WSAUA 2025
WSAUA 2025
WSAUA 2025: Impact of Neoadjuvant Systemic Therapy on Tumor and Tumor Thrombus Regression in Renal Cell Carcinoma with Venous Involvement: A Retrospective Analysis
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a kidney cancer session and a presentation by Jaxson Jeffery discussing the impact of neoadjuvant systemic therapy on tumor and tumor thrombus regression in renal cell carcinoma (RCC) with venous involvement. The utility of neoadjuvant systemic therapy in RCC with inferior vena cava (IVC) tumor thrombus is inadequately defined.
WSAUA 2025: Long-Term Outcomes of Primary Chemoablation of New-Onset or Recurrent Low Grade Upper Tract Urothelial Carcinoma with UGN-101, a Mitomycin Reverse Thermal Gel
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a urothelial carcinoma session and a presentation by Dr. Karim Chamie discussing long-term outcomes of primary chemoablation of new-onset or recurrent low-grade upper tract urothelial carcinoma with UGN-101. Endoscopically guided ablation is commonly used to treat low-grade upper tract urothelial carcinoma. Surgical ablation is effective, but not typically durable, requiring long-term endoscopic surveillance associated with potential complications.
WSAUA 2025: CHAI Analysis of High-Grade Ta Non Muscle Invasive Bladder Cancer Risk Stratification for Progression and Recurrence Across Subgroups
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a urothelial carcinoma session and a presentation by Dr. Siamak Daneshmand discussing computational histology artificial intelligence (CHAI) analysis of high-grade (HG) Ta non-muscle invasive bladder cancer risk stratification for progression and recurrence across subgroups.
WSAUA 2025: Treatment of Low Grade Intermediate Risk Non Muscle Invasive Bladder Cancer With UGN-102: Outcomes From the 5-year Long-Term Extension Study of the Single-Arm, Phase 2b Optima II Study
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a urothelial carcinoma session and a presentation by Dr. Jay Raman discussing 5-year outcomes of the phase 2b Optima II study assessing the treatment of low-grade intermediate-risk non-muscle invasive bladder cancer with UGN-102.
WSAUA 2025: Comparative Performance of UNFOLD AI, PSMA-PET, and mpMRI for Prostate Cancer Localization and Pathologic Staging
- Details
(Urotoday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Austin W. Lee, MD, discussing the comparative performance of Unfold AI, PSMA-PET, and mpMRI for prostate cancer localization and pathologic staging. Over the last several years, there has been a wealth of data assessing the ability of artificial intelligence and new imaging modalities to improve prostate cancer risk stratification. As such, the objective of this study, presented at the 2025 Western Section AUA annual meeting, was to evaluate the diagnostic performance of Unfold AI compared to PSMA-PET and mpMRI in detecting clinically significant prostate cancer and extraprostatic extension, using whole-mount histopathology as ground truth.
In this study, 30 patients with intermediate- to high-risk prostate cancer underwent mpMRI, PSMA-PET, and radical prostatectomy. Unfold AI, an artificial intelligence-driven localization model, produced probabilistic cancer maps from mpMRI and clinical inputs. Each modality was evaluated for cancer localization and T-staging performance against histologic standards using ROC analysis.
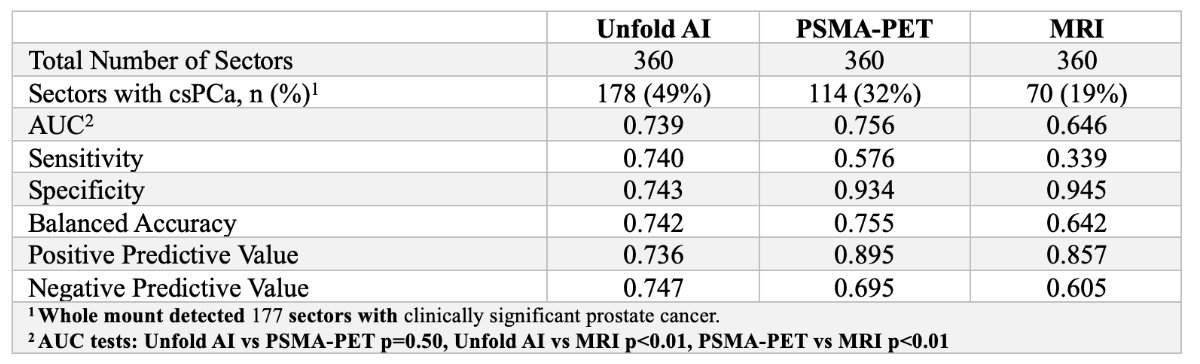
For clinically significant cancer, localization AUCs were: Unfold AI 0.7386, PSMA-PET 0.7562, and mpMRI 0.6461:
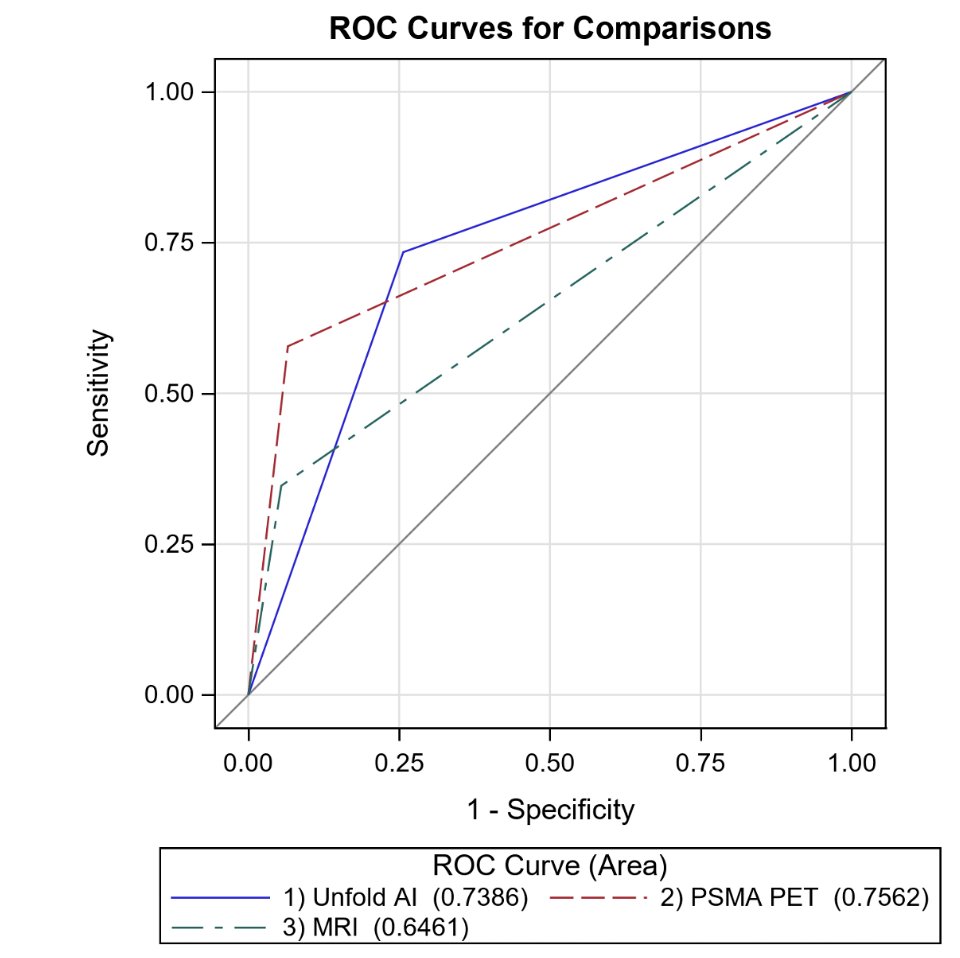
Unfold AI was not significantly different from PSMA-PET (p = 0.50), but significantly better than mpMRI (p < 0.01). Additionally, PSMA-PET outperformed mpMRI (p < 0.01):
For extraprostatic extension detection, Unfold AI (AUC 0.7476) outperformed both PSMA-PET (AUC 0.5681) and mpMRI (AUC 0.6490) (both p<0.01):

PSMA-PET was also inferior to mpMRI for T-staging (p = 0.05):
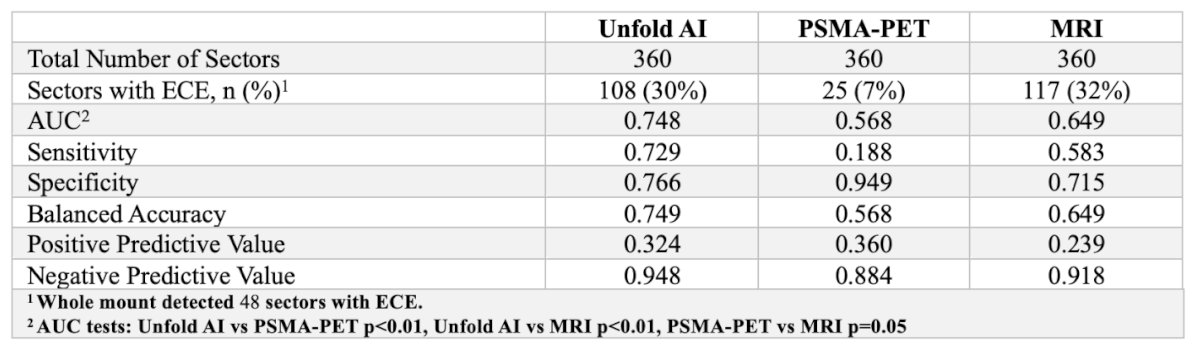
Unfold AI achieved high balanced accuracy for both tasks: localization (AUC 0.742) and extraprostatic extension (AUC 0.749).
Dr. Lee concluded his presentation discussing the comparative performance of UNFOLD AI, PSMA-PET, and mpMRI for prostate cancer localization and pathologic staging with the following take-home points:
- Unfold AI offers comparable accuracy to PSMA-PET and significantly outperforms mpMRI for clinically significant cancer localization
- Unfold AI also exceeded both modalities in detecting extraprostatic extension
- These findings highlight the potential of artificial intelligence-driven platforms to enhance prostate cancer staging and inform treatment planning
Presented by: Austin W. Lee, MD, UCLA, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Western Section American Urological Association (AUA) Annual Meeting, Napa Valley, CA, Sun, Nov 2 – Thurs, Nov 6, 2025.
WSAUA 2025: Head-to-Head Comparison of Multimodal Imaging in the Detection of Prostate Cancer Using Whole Mount Histopathology as a Reference
- Details
(Urotoday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Wayne G. Brisbane, MD, discussing a head-to-head comparison of multimodal imaging in the detection of prostate cancer using whole-mount histopathology as a reference. Micro ultrasound is an emerging imaging modality with promising potential to identify and target suspicious prostate cancer. Recent studies indicate that micro ultrasound can complement mpMRI when compared to biopsy pathology results. Dr. Brisbane aimed to comprehensively evaluate and compare the performance of micro ultrasound, mpMRI, and PSMA PET/CT in the detection of prostate cancer and assessment of extraprostatic extension, using whole mount histopathology as a reference.
Patients with prostate cancer who underwent micro ultrasound, mpMRI, and PSMA PET/CT prior to radical prostatectomy were included in this study:
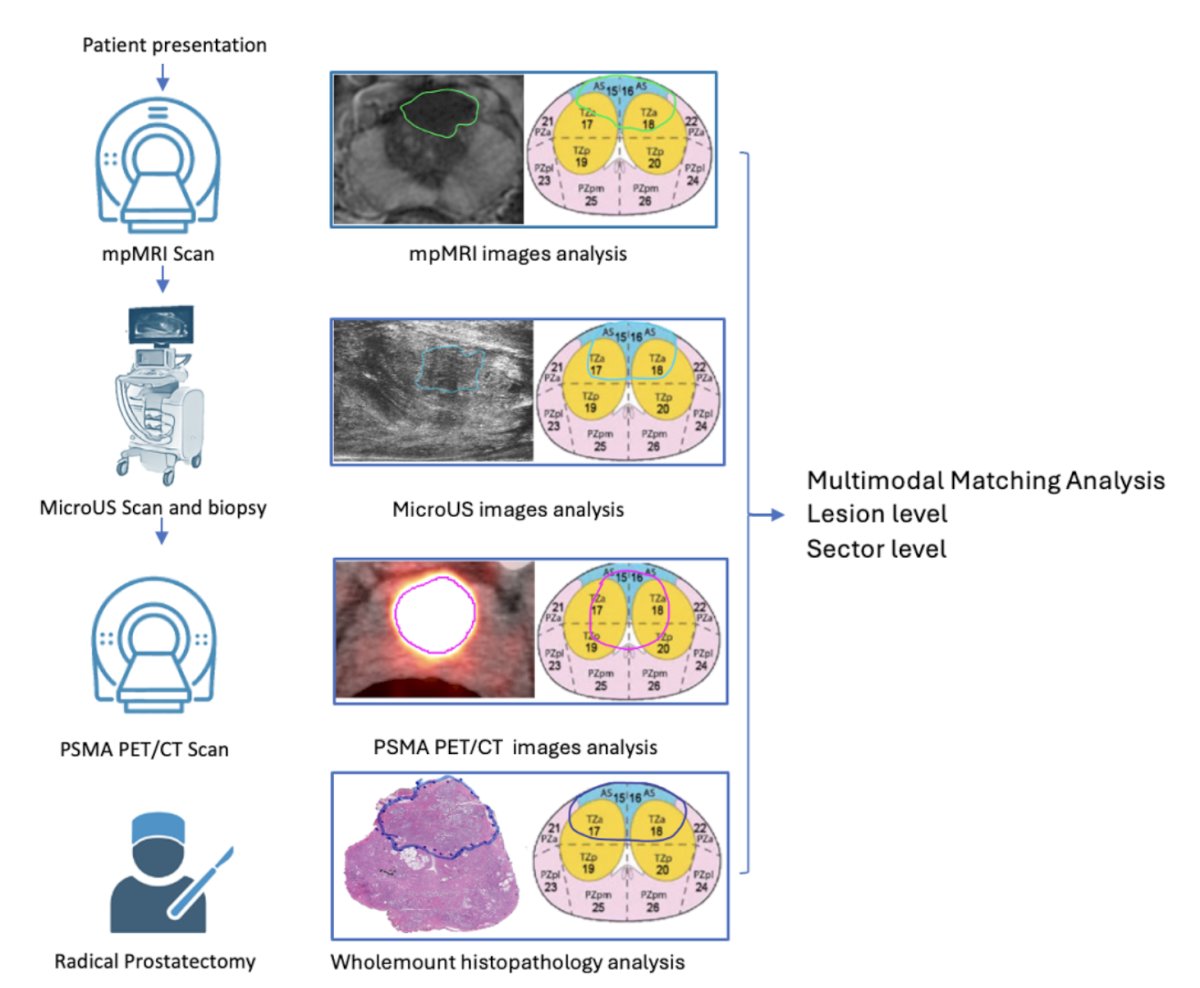
Whole-mount histopathology findings served as the reference standard. Imaging findings were mapped onto a standardized 36-sector map and correlated with whole-mount histopathology to assess prostate cancer involvement. Detection rates of prostate cancer and clinically significant prostate cancer were evaluated at both the lesion and sector levels. Diagnostic performance for detecting prostate cancer, clinically significant prostate cancer, and extraprostatic extension was assessed using receiver operating characteristic (ROC) analysis. The chi-square test and Delong test were used to compare the detection rates and area under the ROC curve (AUC) across different imaging modalities.
The study included 42 patients, of whom 20 patients (47.6%) had extraprostatic extension. Lesion-level detection rates for prostate cancer and clinically significant prostate cancer were 50% and 70% for micro ultrasound, 55% and 77% for mpMRI, and 50% and 74% for PSMA PET/CT, respectively:

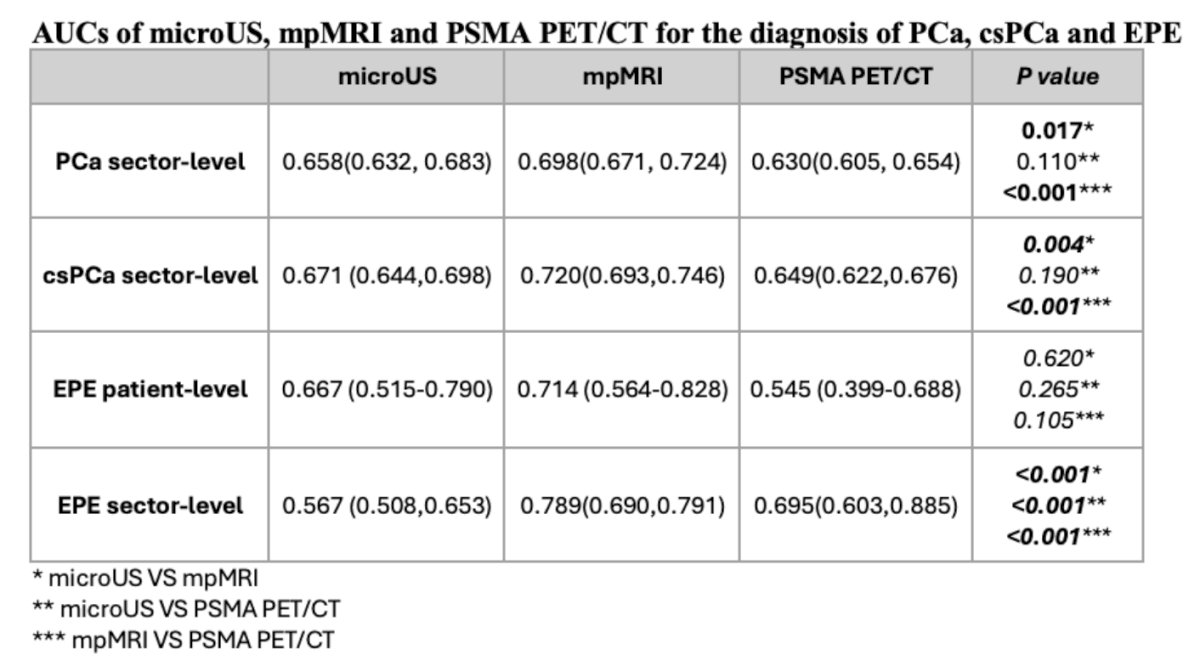
For predicting patient-level extraprostatic extension, AUCs were 0.667 (0.515-0.790) for micro ultrasound, 0.714 (0.564-0.828) for mpMRI, and 0.545 (0.399-0.688) for PSMA PET/CT. At the sector level, mpMRI outperformed micro ultrasound and PSMA PET/CT for detecting prostate cancer (AUC: 0.698 versus 0.658 and 0.630, p = 0.017/p < 0.001), clinically significant prostate cancer (AUC: 0.720 versus 0.671 and 0.649, p = 0.004/p < 0.001), and extraprostatic extension (AUC: 0.789 versus 0.567/0.695, p < 0.001/p < 0.001):
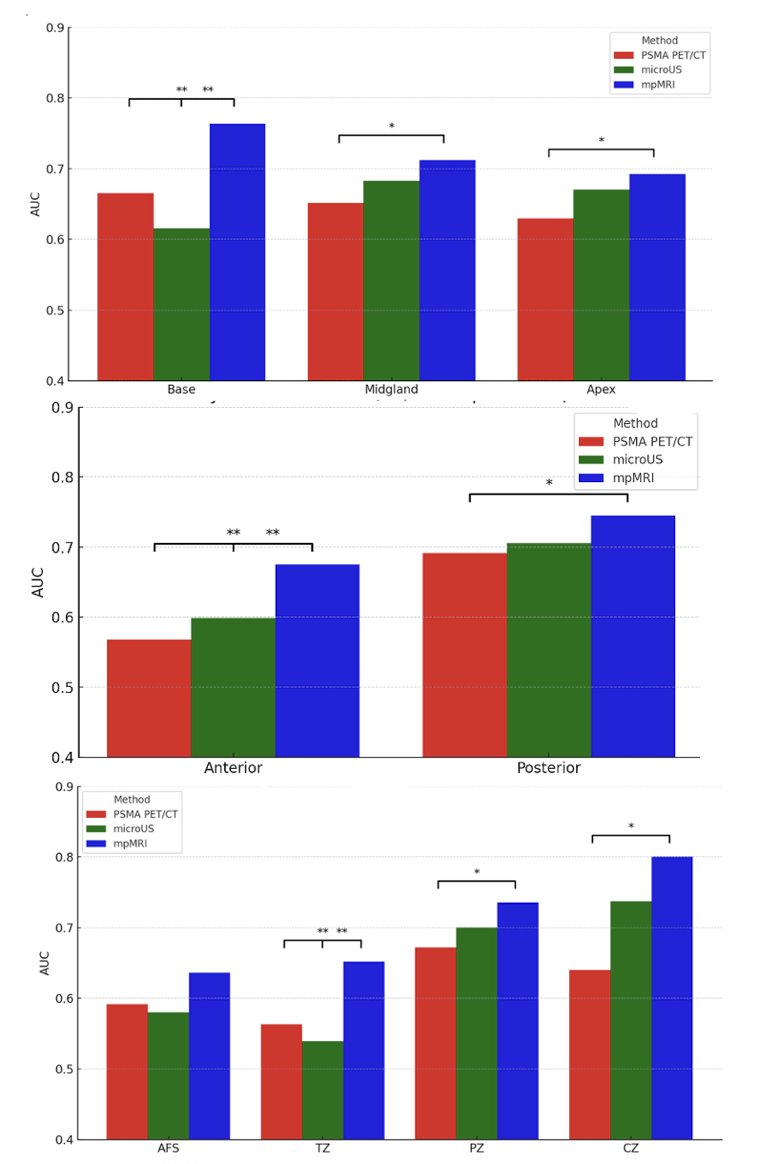
mpMRI performed better in detecting clinically significant prostate cancer in the base level, anterior part, and transition zones and in diagnosing extraprostatic extension in the base and midgland level (all p < 0.05):
Dr. Brisbane concluded his presentation discussing a head-to-head comparison of multimodal imaging in the detection of prostate cancer using whole mount histopathology as a reference, with the following take-home points:
- Micro ultrasound demonstrates comparable performance to mpMRI for detecting clinically significant prostate cancer at lesion-level and patient-level extraprostatic extension
- mpMRI is more accurate in the sector-level analysis
- Micro ultrasound can complement mpMRI, particularly where mpMRI access is limited
- Micro ultrasound’s comparable lesion-level accuracy supports its use in targeted biopsy to improve diagnosis
Presented by: Wayne G. Brisbane, MD, David Geffen School of Medicine, University of California, Los Angeles, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Western Section American Urological Association (AUA) Annual Meeting, Napa Valley, CA, Sun, Nov 2 – Thurs, Nov 6, 2025.
WSAUA 2025: Impact of Bone Protecting Agents on Outcomes with Enzalutamide, with or without Radium-223, in Asymptomatic/mildly Symptomatic Patients with Bone mCRPC from PEACE-3
- Details
(Urotoday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Murilo de Almeida Luz, MD, discussing the impact of bone-protecting agents on outcomes with enzalutamide, with or without radium-223, in asymptomatic/mildly symptomatic patients with bone mCRPC from PEACE-3. PEACE-3 was an ethics-approved international study in 446 patients with mCRPC and bone metastases randomized 1:1 to a combination of enzalutamide + radium-223 versus enzalutamide alone:1

The trial demonstrated significant improvement in the radiological progression-free survival: HR 0.69 (95% CI 0.54–0.87; p = 0.0009). As of March 2018, an urgent safety letter made co-administration of zoledronic acid or denosumab obligatory. This analysis, presented at the 2025 Western Section AUA annual meeting, aimed to determine whether the use of a bone-protecting agent enhanced the therapeutic efficacy of treatment in patients who were treated with or without bone-protecting agents prior to the urgent safety letter.
This analysis included 115 patients who enrolled prior to the urgent safety letter and received protocol treatment. Of these, 59 (51%) received either no bone-protecting agents or only after a fracture had occurred, while 56 (49%) received bone-protecting agents prior and/or during study treatment. Efficacy outcomes included radiological progression-free survival, overall survival, and time to subsequent therapy.
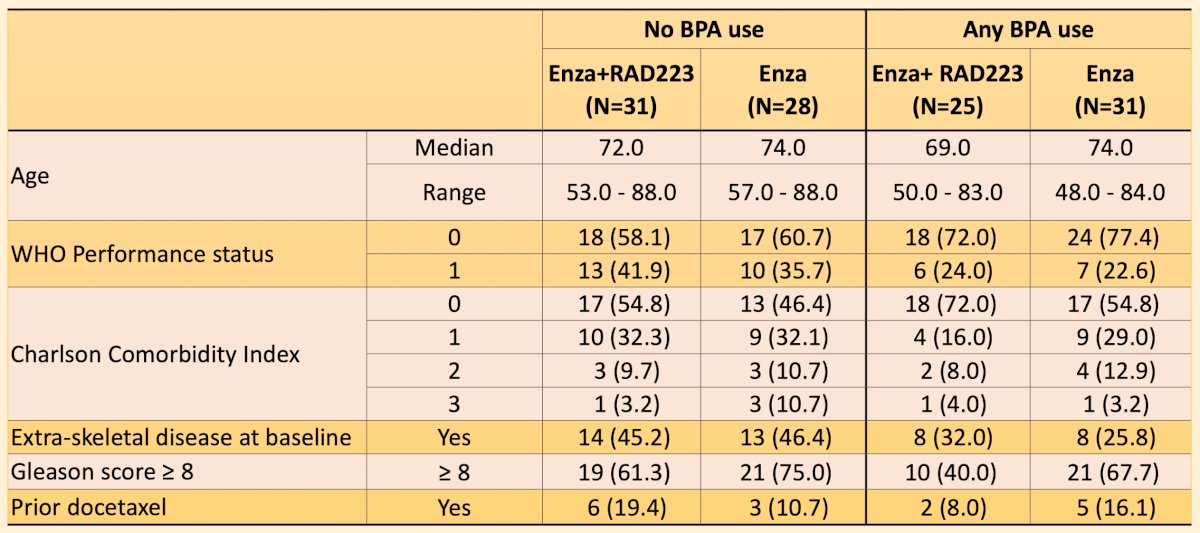
Patients with bone-protecting agent use versus no bone-protecting agent had similar baseline characteristics:
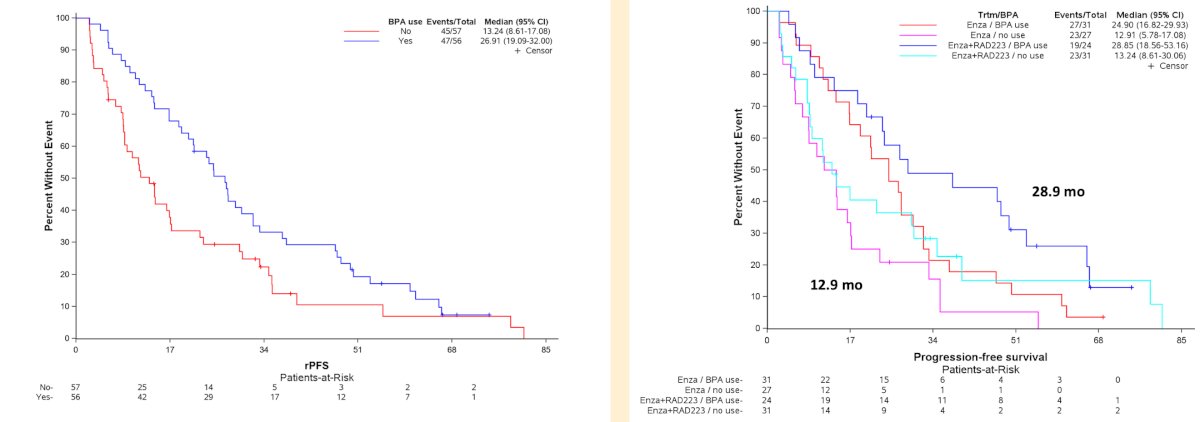
The median enzalutamide treatment duration was 12 months (IQR: 7–27) without and 26 months (IQR: 13–44) with bone-protecting agent use. The median radiological progression-free survival was longer by 14 months from 13 months without to 27 months with bone-protecting agent use (HR 0.61, 95% CI 0.39–0.95), and this difference was similar across both arms. Patients in the enzalutamide + radium-223 arm with bone-protecting agents had a median radiological progression-free survival of 28.8 months versus only 12.9 months for those in the enzalutamide arm without bone-protecting agents:
Median overall survival was longer by 13 months from 28 months without to 41 months with bone-protecting agent use (HR 0.61, 95% CI 0.40–0.94). Again, this difference was notable between the enzalutamide + radium-223 arm with bone-protecting agents and the enzalutamide arm without bone-protecting agents, with median overall survival of 60 months versus 23.98 months, respectively. Patients without bone-protecting agents reported more severe (CTCAE grade ≥3) anemia (9% versus 2%) and renal/urinary disorders (9% versus 2%), but less severe hypertension (39% versus 52%).
Dr. de Almeida Luz concluded his presentation discussing the impact of bone-protecting agents on outcomes from PEACE-3 with the following take-home points:
- In the overall population, radiographic progression-free survival was significantly improved with the addition of radium-223 to enzalutamide
- Bone-protecting agent use led to an improvement in radiographic progression-free survival, with a similar advantage in both arms
- Bone-protecting agent use also led to an improvement in overall survival, again with a similar advantage in both arms
- These exploratory findings suggest that bone-protecting agents in combination with life-prolonging therapeutic options in mCRPC are safe and may provide additional therapeutic benefit
Presented by: Murilo de Almeida Luz, MD, Hospital Erasto Gaertner, Curitiba, Brazil
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Western Section American Urological Association (AUA) Annual Meeting, Napa Valley, CA, Sat, Nov 2 – Thurs, Nov 6, 2025.
References:
WSAUA 2025: Genomic Classifier Scores and Risk of Histologic Upgrading on Confirmatory Biopsy During Active Surveillance
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Dr. James Nie discussing genomic classifier scores and risk of histologic upgrading on confirmatory biopsy during active surveillance.
WSAUA 2025: Baseline Characteristics From the uTRACT Registry Evaluating the Real-World use of UGN-101 in Participants with UTUC in the United States
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a urothelial carcinoma session and a presentation by Dr. Jennifer Linehan discussing baseline characteristics from the uTRACT registry evaluating the real-world use of UGN-101 in participants with upper tract urothelial carcinoma in the United States. Upper tract urothelial carcinoma affects 1-2 in 100,000 people in the United States annually.
WSAUA 2025: Efficacy and Safety of Darolutamide + ADT in Black Patients with Metastatic Hormone-Sensitive Prostate Cancer from the Phase 3 ARANOTE Trial
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Dr. Quoc-Dien Trinh discussing the efficacy and safety of darolutamide + ADT in Black patients with metastatic hormone-sensitive prostate cancer (mHSPC) from the phase 3 ARANOTE trial. Incidence and mortality rates of prostate cancer are higher in Black patients versus other racial groups, yet studies suggest Black patients with metastatic castration-resistant prostate cancer (mCRPC) may respond better to therapy.
WSAUA 2025: Integrating Genomic Prognostic and Hallmark Signatures from Decipher GRID to Predict Adverse Outcomes in Men on Active Surveillance for Prostate Cancer
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Dr. Kevin Shee discussing the integration of genomic prognostic and hallmark signatures from Decipher GRID to predict adverse outcomes in men on active surveillance for prostate cancer. Active surveillance has been accepted as the standard management for lower-risk prostate cancer by major clinical guidelines.
WSAUA 2025: PSA Response with Darolutamide + ADT in Patients with Metastatic Hormone-Sensitive Prostate Cancer in ARANOTE
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Dr. David Crawford discussing PSA response with darolutamide + ADT in patients with metastatic hormone-sensitive prostate cancer in ARANOTE.1
WSAUA 2025: Erdafitinib Use in Eligible Patients with Metastatic Urothelial Carcinoma: Results from the Veterans Health Administration
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a urothelial carcinoma session and a presentation by Dr. Meera Chappidi discussing erdafitinib use in eligible patients with metastatic urothelial carcinoma in the Veterans Health Administration. Next-generation sequencing of tumors from patients with metastatic urothelial carcinoma can identify genomic alterations that may help guide treatment selection.
WSAUA 2025: Comprehensive Analysis of the Correlation Between Molecular Subtype and Multimodal Imaging Features of Prostate Cancer
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Dr. Wayne Brisbane discussing comprehensive analysis of the correlation between molecular subtype and multimodal imaging features of prostate cancer. Over the last several years, both molecular subtyping and multimodal imaging features have helped with risk-stratifying prostate cancer patients.
WSAUA 2025: Nurse and Advanced Practice Provider Perspectives on TAR-200 Treatment of High Risk NMIBC in the Urology Clinic
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a urothelial carcinoma session and a presentation by Dr. Siamak Daneshmand discussing nurse and advanced practice provider perspectives on TAR-200 treatment of high-risk non-muscle invasive bladder cancer in the urology clinic. Non-muscle invasive bladder cancer accounts for ~70% of all bladder cancer cases, and ~50% of patients with high-risk non-muscle invasive bladder cancer experience disease recurrence or progression on BCG.
WSAUA 2025: Impact of PSA Doubling Time and Absolute PSA on PSMA PET Positivity in Post-Prostatectomy Biochemical Recurrence
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Dr. Mouneeb Choudry discussing the impact of PSA doubling time and absolute PSA on PSMA PET positivity in post-prostatectomy biochemical recurrence.
WSAUA 2025: Matching Adjusted Indirect Comparisons of TAR-200 versus FDA-Approved Novel Agents in BCG Unresponsive High-Risk NMIBC with CIS
- Details
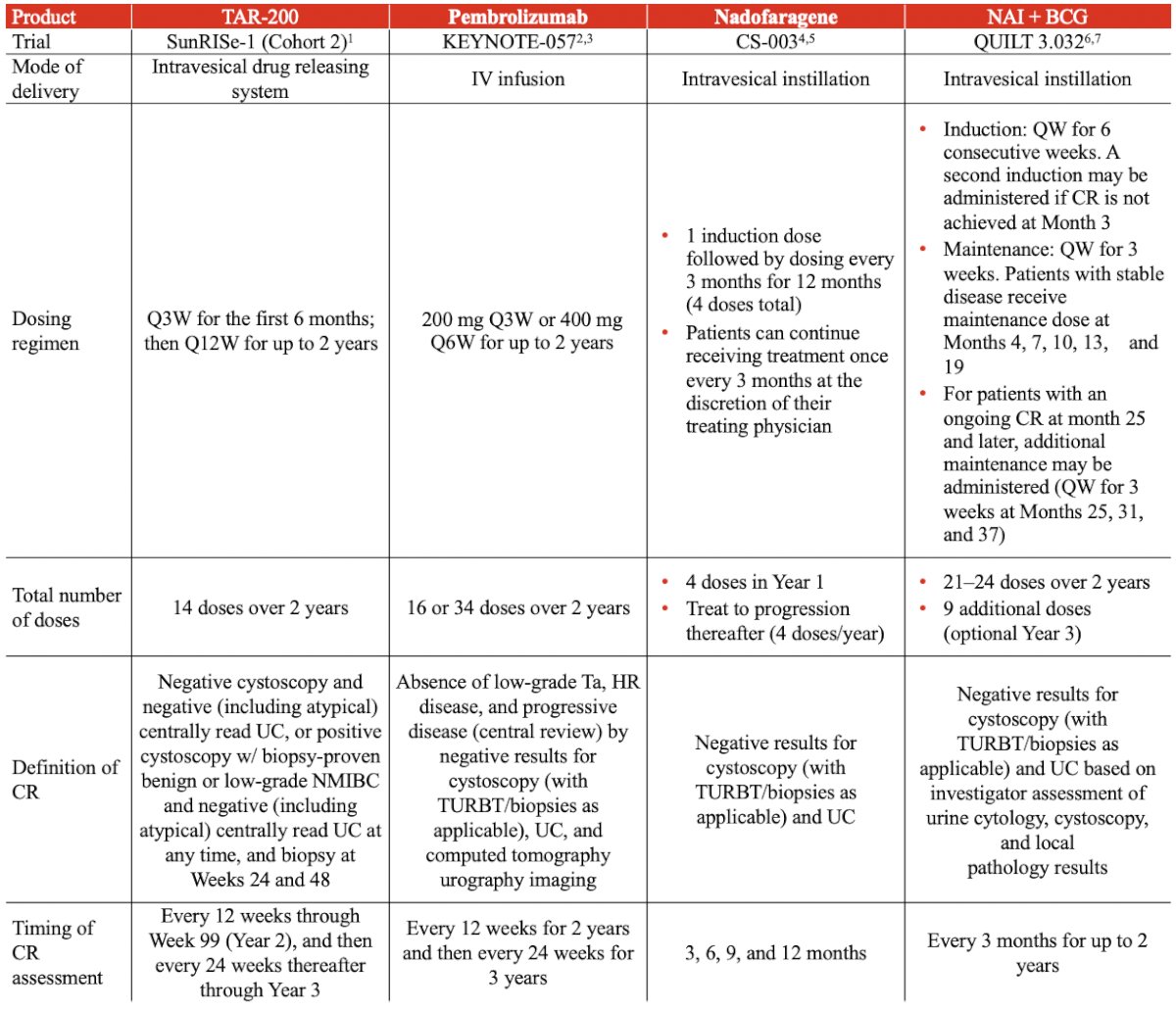
(Urotoday.com) The 2025 Western Section AUA annual meeting featured a urothelial carcinoma session and a presentation by Siamak Daneshmand, MD, discussing a matching adjusted indirect comparison of TAR-200 versus FDA-approved novel agents in BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS. TAR-200 is a novel intravesical drug-releasing system designed for sustained, local delivery of gemcitabine within the bladder. TAR-200 is being investigated in the phase 2b SunRISe-1 study for patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS, with or without papillary tumors, who have refused or are ineligible for radical cystectomy (Cohort 2)1. Moreover, TAR-200 has demonstrated a centrally assessed any time complete response rate of 82.4% in this population. Previously, the FDA has approved pembrolizumab2, nadofaragene firadenovec-vncg (nadofaragene)3, and nogapendekin alfa inbakicept-pmln (NAI) + BCG4 for the treatment of patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS. In the absence of head-to-head data, matching adjusted indirect comparisons were conducted to compare complete response of TAR-200 versus FDA-approved novel agents.
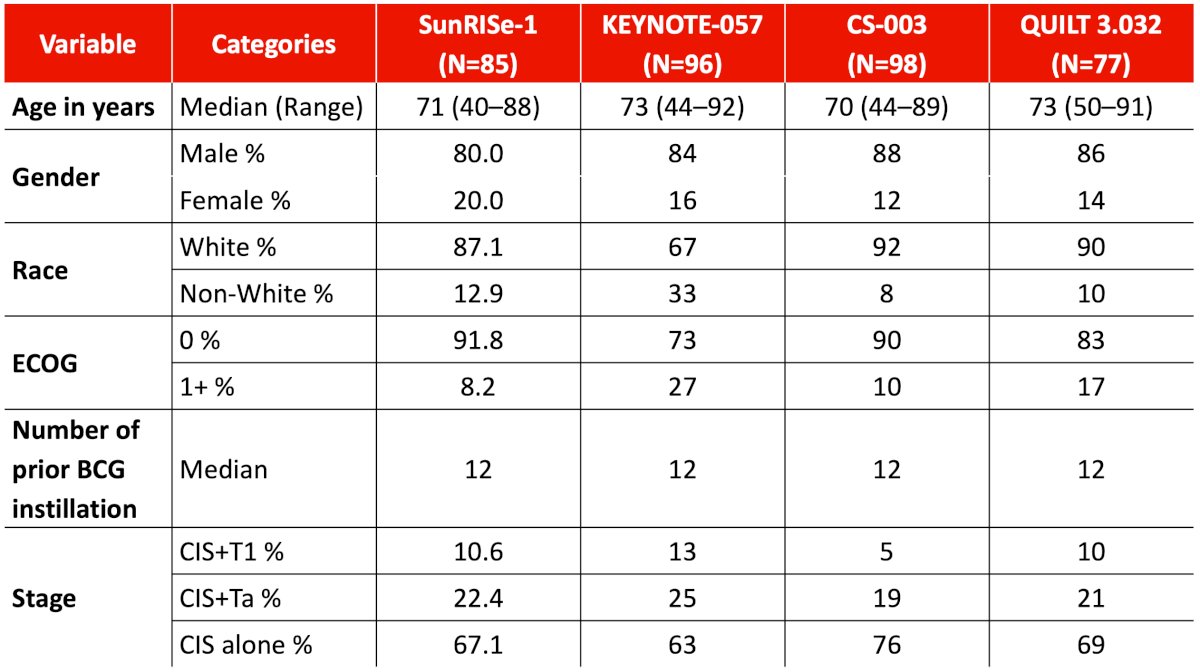
A systematic literature review identified published data on the comparator regimens in the BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS setting. The feasibility of conducting matching-adjusted indirect comparisons was assessed by reviewing the study and patient characteristics, patient eligibility criteria, outcome definitions, and time points of SunRISe-1 and trials of FDA-approved novel agents —KEYNOTE-057, CS-003, and QUILT 3.032 — to determine heterogeneity. Three unanchored matching adjusted indirect comparisons were conducted using individual patient data from SunRISe-1 Cohort 2 and summary-level data from the US prescribing information and primary journal publications of the comparators. Imbalances in patient characteristics (tumor stage, prior doses of BCG instillation, ECOG performance status, age, gender, and race) were adjusted by weighting the TAR-200 individual patient data to match the reported baseline characteristics of the comparator trials. Comparative efficacy was estimated for complete response rate at any time and at first disease assessment. Relative effects were quantified using rate differences with 95% confidence intervals derived from weighted logistic regression analysis.
Dosing regimens, modes of delivery, and definitions of complete response varied across the SunRISe-1, KEYNOTE-057, CS-003, and QUILT 3.032 trials:
Baseline characteristics were similar across all four trials after matching:
After adjustment, the three matching adjusted indirect comparisons showed that TAR-200 provides significantly higher complete response rate at any time versus all three FDA-approved novel agents (p < 0.05 for all comparisons) in the BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS setting. The greatest incremental difference was observed in the TAR-200 versus pembrolizumab comparison (+48%):

Given that re-induction was allowed in QUILT 3.032, an analysis comparing complete response rate at first disease assessment of TAR-200 versus NAI + BCG was conducted to assess the impact of re-induction on complete response rate:
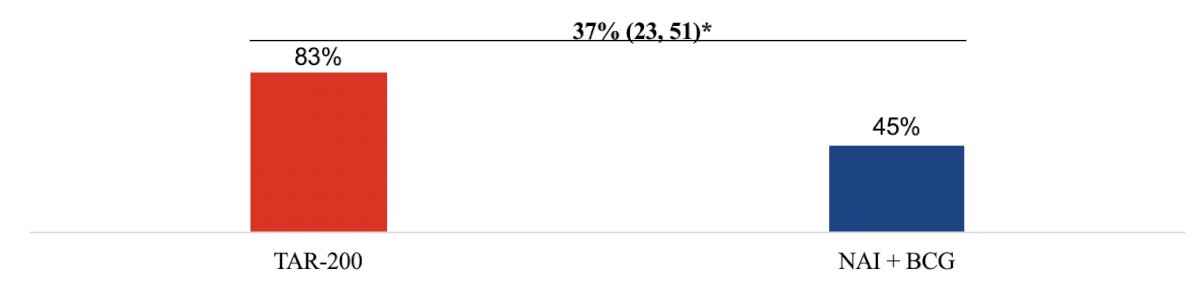
Results from this analysis showed that treatment with TAR-200 led to a significantly higher complete response rate at first disease assessment compared with NAI + BCG (p < 0.05) based on calculated data that excluded patients who received a second induction.
Additional details for the calculation of complete response at first disease assessment for NAI + BCG are as follows:
- In the US prescribing information, the efficacy results from QUILT 3.032 (n = 77) state that 62% achieved complete response at any time (n = 48 responders). The US prescribing information also states that 31% (n = 24) of patients received a second induction course
- Chamie et al.4 also state that 24 patients received re-induction in Cohort A
- Thus, the investigators deduced that the 24 re-induced patients are the same across both data sets. Chamie et al.4 state that of the 24 re-induced patients, 13 achieved complete response after re-induction
- Triangulating between the sources, Dr. Daneshmand and colleagues calculated from the US prescribing information that 48 total responders – 13 responders after re-induction/77 total patients = 45% of patients achieving complete response at first disease assessment
Limitations of this analysis include the matching adjusted indirect comparison methodology only adjusting for observed and reported baseline characteristics. Additionally, any confounders not consistently reported or missing across studies may impact internal validity. Finally, some differences in study design and outcomes can introduce biases that the matching-adjusted indirect comparison cannot fully address.
Dr. Daneshmand concluded his presentation discussing a matching-adjusted indirect comparison of TAR-200 versus FDA-approved novel agents in BCG-unresponsive high-risk non-muscle invasive bladder cancer with CIS, and included the following take-home points:
- TAR-200 is a novel intravesical drug release system that offers a convenient fixed duration treatment regimen with a low number of doses for patients with BCG unresponsive high-risk non-muscle invasive bladder cancer with CIS, without the need for re-induction
- Given that no head-to-head trials exist in this setting, the matching adjusted indirect comparison provides scientific information for clinical and reimbursement decision-making making
- TAR-200 provides a statistically significant clinical benefit in complete response rate at any time versus pembrolizumab, nadofaragene, and NAI + BCG
- TAR-200 also provides a significantly higher complete response rate at first disease assessment compared with NAI + BCG
Presented by: Siamak Daneshmand, University of Southern California, Norris Comprehensive Cancer Center, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Western Section American Urological Association (AUA) Annual Meeting, Napa Valley, CA, Sun, Nov 2 – Thurs, Nov 6, 2025.
References:
- Daneshmand S, Van der Heijden MS, Jacob JM, et al. TAR-200 for Bacillus Calmette-Guerin-Unresponsive High-Risk Non-Muscle-Invasive Bladder Cancer: Results from the Phase IIb SunRISe-1 Study. J Clin Oncol. 2025 Jul 30 [Epub ahead of print].
- Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): An open-label, single-arm, multicenter, phase 2 study. Lancet Oncol. 2021 Jul;22(7):919-930.
- Boorjian SA, Alemozaffar M, Konety BR, et al. Intravesical nadofaragene firadenovec gene therapy for BCG-unresponsive non-muscle-invasive bladder cancer: A single-arm, open-label, repeat-dose clinical trial. Lancet Oncol. 2021 Jan;22(1):107-117.
- Chamie K, Chang SS, Kramolowsky E, et al. IL-15 Superagonist NAI in BCG-Unresponsive Non-Muscle-Invasive Bladder Cancer. NEJM Evid 2022; 2(1).
WSAUA 2025: Ultra-Low PSA Response in ARANOTE Correlates with Improved Clinical Outcomes
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Dr. Jack Andrews discussing the impact of ultra-low PSA response (<0.02 ng/ml) with darolutamide + ADT in ARANOTE. In ARANOTE, darolutamide + androgen deprivation therapy (ADT) significantly reduced the risk of radiological progression or death by 46% versus placebo + ADT in patients with metastatic hormone-sensitive prostate cancer (mHSPC).1
WSAUA 2025: Impact of Post-Traumatic Stress Disorder on Prostate Cancer Outcomes Following Radical Prostatectomy in a Veteran Population
- Details
(Urotoday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Amana Liddell, BS, discussing the impact of post-traumatic stress disorder on prostate cancer outcomes following radical prostatectomy in a veteran population. Prostate cancer and post-traumatic stress disorder are both highly prevalent within the veteran population. Given that stress is known to exacerbate numerous diseases, the investigators sought to determine if post-traumatic stress disorder increases the risk of adverse prostate cancer outcomes and all-cause mortality among veterans who have undergone radical prostatectomy.
This study utilized the VA SEARCH database to identify 7,133 males who underwent radical prostatectomy within the VA health system after 2000. Overall, 30% (n = 2,175) of this population was diagnosed with post-traumatic stress disorder within 3 years prior to radical prostatectomy based on ICD-9 and 10 codes. Cox proportional hazard models were used to test the association between post-traumatic stress disorder and time to biochemical recurrence, metastatic disease, castration-resistant prostate cancer, prostate cancer-specific death, and all-cause mortality.
The patient demographics of those included in the study are as follows:
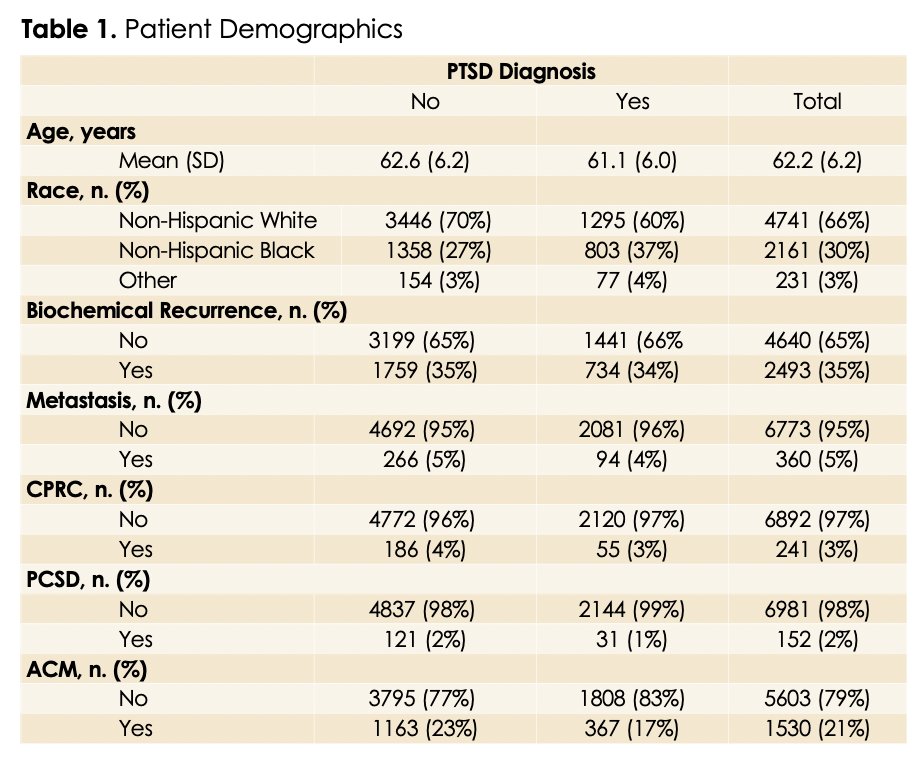
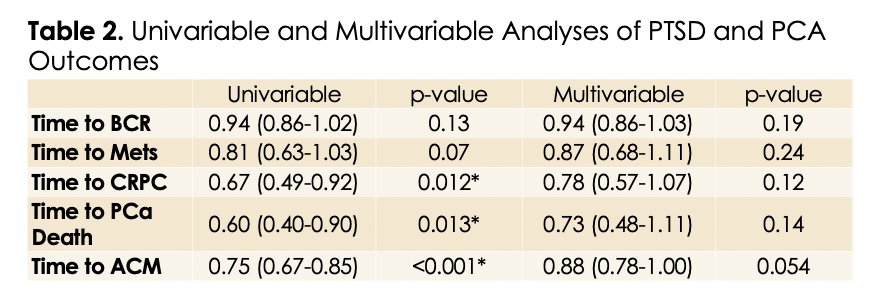
In the univariable analyses, veterans with post-traumatic stress disorder had a 33% reduction in risk of castration-resistant prostate cancer, 40% reduction in risk of prostate cancer-specific death, and 25% reduction in risk of all-cause mortality compared to those without post-traumatic stress disorder. Post-traumatic stress disorder diagnosis did not impact time to biochemical recurrence or time to metastatic disease in the univariable analyses. Multivariable analyses adjusted for demographic and pathological characteristics demonstrated no significant association between post-traumatic stress disorder and prostate cancer-specific progression endpoints. There was, however, a trend for a positive association with post-traumatic stress disorder and improved overall survival (HR 0.88, 95% CI 0.78–1.00, p = 0.054). The following table summarizes the univariable and multivariable analyses of post-traumatic stress disorder and prostate cancer outcomes:
Possible explanations for these findings include differences in healthcare utilization and behavioral factors. More specifically, veterans with post-traumatic stress disorder may engage more frequently with the healthcare system, resulting in earlier detection and treatment of prostate cancer and thus improved outcomes.
Amana Liddell concluded this presentation discussing the impact of post-traumatic stress disorder on prostate cancer outcomes following radical prostatectomy in a Veteran population with the following take-home points:
- Post-traumatic stress disorder did not increase the risk of adverse prostate cancer outcomes such as biochemical recurrence, metastasis, CRPC, and prostate cancer death in veterans who underwent radical prostatectomy
- These findings showed a trend that suggests post-traumatic stress disorder was associated with improved overall survival, which challenges existing literature that links stress with adverse health outcomes
- Future research is needed to further investigate the mechanisms that contribute to improved overall survival in veterans with post-traumatic stress disorder who underwent radical prostatectomy
Presented by: Amana Liddell, BS, Greater Los Angeles Veterans Affairs, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Western Section American Urological Association (AUA) Annual Meeting, Napa Valley, CA, Sun, Nov 2 – Thurs, Nov 6, 2025.
WSAUA 2025: Darolutamide + ADT Therapy in Patients with Metastatic Hormone-Sensitive Prostate Cancer: Efficacy and Safety by Disease Volume in the Phase 3 ARANOTE Study
- Details
(UroToday.com) The 2025 Western Section AUA annual meeting featured a prostate cancer session and a presentation by Dr. David Crawford discussing efficacy and safety by disease volume in ARANOTE. In the phase 3 ARANOTE study, patients with metastatic hormone-sensitive prostate cancer (mHSPC) receiving darolutamide + ADT experienced a 46% reduction in radiological progression or death when compared with those receiving placebo + ADT (HR 0.54; 95% CI 0.41–0.71; p<0.0001).1