(UroToday.com) The 2026 Southeastern Section of the AUA Annual Meeting featured a presentation by Dr. Zachary Klaassen of a post hoc analysis from the phase 3 ARANOTE trial evaluating darolutamide plus androgen-deprivation therapy (ADT) versus placebo plus ADT in patients with metastatic hormone-sensitive prostate cancer (mHSPC), with outcomes stratified by disease volume.
This analysis specifically examined whether the efficacy and safety of darolutamide are consistent across high- and low-volume disease, as defined by CHAARTED criteria.
ARANOTE is a global, randomized, double-blind phase 3 trial enrolling patients with mHSPC diagnosed by conventional imaging, ECOG performance status 0–2, and initiation of ADT within 12 weeks prior to randomization. A total of 669 patients were randomized in a 2:1 fashion to darolutamide 600 mg twice daily plus ADT (n=446) or placebo plus ADT (n=223). The primary endpoint was radiographic progression-free survival (rPFS) by blinded independent central review, with key secondary endpoints including overall survival, time to metastatic castration-resistant prostate cancer (mCRPC), time to PSA progression, time to subsequent systemic therapy, undetectable PSA (<0.2 ng/mL), time to pain progression, and safety.
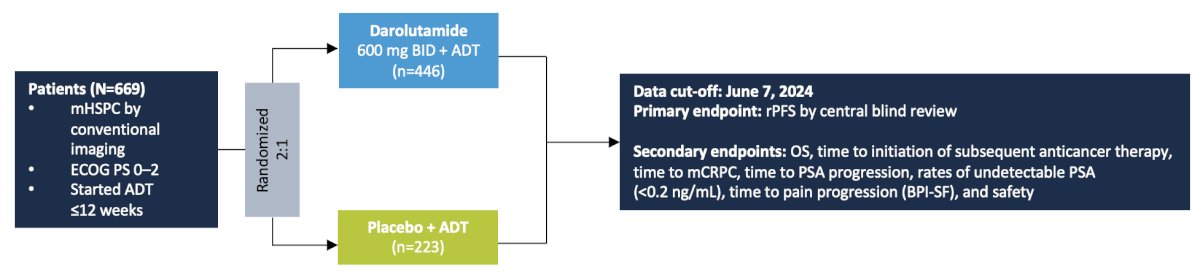
Patients were stratified by disease volume, with high-volume defined as visceral metastases and/or ≥4 bone metastases with ≥1 beyond the vertebral bodies and pelvis, and low-volume defined as all others.
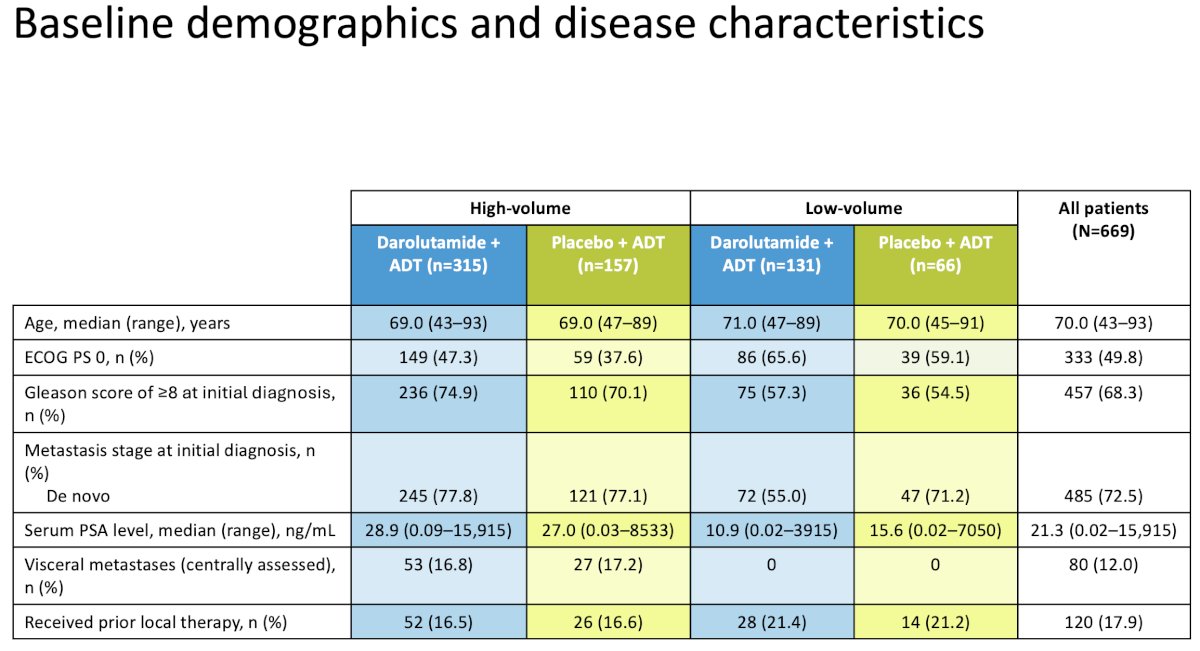
Baseline characteristics were balanced across treatment arms within each subgroup. In the high-volume cohort, median age was 69 years, approximately 75% of patients had Gleason score ≥8 disease, ~78% had de novo metastatic disease, median PSA was ~28–29 ng/mL, and ~17% had visceral metastases. In the low-volume cohort, median age was 70–71 years, Gleason ≥8 disease was observed in ~55–57%, de novo disease in 55–71%, and median PSA ranged from 10.9 to 15.6 ng/mL.
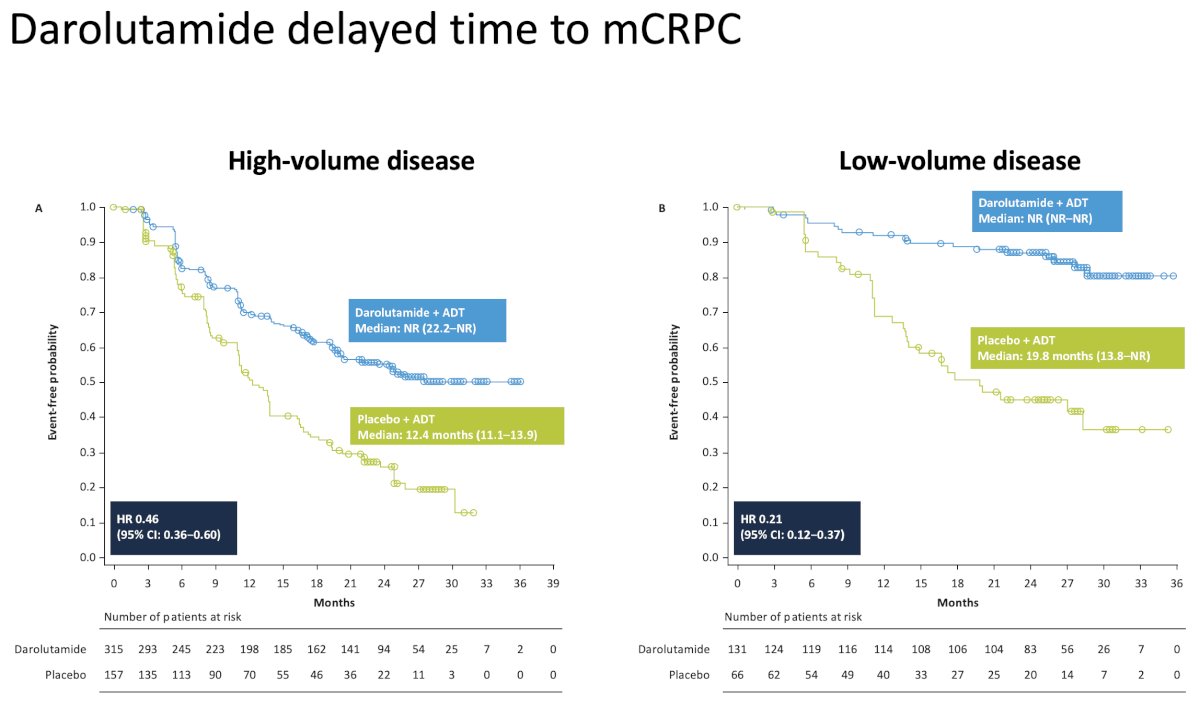
Efficacy analyses demonstrated consistent benefit with darolutamide across both disease volume subgroups. Kaplan–Meier curves for time to mCRPC showed early and sustained separation favoring darolutamide in high-volume disease (HR: 0.46, 95% CI: 0.36-0.60), with an even more pronounced and durable separation in low-volume disease (HR: 0.21, 95% CI: 0.12-0.37), suggesting a greater relative treatment effect in this subgroup.
This pattern was consistent across key secondary endpoints. Darolutamide significantly delayed time to subsequent systemic therapy (overall HR 0.40), with subgroup hazard ratios of 0.47 in high-volume and 0.19 in low-volume disease. Similarly, time to PSA progression was significantly prolonged (overall HR 0.31), with hazard ratios of 0.34 and 0.19 in high- and low-volume disease, respectively. Median time to PSA progression in the placebo arm was 13.9 months in high-volume and 28.3 months in low-volume disease, while not reached in the darolutamide arm. Time to pain progression also favored darolutamide (overall HR 0.72), with numerically greater benefit in low-volume disease (HR 0.53) compared to high-volume disease (HR 0.78).

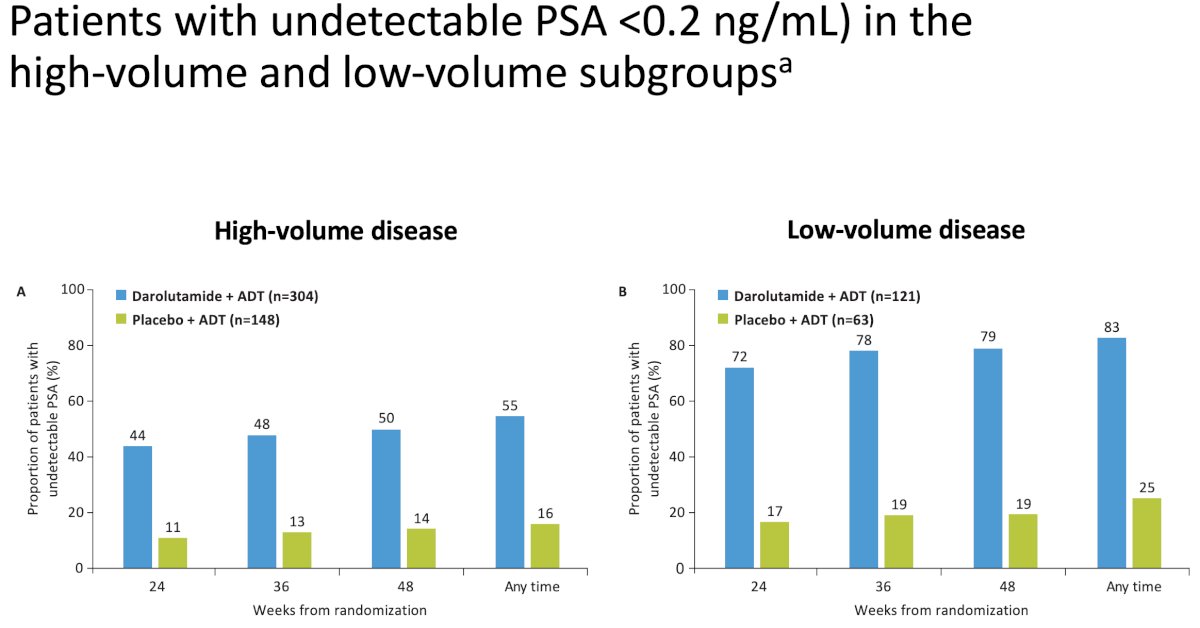
PSA response data further supported these findings. The proportion of patients achieving undetectable PSA (<0.2 ng/mL) was substantially higher with darolutamide across both subgroups. In high-volume disease, undetectable PSA rates were approximately 36% versus 11% at week 24, 50% versus 13% at week 48, and ~55% versus 16% at any time for darolutamide versus placebo. In low-volume disease, corresponding rates were approximately 72% versus 17% at week 24, 79% versus 19% at week 48, and ~83% versus 25% at any time. These data highlight deeper and more durable PSA responses, particularly among patients with low-volume disease.
Safety profiles were comparable between treatment arms regardless of disease volume, with no meaningful increase in adverse events observed with darolutamide. Notably, fewer patients discontinued treatment due to adverse events in the darolutamide arm, supporting its favorable tolerability.
In conclusion, darolutamide plus ADT provides consistent and clinically meaningful benefit in patients with mHSPC regardless of disease volume. Treatment significantly delays progression to mCRPC, prolongs time to PSA progression, reduces the need for subsequent systemic therapy, and increases rates of deep PSA responses, all while maintaining a favorable safety profile. The magnitude of benefit appears particularly pronounced in patients with low-volume disease, supporting treatment intensification across all mHSPC subgroups.
Presented by: Zachary Klaassen, MD, MSc, Urologic Oncologist, Assistant Professor of Surgery/Urology at the Medical College of Georgia at Augusta University, Well Star MCG, Georgia Cancer Center, Augusta, GA
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the AUA SES Annual Meeting in Rio Grande, PR
Related Content:
EAU 2026: Who Benefits from Intensification with Docetaxel?
EAU 2026: Disconnect Between Evidence and Real-World Data in Metastatic Prostate Cancer
ASCO GU 2026: Impact of Hospitalizations on Health-Related Quality of Life and Overall Survival in mCSPC: Insights from the ARANOTE Trial