(UroToday.com) The 2025 SUO annual meeting featured a state-of-the-art session on reducing over-detection in prostate cancer and a presentation by Dr. Peter Pinto discussing the case for reflex imaging, and why MRI, and emerging imaging tools, should guide first-line diagnostic pathways in prostate cancer.
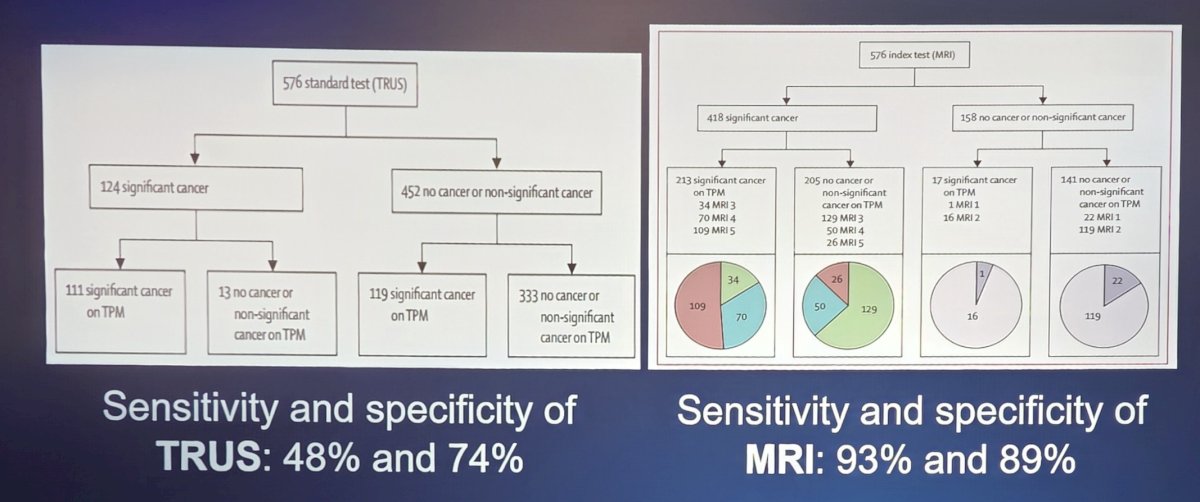
Dr. Pinto started by emphasizing that the 12-core systematic “blind” prostate biopsy has low sensitivity and specificity in detecting clinically significant cancer. This is secondary to potentially only sampling 0.04% of gland, difficulty sampling anterior and apical regions, and less effectiveness in patients with prior negative biopsy. When assessing ultrasound versus MRI, the sensitivity and specificity of TRUS is 48% and 74%, respectively, and for MRI in the PROMIS trial1 was 93% and 89%, respectively:
With regards to MRI targeted prostate biopsy, advances in MRI technology have taken the “blindfold” off urologists, resulting in a new era of cancer detection beyond TRUS. In 2015, Dr. Pinto’s group compared MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer.2 This was a prospective study of 1,003 men (all suspected or newly diagnosed prostate cancer) undergoing both MRI tumor-targeted and standard 12-core TRUS biopsy in the same biopsy session. The results were as follows:
- MRI-targeted biopsy diagnosed 30% more high-risk cancer
- MRI-targeted biopsy diagnosed 17% fewer low-risk cancer
- The benefit of a treatment decision based on the biopsy type favored MRI-targeted biopsy
Dr. PINTO then discussed PRECISION,3 which assigned 500 men with a clinical suspicion of prostate cancer who had not previously undergone a prostate biopsy to undergo MRI with or without a targeted biopsy vs standard TRUS-guided biopsy. Men in the MRI group underwent a targeted biopsy if there was a suspicion of prostate cancer on imaging, and did not undergo a biopsy if the MRI was negative. The primary outcome for this randomized clinical trial was a diagnosis of clinically significant prostate cancer. In the MRI-targeted biopsy group, 28% had a negative MRI and thus no biopsy. Among men undergoing targeted biopsy, 38% had clinically significant cancer, compared to 26% in the TRUS-guided biopsy group (p = 0.005). Furthermore, fewer men in the MRI-targeted biopsy group had clinically insignificant prostate cancer compared to the TRUS-guided biopsy group.
Dr. Pinto notes that without reflex imaging, the biopsy misses aggressive cancers, which leads to uncertainty and doubt. The ramifications of uncertainty leading to over-treatment is that there are (i) high rates of upgrading at prostatectomy, (ii) approximately 30% rate of missed diagnoses, and (iii) 43% of prostatectomies are done for men ultimately confirmed to have Gleason 6 disease. Reducing this uncertainty will give the patient and urologist more confidence to enroll in active surveillance or focal therapy.
In 2020, Ahdoot et al.4 assessed 2,103 men undergoing both MRI tumor-targeted and systematic 12-core TRUS biopsy during the same biopsy session. Ultimately, 404 men underwent radical prostatectomy, with a primary endpoint of cancer detection according to Gleason grade group, and among those who underwent radical prostatectomy, upgrading and downgrading of grade group from biopsy to whole-mount histopathology. The authors found that cancer was diagnosed in 1,312 (62.4%) by a combination of the two methods, and 404 (19.2%) men underwent radical prostatectomy. Cancer detection rates on MRI-targeted biopsy were significantly lower than on systematic biopsy for grade group 1 cancers and significantly higher for grade groups 3 through 5 (p<0.01 for all comparisons). Combined biopsy led to cancer diagnoses in 208 more men (9.9%) than with either method alone and to upgrading to a higher grade group in 458 men (21.8%). However, if only MRI-target biopsies had been performed, 8.8% of clinically significant cancers (grade group ≥3) would have been misclassified. Among the 404 men who underwent subsequent radical prostatectomy, combined biopsy was associated with the fewest upgrades to grade group 3 or higher on histopathological analysis of surgical specimens (3.5%), as compared with MRI-targeted biopsy (8.7%) and systematic biopsy (16.8%)
Dr. Pinto noted that urologists can now provide themselves and their patients with increased confidence in the shared decision for choosing active surveillance or focal therapy. Additionally, according to the early detection of prostate cancer AUA/SUO 2023 guideline, the following two statements are important:
- When screening for prostate cancer, clinicians should use PSA as the first screening test. (Strong Recommendation; Evidence Level: Grade A)
- Clinicians may use MRI prior to initial biopsy to increase the detection of GG2+ prostate cancer. (Conditional Recommendation; Evidence Level: Grade B)
Finally, Dr. Pinto discussed the recently published OPTIMUM randomized trial assessing micro-ultrasonography versus MRI-guided biopsy for prostate cancer diagnosis.5 This was a multicenter, international, open-label, randomized noninferiority trial of biopsy-naive men from 20 centers (678 men underwent biopsy). The primary endpoint was detection of GG2 or higher cancers using micro-ultrasonography + systematic biopsy versus MRI/conventional ultrasonography + systematic biopsy, with a non-inferiority margin set at 10%. This trial found that GG2 or higher cancer was detected in 47.1% of micro-ultrasonography group, 42.6% in the MRI/conventional ultrasound group, and 46.9% in MRI/ultrasound/MRI group. Ultimately, micro-ultrasonography-guided biopsy was noninferior to MRI fusion biopsy with a difference of 3.52% (p<0.001).
Dr. Pinto concluded his presentation discussing the case for reflex imaging with the following take-home points:
- MRI reflex imaging outperforms TRUS systematic in clinically significant prostate cancer detection in multiple large institutional trials
- Micro-ultrasonography reflex imaging shows promise but needs corroborative evidence to show reproducibility
- Reflex imaging should be considered as a standard component of contemporary prostate cancer diagnostic pathways
Presented by: Peter Pinto, MD, National Cancer Institute, National Institutes of Health, Bethesda, MD
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Society of Urologic Oncology (SUO) Annual Meeting, Phoenix, AZ, Wed, Dec 3 – Fri, Dec 5, 2025.
References:
- Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): A paired validating confirmatory study. Lancet 2017;389(10071):815-822.
- Siddiqui MM, Rais-Bahrami S, Turkbey B, et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA. 2015 Jan 27;313(4):390-397.
- Kasivisvanathan V, Rannikko AS, Borghi M, et al. MRI-targeted or standard biopsy for prostate cancer diagnosis. N Engl J Med 2018;378(19):1767-1777.
- Ahdoot M, Wilbur AR, Reese SE, et al. MRI-Targeted, Systematic, and Combined Biopsy for Prostate Cancer Diagnosis. N Engl J Med. 2020 Mar 5;382(10):917-928.
- Kinnaird A, Luger F, Cash H, et al. Microultrasonography-Guided vs MRI-Guided Biopsy for Prostate Cancer Diagnosis: The OPTIMUM Randomized Clinical Trial. JAMA. 2025 May 20;333(19):1679-1687.