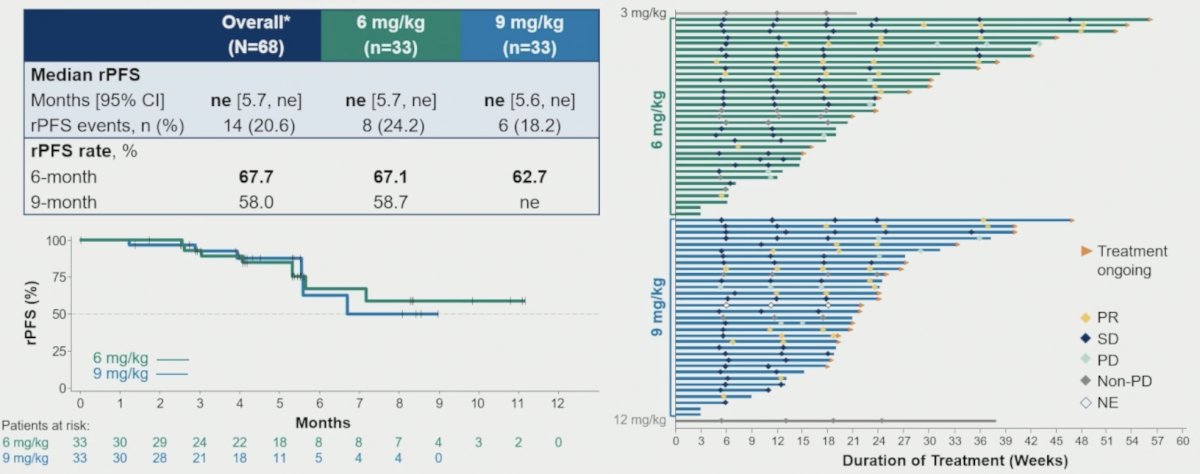
DB-1311/BNT324 is an investigational B7H3 antibody drug conjugates that received FDA Fast-Track Designation for previously treated CRPC:

Among 52 response-evaluable patients (measurable disease at baseline per RECIST 1.1), the best overall response was partial response in 22 patients and stable disease in 25 patients for an unconfirmed objective response rate of 42.3% (95% CI 28.7-56.8) and disease control rate of 90.4% (95% CI 79.0, 96.8). The median duration of response was not reached (95% CI 4.0, NE):
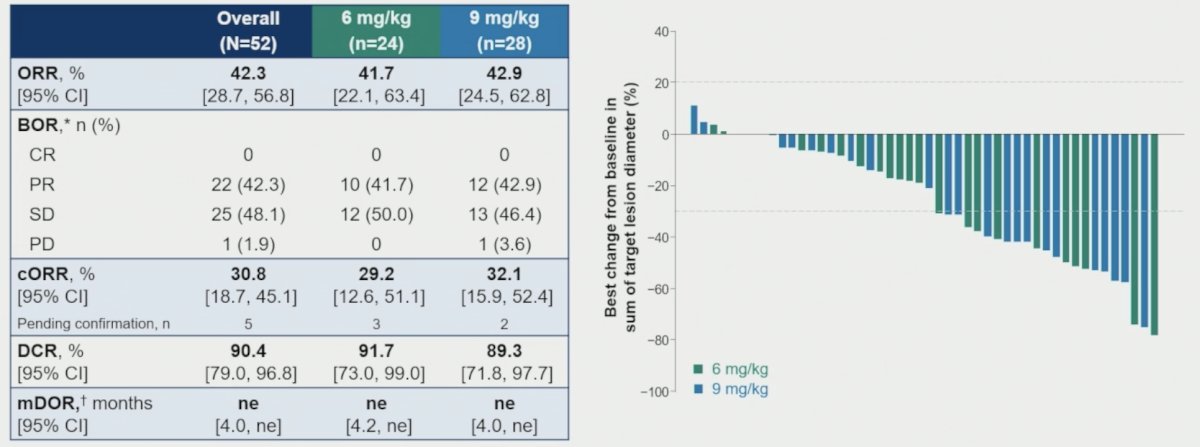
The median radiographic progression free survival (n = 68) was not reached (95% CI 5.7, not reached) with a 6-month rate of 67.7%:
In a phase I study, the STEAP-1 targeting bi-specific T cell engager, Xaluritamig (AMG 509), was evaluated in heavily pre-treated mCRPC patients who had progressed on a prior androgen receptor pathway inhibitor and a taxane.4 Notably, there were 53% of patients that had visceral metastases, including 37% with liver metastases. A PSA50 response was observed in 49% of patients, and a PSA90 response was observed in 30%.
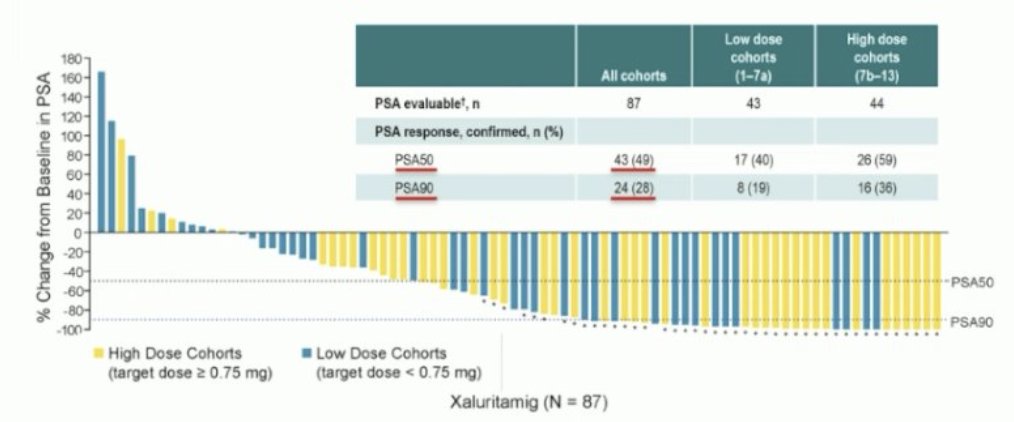
From a safety standpoint, cytokine release syndrome was present in ~70% of patients. However, only 3% of patients discontinued this drug because of cytokine release syndrome.
Pasritamig is a first-in-class T-cell-redirecting bispecific antibody targeting human kallikrein 2. Pasritamig simultaneously binds KLK2 on prostate cancer cells and CD3 receptor complexes on T cells, leading to T-cell activation and subsequent lysis of cancer cells.
Pasritamig target doses were escalated from 0.5-2000 mg SC and 150-900 mg IV QW-Q6W, with various step-up dosing schedules. Pre-medication with dexamethasone (16 mg) was required in step-up and first target dose. The primary objective was to determine the safety and the recommended phase 2 dose, whereas secondary objectives included preliminary assessment of antitumor activity.
There were no pasritamig-related deaths. One patient experienced a dose limiting toxicity of transient grade 3 ALT/AST elevation after 50 mg step-up 2 SC administration. While most patients reported ≥1 treatment related adverse events (82.8% overall), these were mostly low grade, with only 9.8% of patients experiencing a grade ≥3 treatment related adverse event.
In the recommended phase 2 dose efficacy population (n = 33; 3.5 mg [Day 1], 18 mg [Day 8], 300 mg Q6W IV), PSA50 was 42.4% (14/33).
The objective response rate in the 84 patients with measurable disease was 8.3% and the median duration of response of 8.9 (95% CI 3.6, NE) months. In the recommended phase 2 dose efficacy population, the median radiographic progression free survival was 7.9 (95% CI 2.9, NE) months, with 21.2% of patients with treatment ongoing. PSA50 responses and durable disease control were observed irrespective of prior treatment with taxanes or PSMA targeted radioligand therapy.
Dr. McKay concluded her presentation discussing emerging frontiers in metastatic prostate cancer with the following take home points:
- There have been significant advances in advanced prostate cancer treatment
- Somatic tumor and germline sequencing is recommended for all patients with advanced disease
- The newest FDA approvals include PARP inhibitor + androgen receptor pathway inhibitor combinations for HRR altered mCRPC and 177Lu-PSMA-617 in the pre-chemotherapy setting
- There are many novel agents in testing, including androgen receptor targeting, antibody drug conjugates, T-cell engagers, and others
Presented by: Rana McKay, MD, UC San Diego, San Diego, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, Wed, Dec 3 – Fri, Dec 5, 2025.
References:
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103.
- Morris MJ, Castellano D, Herrmann K, et al. 177Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naïve patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): A phase 3, randomized, controlled trial. Lancet 2024 Sep 28;404(10459):1227-1239.
- Fizazi K, Bernard-Tessier A, Roubaud G, et al. Targeted inhibition of CYP11A1 in castration-resistant prostate cancer. NEJM Evid. 2024 Jan;3(1):EVIDoa2300171.
- Kelly WK, Danila DC, Lin CC, et al. Xaluritamig, a STEAP1 x CD3 XamAb 2+1 Immune Therapy for Metastatic Castration-Resistant Prostate Cancer: Results from a Dose Exploration in a First-in-Human Study. Cancer Discov. 2024 Jan 12;14(1):76-89.
- Stein MN, Vinceneux A, Robbrecht D, et al. Pasritamig, a First-in-Class, Bispecific T-Cell Engager Targeting Human Kallikrein 2, in Metastatic Castration-Resistant Prostate Cancer: A Phase I Study. J Clin Oncol. 2025 Aug;43(22):2515-2526.