(UroToday.com) The 2025 Western Section AUA annual meeting featured a kidney cancer session and a presentation by Jaxson Jeffery discussing the impact of neoadjuvant systemic therapy on tumor and tumor thrombus regression in renal cell carcinoma (RCC) with venous involvement. The utility of neoadjuvant systemic therapy in RCC with inferior vena cava (IVC) tumor thrombus is inadequately defined.
While tyrosine kinase inhibitors and immune checkpoint inhibitors show efficacy in advanced RCC, their role in facilitating surgical resection via preoperative downstaging is not well established. This study, presented at the 2025 Western Section AUA annual meeting, investigated radiographic and perioperative outcomes in RCC patients with IVC tumor thrombus who received neoadjuvant systemic therapy prior to nephrectomy and IVC thrombectomy.
Data were investigated from the Mayo Clinic Advanced Renal Cancer Database, a multi-institutional resource. The investigators retrospectively identified clear cell RCC patients with venous tumor thrombus who received neoadjuvant systemic therapy followed by radical or cytoreductive nephrectomy (2010-2024). Regimens included tyrosine kinase inhibitor monotherapy, immune checkpoint inhibitor + tyrosine kinase inhibitor combination, or dual immune checkpoint inhibitors. Metrics evaluated included primary tumor size and thrombus level changes, and perioperative outcomes. RECIST 1.1 criteria assessed radiographic changes, and survival was estimated using Kaplan-Meier methods.
Overall, there were 39 patients included in the analysis. The median age was 66 years (IQR: 61–73), and 76.9% were male. The median neoadjuvant systemic therapy duration was 9.2 months for immune checkpoint inhibitor + tyrosine kinase inhibitor therapy, 6.7 months for tyrosine kinase inhibitor monotherapy, and 4.5 months for immune checkpoint inhibitor + immune checkpoint inhibitor combination therapy. The mean tumor size decreased from 9.8 cm to 7.1 cm, with the greatest reduction in the immune checkpoint inhibitor + tyrosine kinase inhibitor group (−3.0 cm). IVC thrombus level reduction occurred in 16 patients (41.0%):
- 44.0% in immune checkpoint inhibitor + tyrosine kinase inhibitor combination therapy
- 40.0% in immune checkpoint inhibitor + immune checkpoint inhibitor combination therapy
- 33.3% in tyrosine kinase inhibitor monotherapy
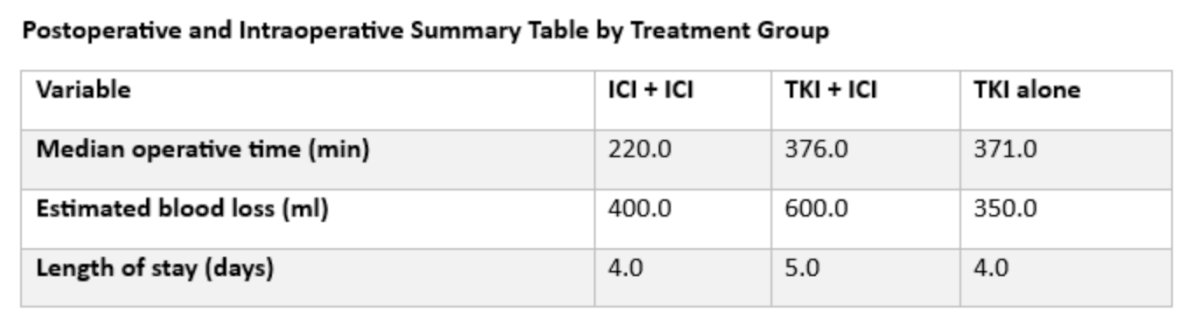
All patients receiving dual immune checkpoint inhibitors had localized disease, whereas metastatic disease was present in 72.0% of the immune checkpoint inhibitor + tyrosine kinase inhibitor and 33.3% of the tyrosine kinase inhibitor groups. Postoperative complications occurred in 11 patients (28.2%), most commonly Clavien-Dindo grade II (n = 5). Operative time and estimated blood loss were highest in the immune checkpoint inhibitor + tyrosine kinase inhibitor group:
The median overall survival was longest in the tyrosine kinase inhibitor group (1,961 days), followed by immune checkpoint inhibitor + immune checkpoint inhibitor combination (716 days), and immune checkpoint inhibitor + tyrosine kinase inhibitor combination (270 days), although interpretation is limited by the small sample size and follow-up duration:

Jaxson Jeffery concluded his presentation discussing the impact of neoadjuvant systemic therapy on tumor and tumor thrombus regression in RCC with venous involvement with the following take-home points:
- Neoadjuvant systemic therapy was associated with measurable reductions in primary tumor size and thrombus level in RCC patients with venous involvement, particularly among those receiving immune checkpoint inhibitor + tyrosine kinase inhibitor combination therapy
- These findings support preoperative tumor downstaging feasibility and underscore the need for prospective studies to refine patient selection and optimize treatment strategies
Presented by: Jaxson Jeffery, Medical Student, Mayo Clinic, Phoenix, AZ
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Western Section American Urological Association (AUA) Annual Meeting, Napa Valley, CA, Sun, Nov 2 – Thurs, Nov 6, 2025.