(UroToday.com) The 2025 SUO annual meeting featured a state-of-the-art session on reducing over-detection in prostate cancer and a presentation by Dr. Jeffrey Tosoian discussing the case for reflex biomarkers. To begin, Dr. Tosoian acknowledges that a pre-biopsy MRI absolutely improves the detection of clinically significant prostate cancer. According to data from Ahdoot et al.1 and the body of literature, a combination of systematic and targeted biopsies leads to a 6-13% absolute increase in clinically significant prostate cancer detection. However, there are two important considerations for reflex biomarker testing:
- There are critical limitations of MRI as a rule-out test
- There is excellent rule-out accuracy of biomarkers
A reliable rule-out test should have a high negative predictive value. For example, if a test has a 95% negative predictive value, that means that a negative result is only missing 5% of clinically significant prostate cancer. So, how good is the negative predictive value of MRI? In a 2020 systematic review and meta-analysis from Sathianathen et al.,2 they assessed 42 studies and 7,321 patients. Of note, these were predominantly academic expert centers, with zero centers classified as “community.” They defined a negative MRI as PI-RADS 1–2 and clinically significant prostate cancer as GG2+. The reference standard was biopsy or clinical follow-up. The investigators reported a pooled negative predictive value of 91% (range: 63% to 100%), but with high variability across clinical sites.
In 2019, Sonn et al.3 assessed prostate MRI interpretation variability across radiologists at Stanford University and the Palo Alto VA. There were 9 radiologists who assessed 409 patients, with a negative MRI defined as PI-RADS 1-2. They reported a low negative predictive value of 76% (range across radiologists of 40-87%), with a risk of clinically prostate cancer after a negative MRI of 24% (range across radiologists of 13-60%):
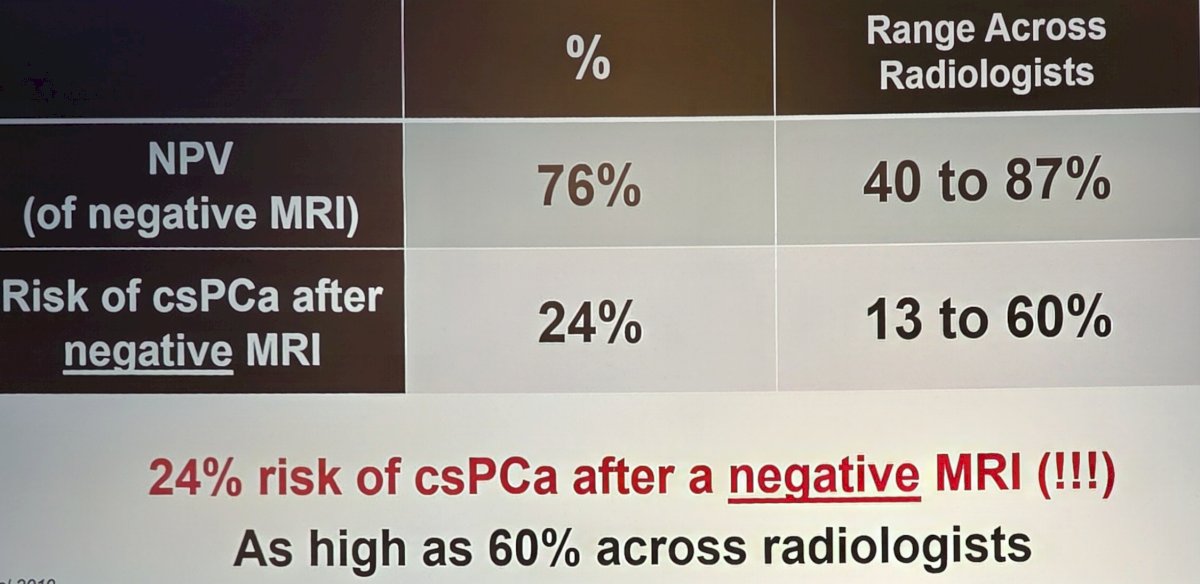
There is also low MRI negative predictive value at the statewide level based on data from the MUSIC collaborative. Among 857 patients with a negative MRI across 26 practices that underwent a prostate biopsy within 1 year of MRI, the negative predictive value was 77%, suggesting a 23% risk of clinically significant prostate cancer after a negative MRI. Dr. Tosoian notes that there are many studies in the literature suggesting high inter-reader variability in multiple settings. Based on the aforementioned data, is MRI a first-line rule-out test? Dr. Tosoian suggests, absolutely not. For example, for a patient with a PSA of 3-10 ng/mL, the risk of GG2+ prostate cancer prior to MRI is 12%, which increases to 24% (range: 13-60%) risk after a negative MRI.
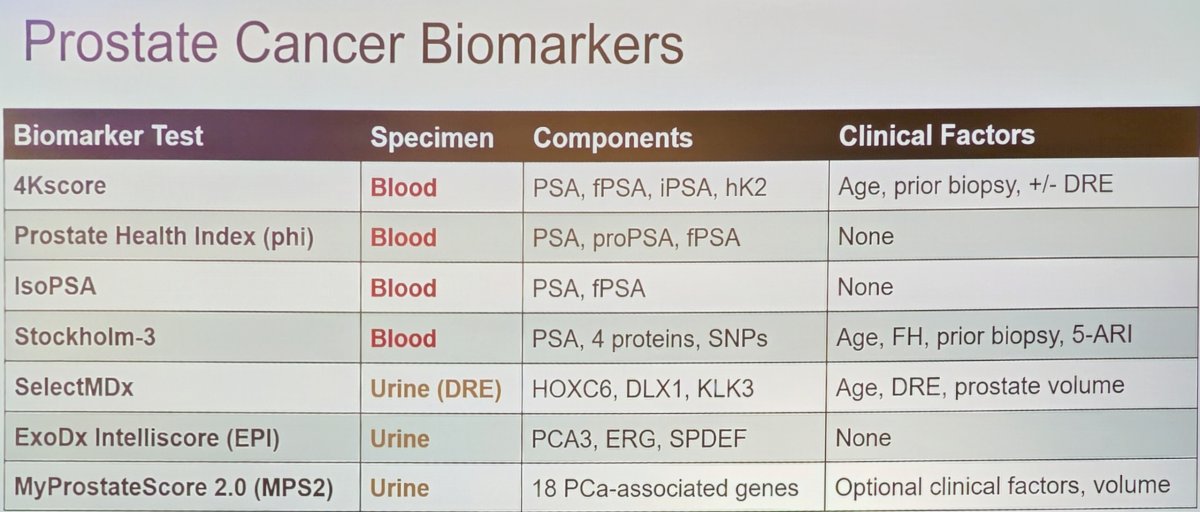
Next, Dr. Tosoian discussed the excellent rule-out accuracy of biomarkers, highlighting the following comprehensive table of available biomarker tests:
To assess the clinical data for biomarkers, Dr. Tosoian highlighted two review articles from his group,4-5 looking at blood and urine biomarkers after PSA for pre-biopsy use per the NCCN guidelines. Inclusion required validation studies in patients referred for biopsy due to elevated PSA (and/or abnormal DRE) from 2015–2025. The outcome was GG≥2 prostate cancer on biopsy, and they also reported on sensitivity and specificity (+/- negative predictive value, positive predictive value). The calculations for GG2+ based on the available literature are highlighted in the following table:
![To assess the clinical data for biomarkers, Dr. Tosoian highlighted two review articles [4-5] from his group, looking at blood and urine biomarkers after PSA for pre-biopsy use per the NCCN guidelines. Inclusion required validation studies in patients referred for biopsy due to elevated PSA (and/or abnormal DRE) from 2015–2025. The outcome was GG≥2 prostate cancer on biopsy, and they also reported on sensitivity and specificity (+/- negative predictive value, positive predictive value). The calculations for GG2+ based on the available literature are highlighted in the following table:](/images/com-doc-importer/241-suo-2025/suo-2025-reducing-over-detection-in-prostate-cancer-the-case-for-reflex-biomarkers/image-2.jpg)
Dr. Tosoian highlighted several key observations from this analysis:
- There was a consistently high negative predictive value, providing a highly accurate rule out for each patient
- There was a consistently high sensitivity, preserving immediate detection of ~93% of clinically significant prostate cancer detected under a “biopsy all” population
- There was 40% specificity, thus avoiding ~40% of unnecessary biopsies in the population
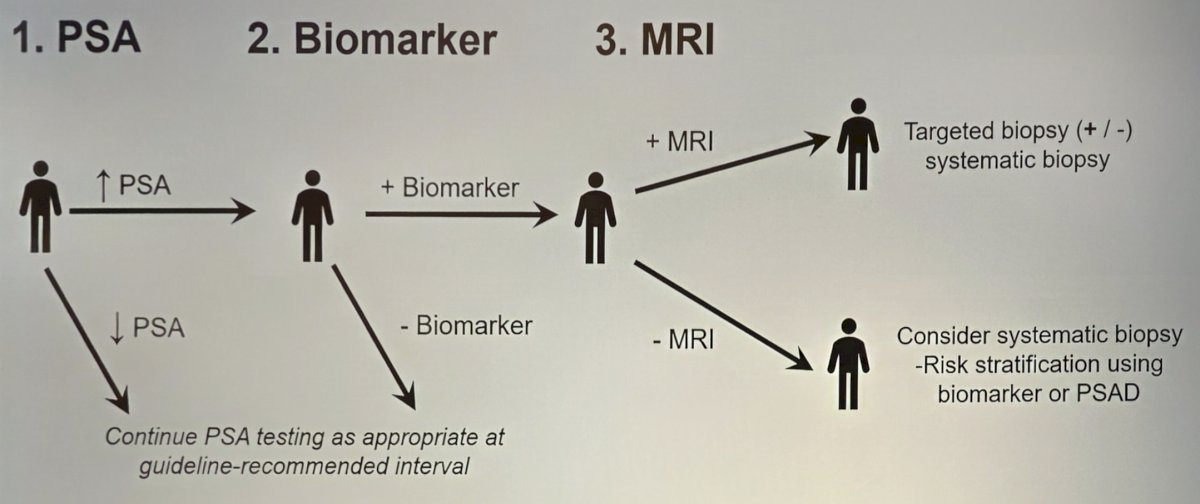
What is the optimal Approach? The optimal diagnostic approach must:
- Synergize the clinical performance strengths of both modalities
- Account for the practical attributes of testing
Regarding synergizing the clinical performance of each tool, biomarkers are highly accurate for rule-out testing, thus avoiding unnecessary biopsies. MRI is good for rule-in testing and lesion targeting, which leads to improved detection of clinically significant prostate cancer via targeted biopsy. It is also important to consider the practical factors of each tool as a first-line test:
- Biomarker practical attributes include:
- Sent from clinic (or home)
- Objective interpretation
- Readily accessible across settings
- Very few ineligible patients
- MRI practical attributes:
- Requires an additional hospital visit
- Accuracy is dependent on the radiologist
- Not available in all settings (only 32% use in 2019)
- Decreased use among rural, Hispanic, and Black patients
- Some ineligible patients (implants, claustrophobia)
- Less cost-effective (United States)
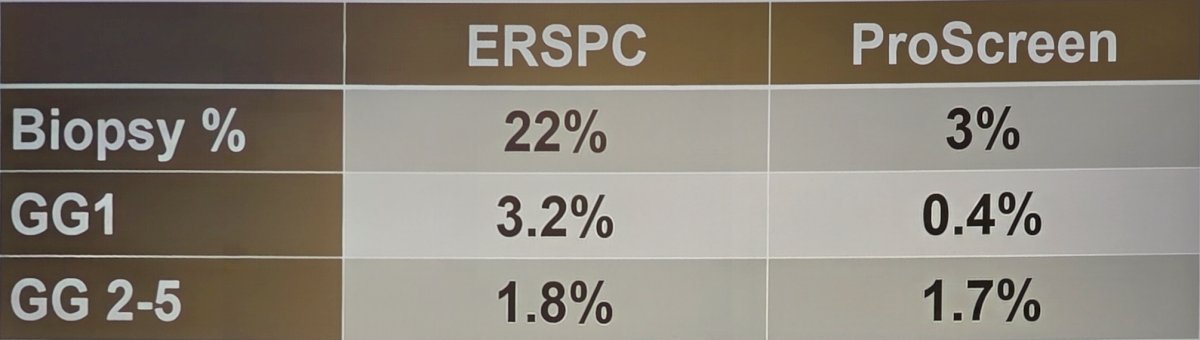
In fact, this was the same algorithm used in the recently published ProScreen Trial,6 specifically PSA, 4K panel, and MRI:
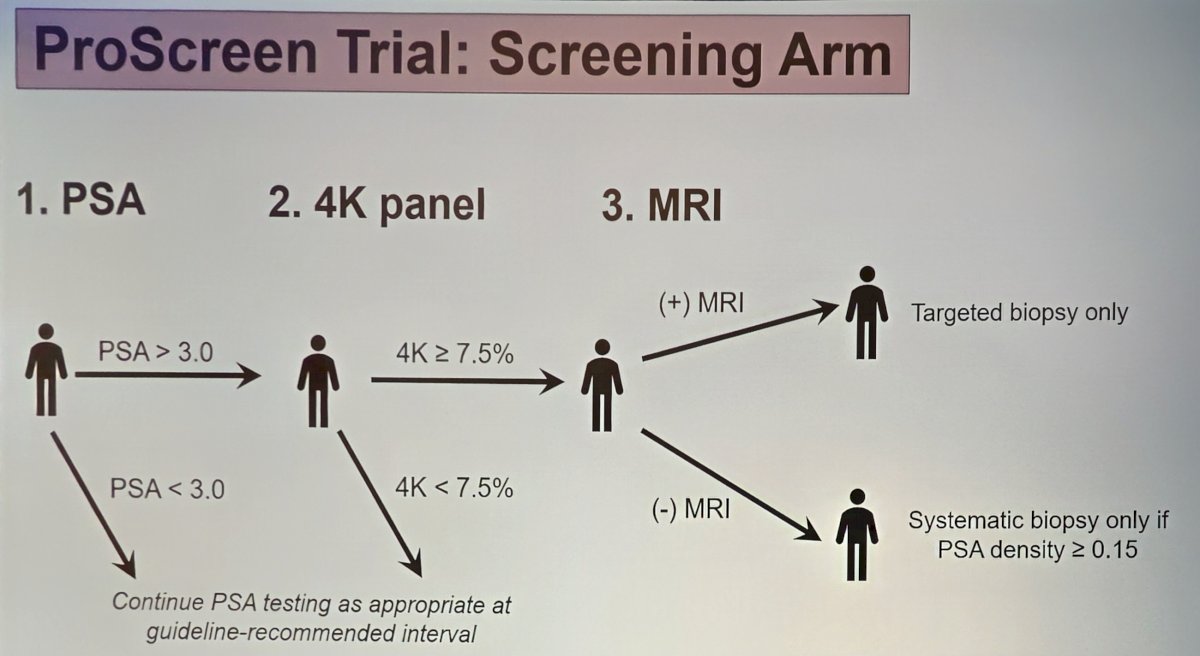
Compared to the ERSPC first rounds of screening, ProScreen had a lower biopsy rate (3% versus 22%), fewer diagnoses of GG1 prostate cancer (0.4% versus 3.2%), and the same diagnosis rate of GG 2-5 prostate cancer (1.7% versus 1.8%):
Dr. Tosoian concluded his presentation discussing the case for reflex biomarkers with the following take-home points:
- Both clinical accuracy and practical considerations favor biomarkers for first-line reflex testing in patients with elevated PSA
- High-quality MRI data support its ability to improve detection of clinically significant prostate cancer, but use as a rule-out test merits concern in many settings
- Biomarkers and MRI offer complementary strengths well-suited to sequential testing, an approach supported by ProScreen data
Presented by: Jeffrey Tosoian, MD, MPH, Vanderbilt University Medical Center, Nashville, TN
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, Wed, Dec 3 – Fri, Dec 5, 2025.
References:
- Ahdoot M, Wilbur AR, Reese SE, et al. MRI-Targeted, Systematic, and Combined Biopsy for Prostate Cancer Diagnosis. N Engl J Med. 2020 Mar 5;382(10):917-928.
- Sathianathen NJ, Omer A, Harriss E, et al. Negative predictive value of multiparametric magnetic resonance imaging in the detection of clinically significant prostate cancer in the Prostate Imaging Reporting and Data System Era: A systematic review and meta-analysis. Eur Urol. 2020 Sep;78(3):402-414.
- Sonn GA, Fan RE, Ghanouni P, et al. Prostate Magnetic Resonance Imaging Interpretation Varies Substantially Across Radiologists. Eur Urol Focus. 2019 Jul;5(4):592-599.
- Eyrich NW, Morgan TM, Tosoian JJ. Biomarkers for detection of clinically significant prostate cancer: Contemporary clinical data and future directions. Tranl Androl Urol. 2021 Jul;10(7):3091-3103.
- Robinson HS, Lee SS, Barocas DA, et al. Evaluation of blood and urine based biomarkers for detection of clinically-significant prostate cancer. Prostate Cancer Prostatic Dis. 2025 Mar;28(1):45-55.
- Auvinen A, Tammela TL, Mirtti T, et al. Prostate Cancer Screening with PSA, Kallikrein Panel, and MRI: The ProScreen Randomized Trial. JAMA. 2024 May 7;331(17):1452-1459.