(UroToday.com) The 2025 SUO annual meeting featured a bladder cancer session and a presentation by Dr. Yair Lotan discussing an overview of recommendations and risk stratification from the 2025 AUA Hematuria Guidelines. Hematuria is one of the most common urologic diagnoses, with a prevalence of 6.5% (3.4 to 12.2%).
The likelihood of an identifiable cause is 33–65% and the likelihood of cancer is <1% to 10%, with >80% of cancers identified as bladder cancer (ie. they need cystoscopy to diagnose). Unfortunately, most patients are not referred for evaluation, leading to a delay in diagnosis, and finding cancer when patients have microscopic hematuria is better than when they have gross hematuria.
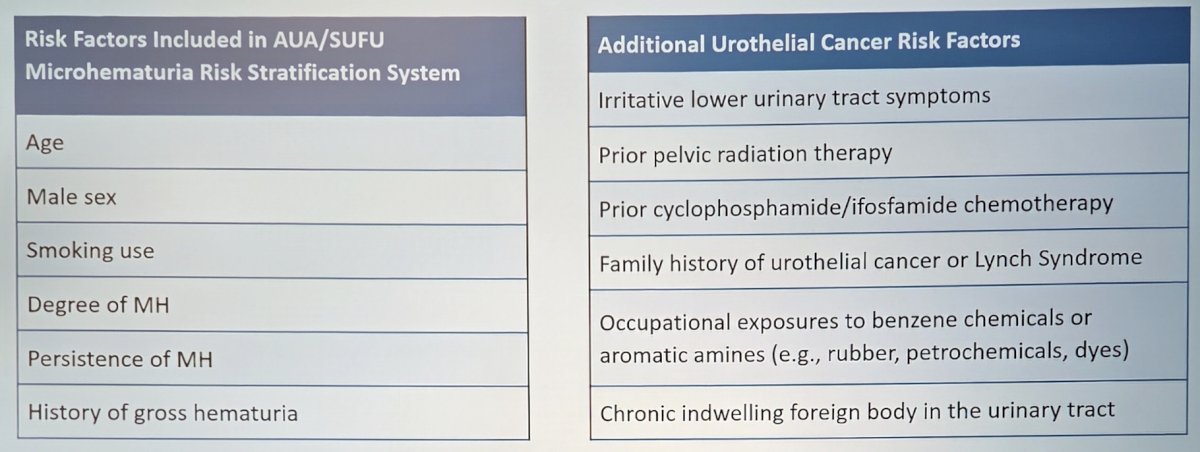
The 2025 AUA/SUFU microhematuria update started with a literature review in 2024, assessing the following risk factors:
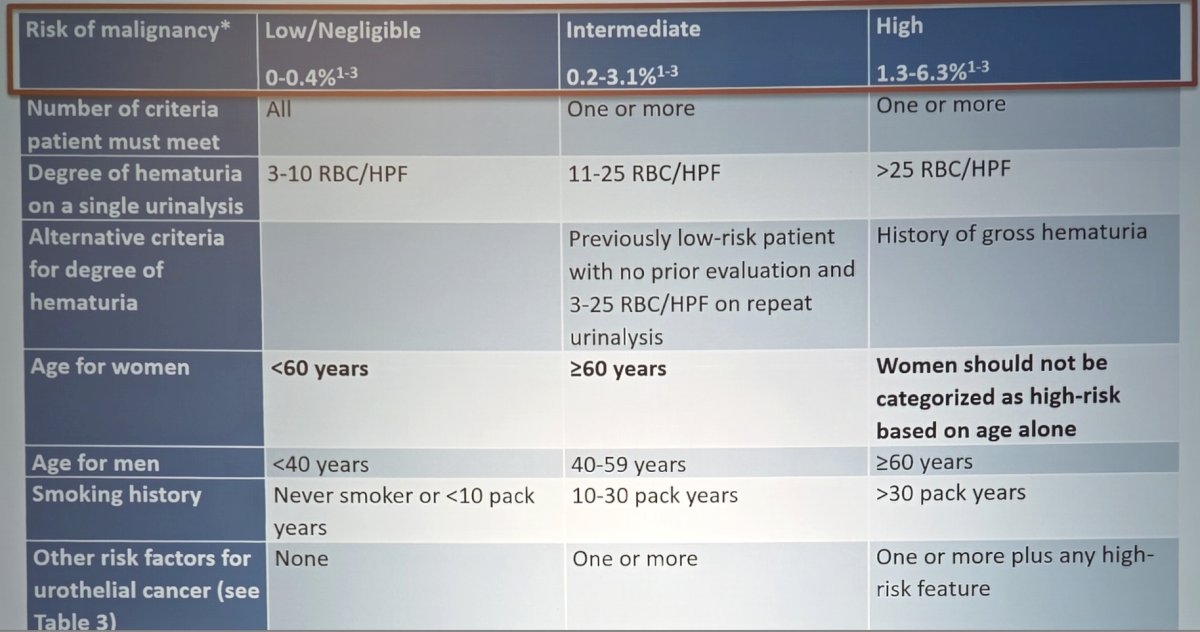
Next, Dr. Lotan highlighted changes to the risk stratification system for 2025, most notably renaming the low-risk group as low/negligible risk:
In 2021, Woldu et al.1 evaluated the 2020 AUA guideline risk classification for hematuria. This evaluation included 15,779 patients with hematuria and complete evaluation of date from the following sources:
- DETECT 1 (ClinicalTrials.gov: NCT02676180): prospective observational study of 3,556 patients referred for urologic evaluation of hematuria across 40 hospitals in UK between 2016–2017
- Initial NMP22 cohort: 1,217 prospectively and consecutively enrolled patients from 23 clinical sites between 2001–2002 in a study of the NMP22 protein
- Pacific Database cohort: 1,385 patients from several prospective cohorts evaluating the Cxbladder Detect assay in patients presenting with hematuria for urologic evaluation
- MDxHealth cohort: 1,005 prospectively enrolled patients from 6 Dutch hospitals in a study of gene methylation/mutation in urine samples
- Cepheid Cohort: 906 prospective patients from 22 multinational sites in the GeneXpert® Bladder Cancer Detection Assay
- NMP22 BladderChek cohort: 378 prospectively enrolled patients from 3 academic centers
- Kaiser Permanente: This prospective maintained cohort included 7,322 patients within an integrated healthcare system in Southern California between 2009-2015
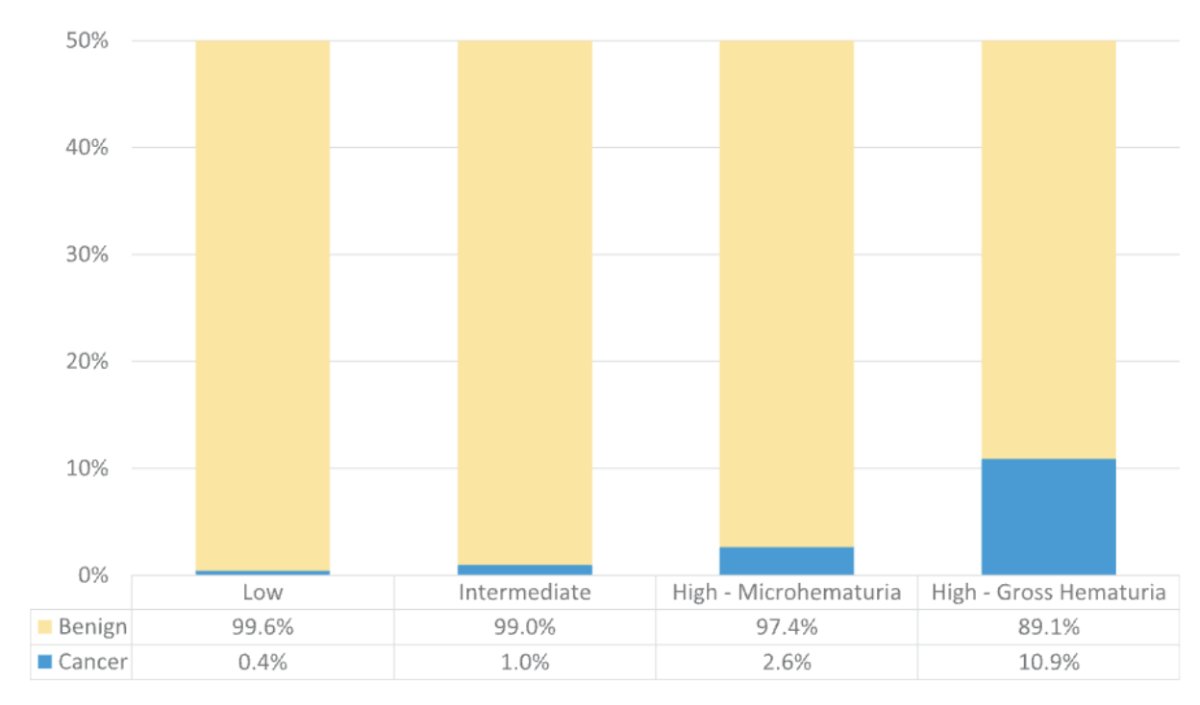
This study found cancer incidence in low-risk patients of 0.4%, 1.0% for intermediate-risk, 2.6% for high-risk microhematuria, and 11.0% for gross hematuria:
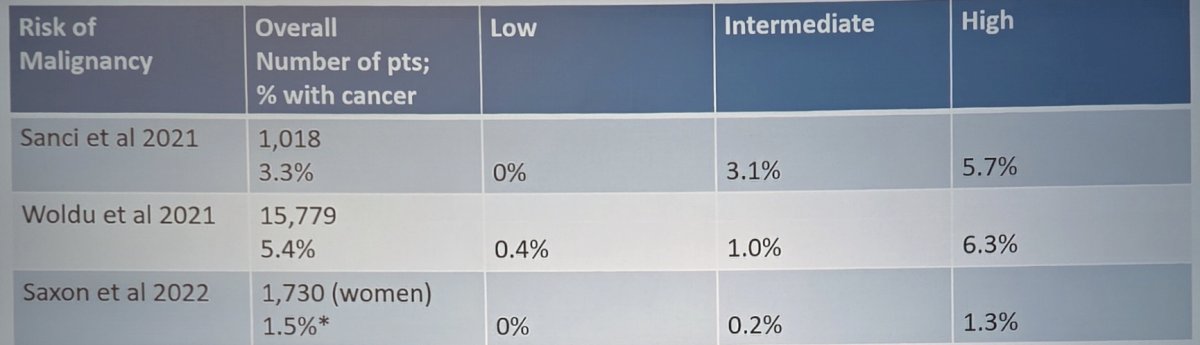
In 2021, Sanci et al. [2] provided a comparison of the 2012 and 2020 microscopic hematuria guidelines. This analysis included 1,018 men and women who presented with microscopic hematuria (defined as ≥3 or more RBC/HPF on urinalysis in the absence of an obvious benign cause). All patients underwent cystoscopy and urinary tract imaging, and urinary tract malignancy was detected in 34 patients (3.3%). Patients were risk-stratified according to the 2020 AUA/SUFU guidelines, with the following cancer detection rates:
- Low risk: 21.4% (n=218); cancer rate: 0%
- Intermediate risk: 43.9% (n=447); cancer rate: 3.1%
- High risk: 34.6% (n=353); cancer rate: 5.7%
With regards to microhematuria in women, Dr. Lotan highlighted a retrospective study of 1,730 women evaluated in a university-based urology practice [3]. Overall, 431 (31.3%) of women included in the study were considered inappropriate referrals, given that they had a dipstick alone or had <3 RBC/HPF on urinalysis with microscopy. There were 13 genitourinary malignancies identified, including 9 renal cell carcinomas and 4 bladder cancers.
Based on the aforementioned studies assessing the 2020 microhematuria guidelines, the low-risk group is actually really low risk:
The updated AUA guidelines suggest that for low/negligible-risk patients with microhematuria, “clinicians should obtain repeat UA within six months rather than perform immediate cystoscopy or imaging. (Moderate Recommendation; Evidence Level: Grade C)” The Sanci et al. [2] study followed low-risk patients for a median of 26 months, and no additional cancers were identified. However, there may be scenarios in which cystoscopy in low/negligible-risk patients may be warranted based on symptoms, clinical suspicion, or patient preference. Given the intermittent nature of hematuria, guidelines recommend a repeat urinalysis with subsequent risk-based evaluation.
For intermediate risk patients, the 2025 AUA guidelines state that “clinicians should recommend cystoscopy and renal ultrasound in patients with microhematuria categorized as intermediate risk for malignancy. (Strong Recommendation; Evidence Level: Grade C)”
Dr. Lotan then discussed upper tract imaging, and the goal in microhematuria patients is to identify malignancies of the renal parenchyma and upper tract urothelium as well as to identify actionable non-malignant diagnoses of the kidney, collecting system, and ureters. The overall risk of renal parenchymal cancer and upper tract urothelial carcinoma is low across many studies, and generally <1% risk. Looking at CT urogram versus ultrasound, CT urography provides excellent delineation of the excretory urinary tract, is very sensitive for urinary stones, readily identifies renal cortical lesions, and provides extra-urinary information. However, a CT urogram is (i) more expensive than renal ultrasound, (ii) involves ionizing radiation, and (iii) includes iodine-based intravenous contrast. Renal ultrasonography is (i) less expensive, (ii) has no radiation, (iii) provides reasonable discrimination for cortical lesions, (iv) but can miss small upper tract urothelial carcinoma, bladder and kidney tumors, as well as small stones.
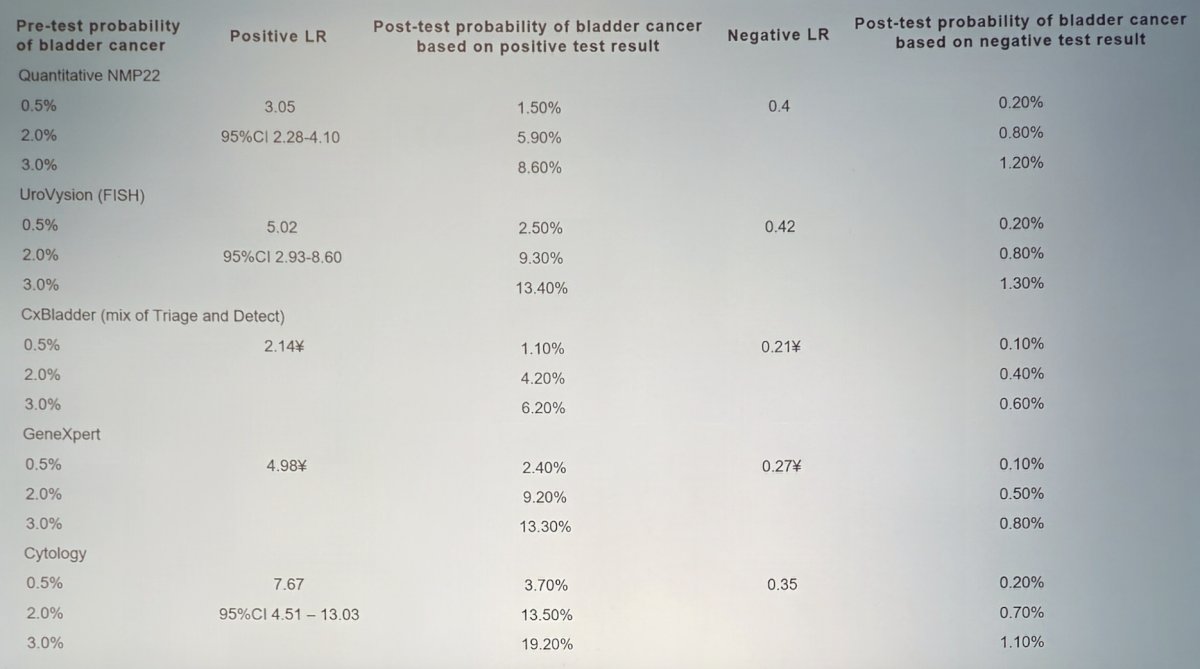
The AUA guidelines also state that “for appropriately counseled intermediate-risk patients who want to avoid cystoscopy and accept the risk of forgoing direct visual inspection of the bladder urothelium, clinicians may offer urine cytology or validated urine-based tumor markers to facilitate the decision regarding the utility of cystoscopy. Renal and bladder ultrasound should still be performed in these cases. (Conditional Recommendation; Evidence Level: Grade C).” Dr. Lotan notes that the gold standard to evaluate for bladder cancer is cystoscopy, but urine-based tumor markers and urine cytology were developed to provide a non-invasive method to detect urothelial carcinoma. In an analysis of 11 studies, with study populations of 8,302 patients for cytology evaluation and ranging from 354–6,474 patients for the commercially available urine markers, the likelihood of cancer is impacted by the prevalence of disease and performance of the biomarker. Dr. Lotan provided the following table highlighting the available urine-based tumor markers:
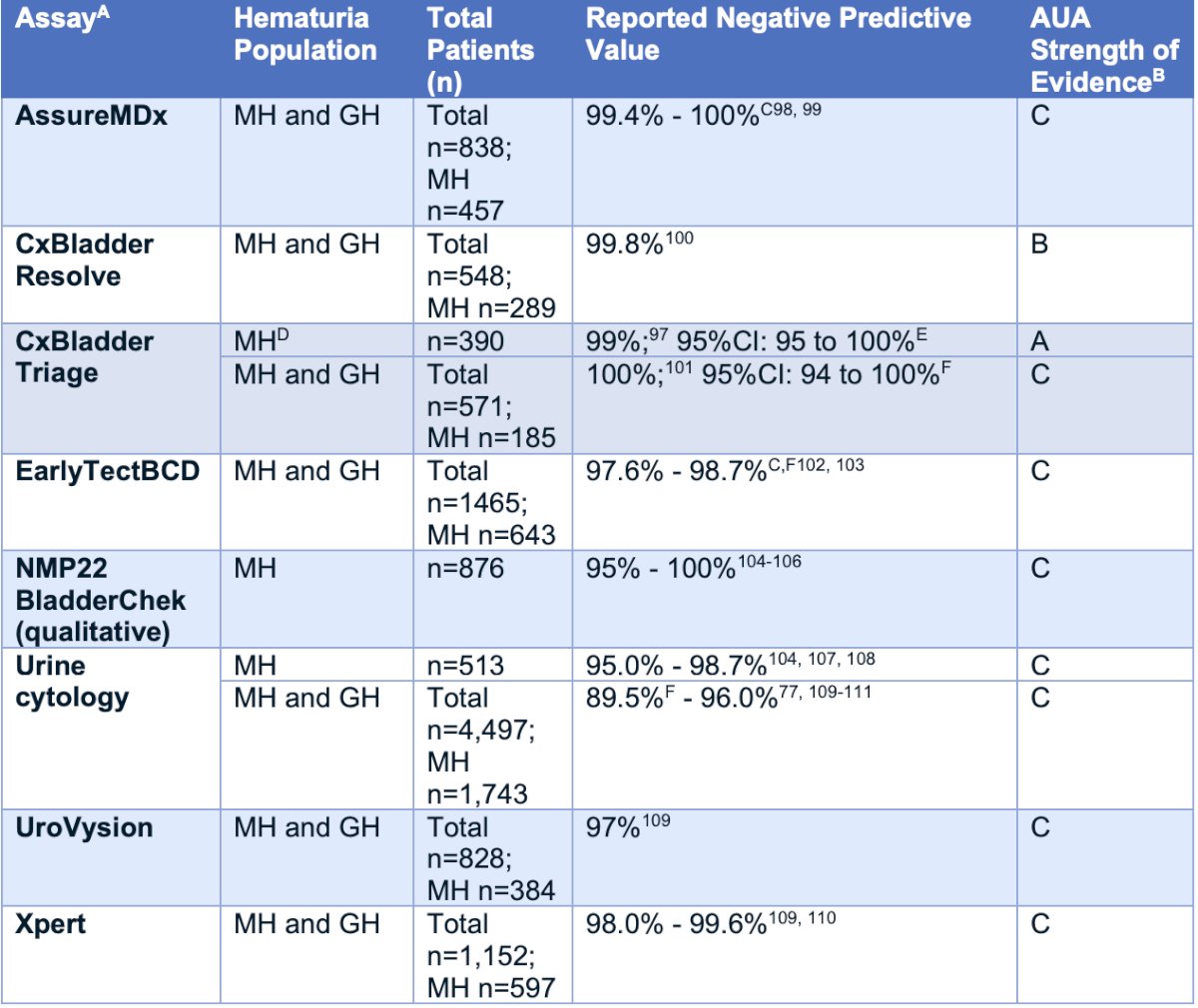
The following table from the AUA 2025 guidelines highlights the reported negative predictive values for the detection of bladder cancer using the available urine cytology and urine-based biomarkers:
For intermediate risk patients, the AUA guidelines state that “patients who do not undergo cystoscopy based on urinary marker results, clinicians should obtain a repeat urinalysis within 12 months. Such patients with persistent microhematuria should then undergo cystoscopy. (Strong Recommendation; Evidence Level: Grade C).” Additionally, “Clinicians should not routinely use urine cytology or urine-based tumor markers to decide whether to perform cystoscopy in the initial evaluation of low/negligible- or high-risk patients with microhematuria. (Strong Recommendation; Evidence Level: Grade C).” For low/negligible-risk patients, they have a very low probability of harboring cancer, and any marker would lead to many additional workups unless the specificity is nearly perfect. For high-risk patients, the overall incidence of cancer is relatively high. At present, there is insufficient evidence to demonstrate the safety and efficacy of using marker results to exclude the need for cystoscopy in the initial evaluation of high-risk patients.
For follow-up, the AUA guidelines state that “in patients with a negative risk-based hematuria evaluation, clinicians should engage in shared decision making regarding whether to repeat a urinalysis in the future. (Strong Recommendation; Evidence Level: Grade C).” Additionally, “for high-risk patients with microhematuria who have a family history of renal cell carcinoma, a known genetic renal tumor syndrome, or a personal or family history of (or suspicious for) Lynch syndrome, clinicians should perform upper tract imaging regardless of risk category. (Expert Opinion)” These known genetic renal tumor syndromes include:
- von Hippel-Lindau
- Birt-Hogg-Dube
- Hereditary Papillary RCC
- Hereditary Leiomyomatosis Renal Cell Cancer
- Tuberous sclerosis
Dr. Lotan concluded his presentation discussing an overview of recommendations and risk stratification from the 2025 AUA Hematuria Guidelines with the following take-home points:
- There is a high prevalence of microhematuria
- Most patients currently do not get any evaluation
- 25% of bladder cancer is diagnosed when muscle invasion is present (rate unchanged)
- We need to improve referral patterns and improve risk stratification, with hopefully practical guidelines to improve compliance
Presented by: Yair Lotan, MD, Urologic Oncologist, UT Southwestern Medical Center, Dallas, TX
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, Wed, Dec 3 – Fri, Dec 5, 2025.
References:
- Woldu SL, Ng CK, Loo RK, et al. Evaluation of the new American Urological Association Guidelines Risk Classification for Hematuria. J Urol. 2021 May;205(5):1387-1393.
- Sanci A, Oktar A, Gokce MI, et al. Comparison of Microscopic Hematuria Guidelines as Applied in 1018 Patients with Microscopic Hematuria. Urology. 2021 Aug;154:28-32.
- Saxon GM, Patil D, Hammett J. Microhematuria in Women: Prevalence of Malignancy and Risk Score Evaluation. Urology. 2022 Feb;160:34-39.
- Ghandour R, Freifeld Y, Singla N, et al. Evaluation of Hematuria in a Large Public Health Care System. Bladder Cancer. 2019;5(2):119-129.