(UroToday.com) At the 2025 SUO Annual Meeting, Dr. Hristos Kaimakliotis presented the primary efficacy and surgical outcomes from KEYNOTE-905/EV-303, a phase III study evaluating perioperative enfortumab vedotin plus pembrolizumab (EV + pembro) versus radical cystectomy (RC) alone in cisplatin-ineligible patients with cT2–T4aN0M0 or T1–T4aN1M0 muscle-invasive bladder cancer.
Eligible participants were cisplatin-ineligible by Galsky criteria or had contraindications to cisplatin. Variant histology was permitted, but ≥50% urothelial histology was required. Patients were randomized to EV + pembro before and after RC or to immediate RC alone. The primary study endpoint was event-free survival (EFS) by blinded independent central review (BICR). Key secondary endpoints were overall survival (OS) and pathological complete response (pCR). Of note, treatment was halted in November 2022 due to positive futility boundaries being exceeded in favor of the investigational arm.
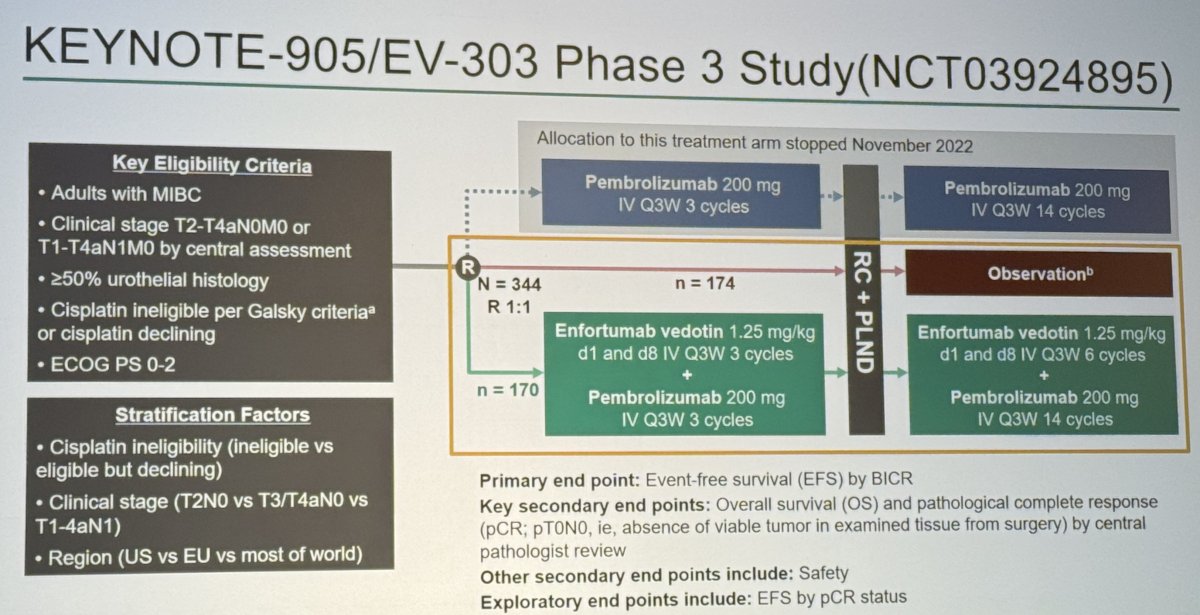
A total of 344 participants were randomized (EV + pembro: 170; Control: 174) between December 2020 and June 2024. In the EV + pembro arm, 167 began neoadjuvant therapy and 148 underwent surgery. The control arm included 156 participants who underwent RC. Common reasons for not undergoing surgery included patient withdrawal, physician decision, and progression in the neoadjuvant phase. The median time from randomization to RC was 14.1 weeks in the EV + pembro group and 6.4 weeks in the control group. The median time from completion of EV + pembro to RC was 5.6 weeks only.
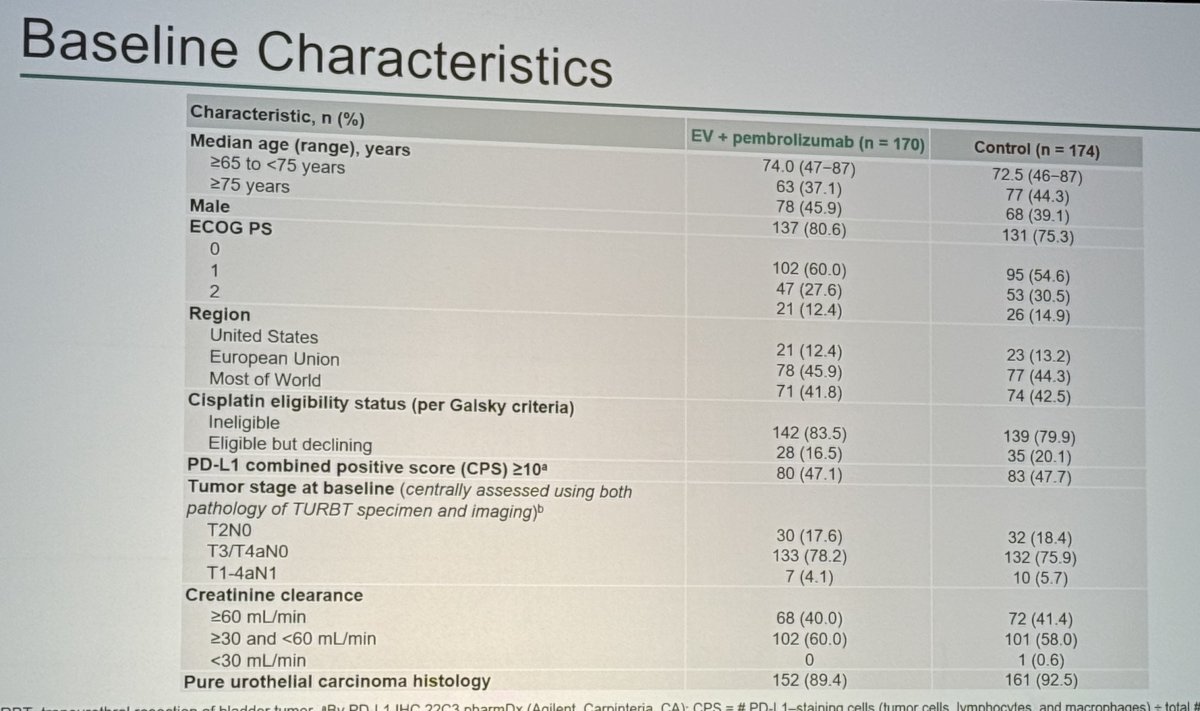
The baseline characteristics were well balanced. The median age was 74 years in the EV + pembro arm and 73 years in the control arm, with approximately 74% male in each group. Around two-thirds of participants were from the United States. Cisplatin ineligibility due to renal impairment was present in roughly half of the patients in each arm. PD-L1 combined positive score ≥10 was observed in 50.6% of EV + pembro and 51.1% of control participants.
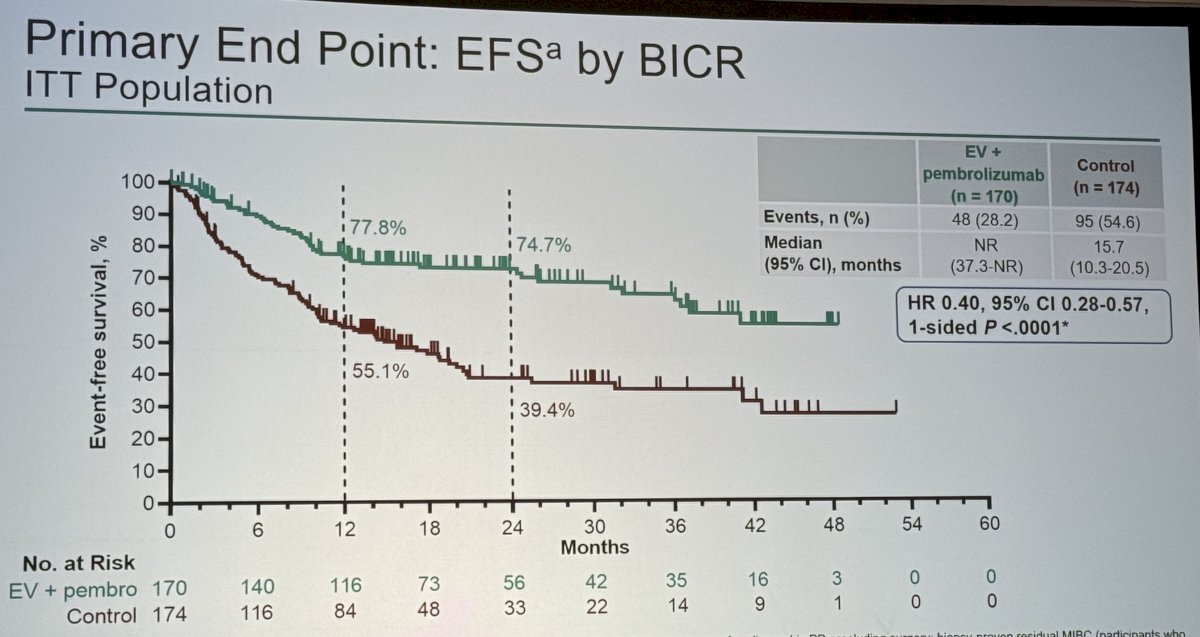
The primary endpoint, EFS by BICR, demonstrated a clear benefit in favor of perioperative EV + pembro. At 12 months, EFS was 77.8% with EV + pembro versus 55.1% in the control arm. At 24 months, EFS was 74.7% versus 39.4%, respectively. Median EFS was not reached for EV + pembro (95% CI 42.8–NE) and 17 months (95% CI 13–27) for control. EV + pembro reduced the risk of EFS events by 60% (HR 0.40, 95% CI 0.28–0.57; 1-sided p<0.0001).
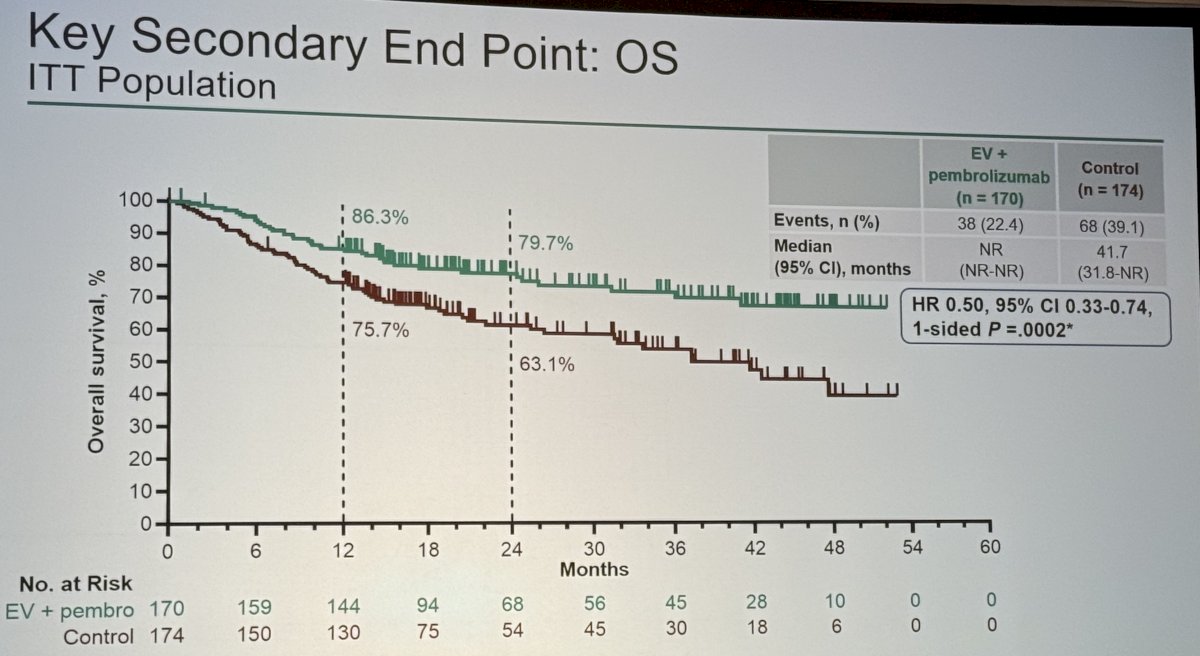
OS is a key secondary endpoint, also favored EV + pembro. At 12 months, OS was 86.3% versus 75.7%. At 24 months, OS was 79.7% versus 63.1%. Median OS was not reached in either arm, with an HR of 0.50 (95% CI 0.33–0.74; 1-sided p=0.0002).
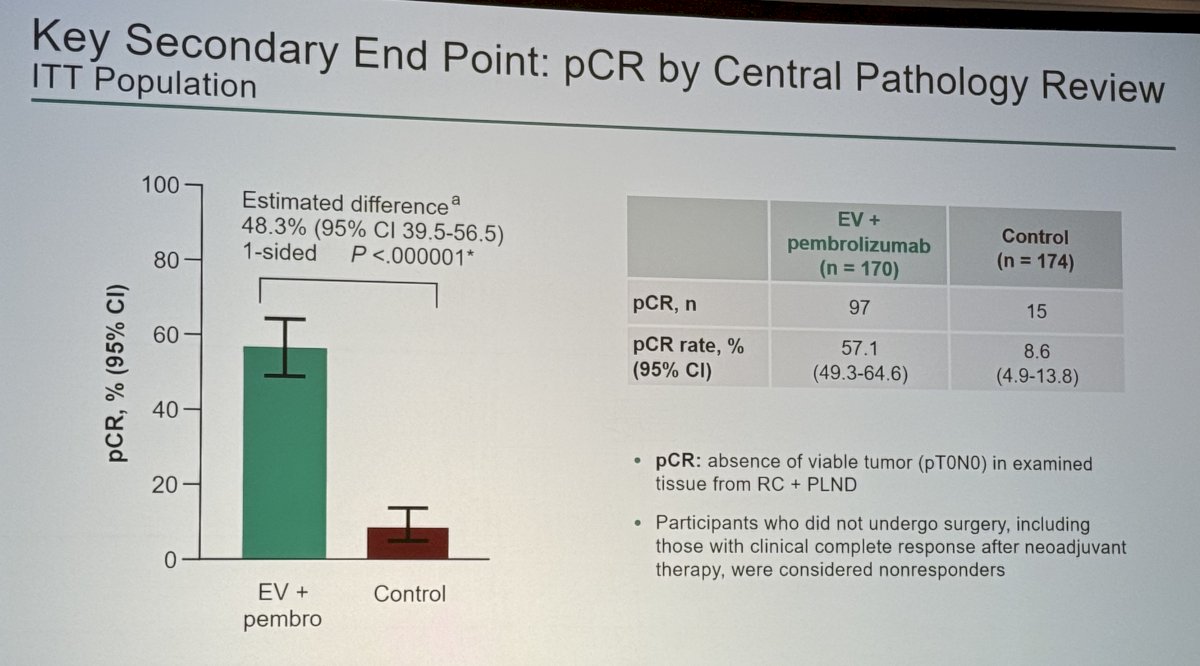
pCR was markedly higher with EV + pembro. pCR occurred in 57.1% (97/170; 95% CI 49.3–64.8) versus 8.6% (15/174; 95% CI 4.9–13.8) in the control arm, an absolute difference of 48.5% (95% CI 39.5–56.5; 1-sided p<0.000001). Participants who did not undergo RC but had clinical complete responses after neoadjuvant therapy were considered non-responders in the pCR analysis, making the magnitude of difference even more notable.
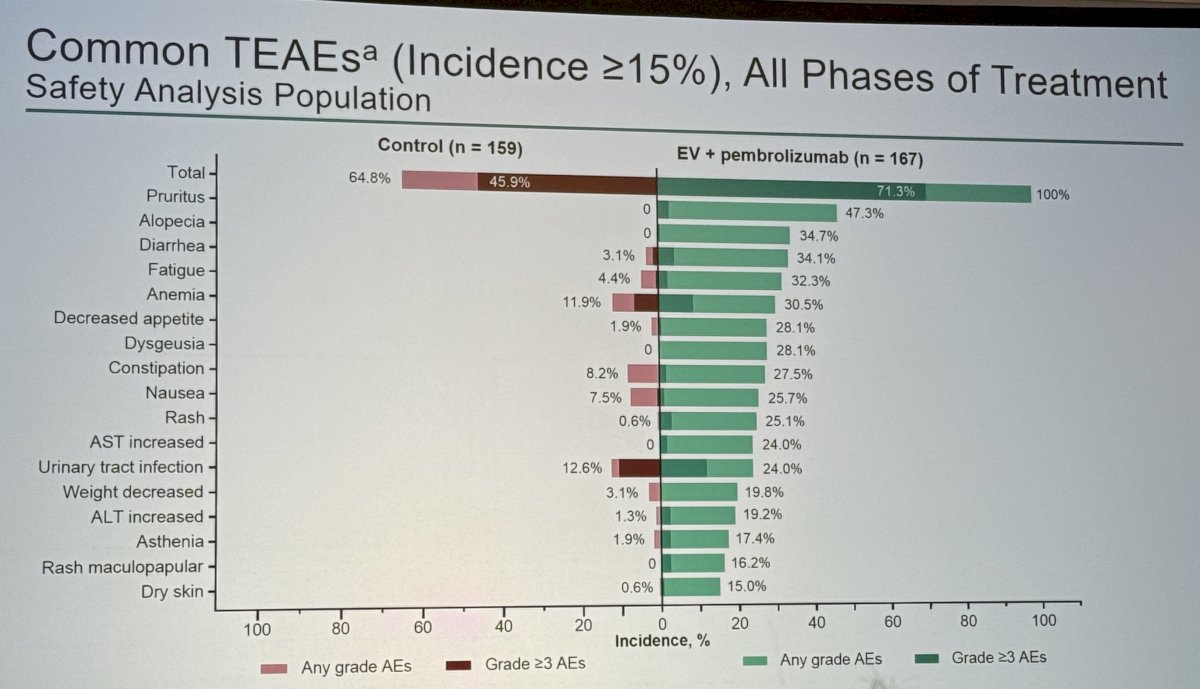
Safety across perioperative therapy was manageable and consistent with the known profiles of EV and pembrolizumab. Across all treatment phases, common treatment-emergent adverse events (TEAEs) in the EV + pembro arm included alopecia (43.7%), fatigue (37.7%), rash (32.9%), and diarrhea (27.5%), with Grade ≥3 TEAEs generally infrequent.
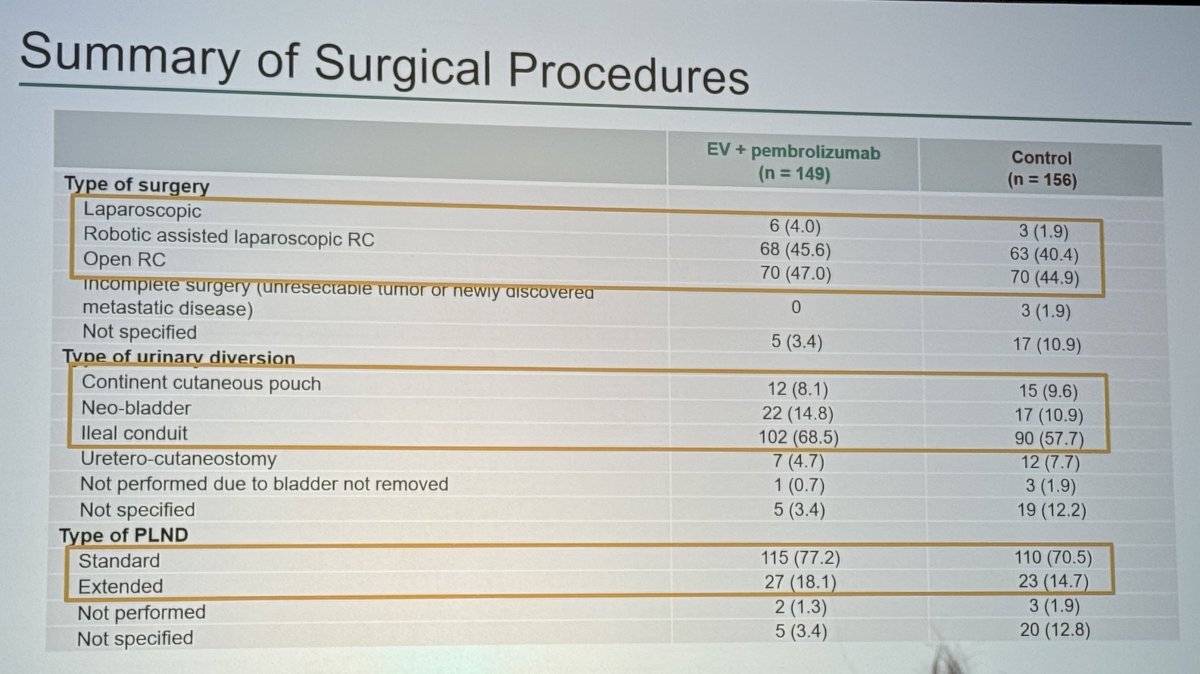
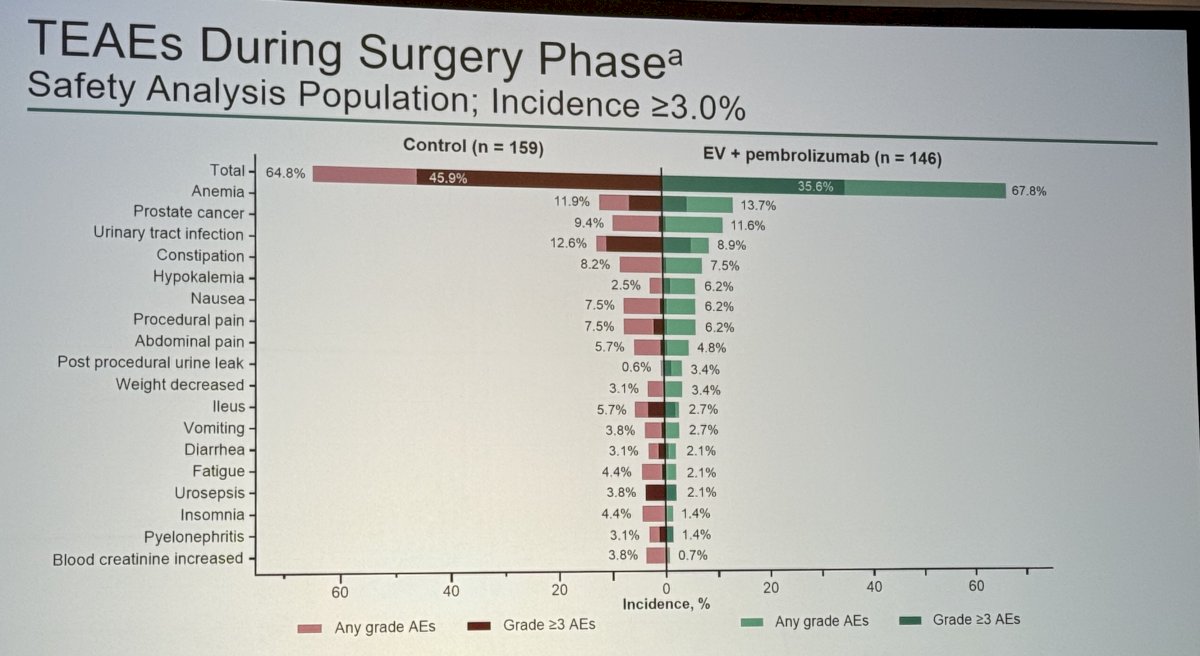
During the surgical phase, TEAEs ≥3% included anemia, urinary tract infection, and wound complications, with similar rates seen in the control arm. Surgical feasibility was preserved; 148 EV + pembro participants underwent RC, with comparable distributions of laparoscopic, robotic, and open procedures between arms. Diversion type and extent of pelvic lymph node dissection (PLND) were also similar, highlighting that neoadjuvant EV + pembro did not impair surgical candidacy.
Dr. Kaimakliotis concluded his presentation of KEYNOTE-905/EV-303, a phase III study of perioperative enfortumab vedotin plus pembrolizumab versus radical cystectomy alone in cisplatin-ineligible patients with cT2–T4aN0M0 or T1–T4aN1M0 muscle-invasive bladder cancer, as follows:
- Pre-operative EV + pembro, followed by RC and adjuvant EV + pembro, significantly and meaningfully improved EFS, OS, and pCR rate
- Neoadjuvant EV + pembro did not impact the ability of participants to undergo curative intent surgery, and time to radical cystectomy
- The safety profile of perioperative EV + pembro was manageable and consistent with prior reports of this regimen. Adverse events in the surgery phase were similar across arms
- KEYNOTE-905 is the first phase III study to show improved efficacy with perioperative therapy relative to surgery for patients who are cisplatin ineligible, offering a new treatment option in this population with high unmet clinical need, and has been approved by the US FDA
Presented by: Hristos Kaimakliotis, MD, Department of Urology, Indiana University School of Medicine, Indianapolis, IN
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, Wed, Dec 3 – Fri, Dec 5, 2025.
Related content: KEYNOTE-905 Evaluates Perioperative EV+Pembrolizumab in Cisplatin-Ineligible Bladder Cancer - Hristos Kaimakliotis