(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., between March 13th and 16th 2026, was host to the Hormone-sensitive metastatic prostate cancer: Thematic Session. Dr. Christopher Sweeney argued there is a disconnect between evidence and real-world data in metastatic prostate cancer.
Dr. Sweeney began by presenting two clinical cases to highlight the broad range of reasons why patients may not be eligible for clinical trials and the resulting disconnect between trial evidence and real-world practice. The first patient, described as non-compliant, had unstable social circumstances and unreliable treatment adherence, making him unsuitable for intensification strategies such as those used in ARASENS.1 The second patient, an 88-year-old frail individual with multiple comorbidities, was also not eligible for clinical trials, and even the selection of an ARPI was challenging. These cases illustrate how many real-world patients fall outside the populations typically represented in clinical trials and, therefore, outside the populations that inform current guidelines.
Dr. Sweeney then reviewed the evolving long-term outcomes in mHSPC, highlighting how survival has progressively improved across successive trials. In earlier SWOG studies, when ADT alone was the main treatment approach, approximately 25% of patients were alive at 8 years. With treatment intensification in trials such as CHAARTED, survival improved to roughly 35% at 8 years, and more recent data from ENZAMET show nearly 50% of patients alive at 8 years.2,3 Notably, about 30% of patients remained on enzalutamide long term, and approximately 15% of deaths were due to non–prostate cancer causes, reflecting the increasingly prolonged survival in this population.

Moreover, he discussed a retrospective real-world study of patients with de novo mHSPC showing that the addition of an ARPI to ADT was associated with improved survival, with approximately 50% of patients alive at 4 years with ADT + ARPI. He contrasted these findings with results from the ENZAMET trial, where in patients with de novo mHSPC not treated with docetaxel, roughly 50% of high-volume patients were alive at 5.5 years, and about 50% of low-volume patients were alive beyond 8 years with ADT + ARPI. Overall, the treatment effect appeared similar between real-world and clinical trial populations, although survival tended to be shorter in the real-world setting.

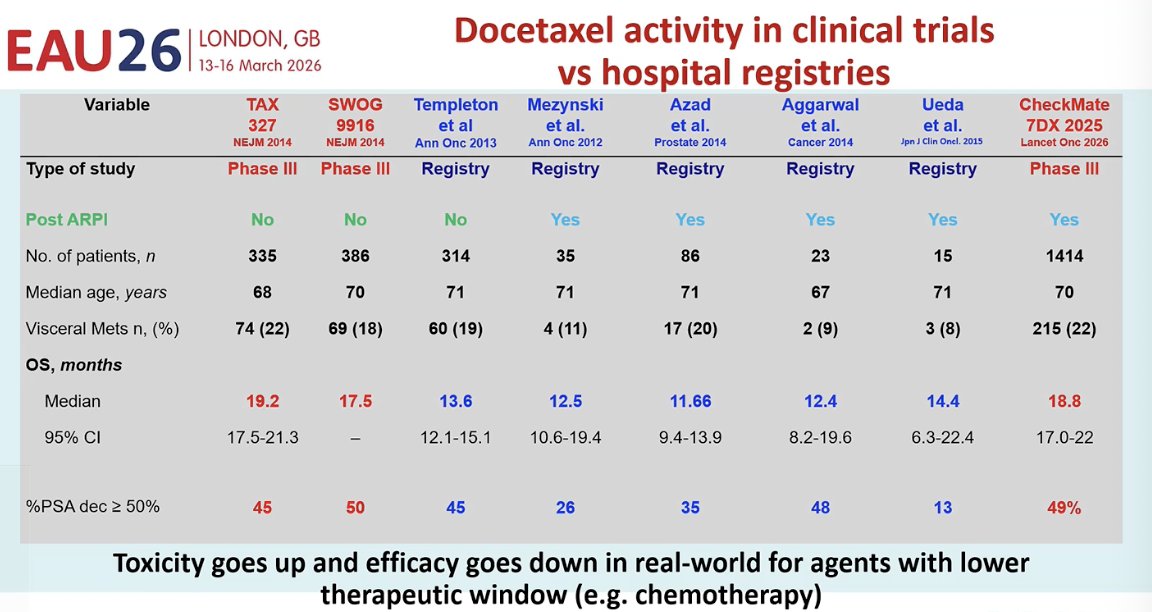
Dr. Sweeney also highlighted that the activity of docetaxel observed in clinical trials does not always translate the same way in real-world practice. Data from hospital registries suggest that outcomes are generally worse outside of the controlled trial setting, with shorter overall survival and lower response rates compared with phase III trials. This likely reflects broader patient populations, greater comorbidity, and treatment-related toxicity, emphasizing that agents with narrower therapeutic windows, such as chemotherapy, often perform less favorably in real-world settings.
Dr. Sweeney also noted that treating physicians often receive mixed messages from clinical trials and conference discussions. One consistent finding across multiple studies is the benefit of adding an ARPI to ADT, which has been reproducibly demonstrated in trials such as STAMPEDE, LATITUDE, TITAN, ARCHES, ENZAMET, and ARANOTE.1-4 In contrast, the role of additional intensification strategies remains less clear. Trials evaluating the addition of docetaxel or radiation to ADT, or the use of triplet therapy with ADT, ARPI, and docetaxel or radiation, have produced more variable results, leading to uncertainty about which patients should receive these combinations and whether they should be applied broadly or only in selected subgroups.
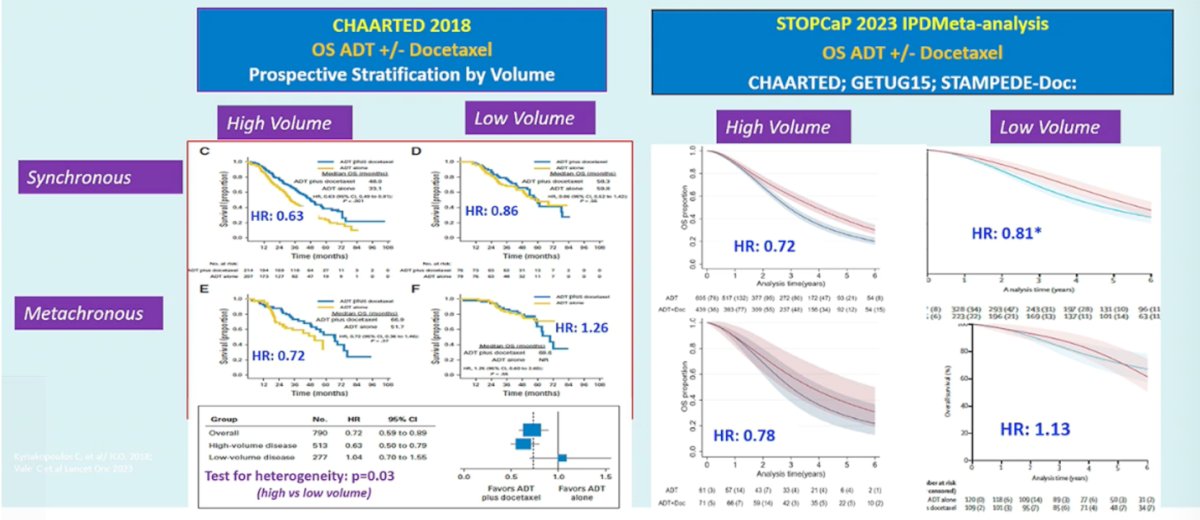
Dr. Sweeney then proposed a model for consensus building based on global data sharing across trials. Using pooled analyses from studies such as CHAARTED,2 investigators were able to better define which patients benefit from adding docetaxel to ADT (As shown below). These analyses showed that the benefit of docetaxel is most pronounced in patients with high-volume disease, particularly those with synchronous metastatic presentation, while the benefit appears much more limited in patients with low-volume disease. This approach illustrates how collaborative data analysis can help clarify conflicting trial results and guide more precise treatment decisions.
A similar effort was conducted through the STOPCAP individual patient data meta-analysis, which pooled results from CHAARTED, GETUG-15, and STAMPEDE. This analysis confirmed that the survival benefit of adding docetaxel to ADT is primarily seen in patients with high-volume disease, with more modest or uncertain benefit in low-volume disease.5
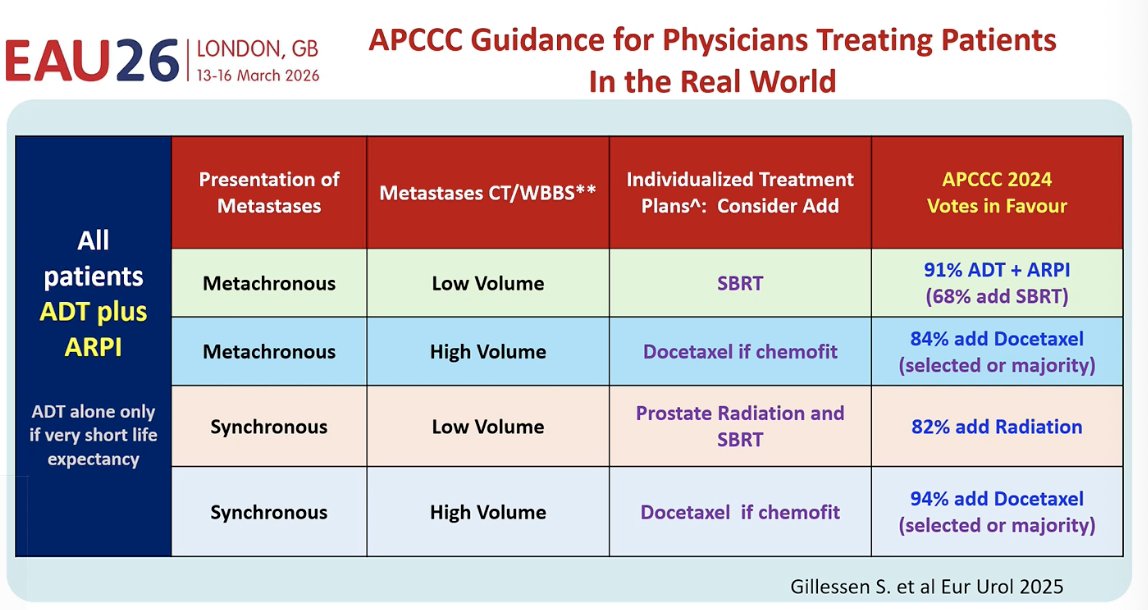
These data were subsequently brought to the APCCC 2024 consensus conference, where experts voted on treatment strategies to help reduce confusion for treating physicians. A clear message emerged that ADT plus an ARPI should be the backbone of therapy for most patients. Additional treatment decisions were then tailored based on disease presentation and volume. For example, SBRT was favored in patients with metachronous low-volume disease, radiation to the prostate was supported in synchronous low-volume disease, and docetaxel was recommended for patients with high-volume disease who are fit for chemotherapy. This collaborative effort across multiple trials helped move the field toward a clearer consensus and more consistent treatment recommendations.
Dr. Sweeney then raised a practical question: What proportion of patients should, and realistically can, receive ADT + ARPI + additional intensification? He emphasized that ADT + ARPI should now be considered the default backbone of therapy. With the availability of darolutamide, more patients may be eligible for intensification, although important limitations remain, including avoidance of abiraterone in older patients and contraindications to enzalutamide or apalutamide, such as seizure risk. He also noted that some clinicians still favor SBRT alone for selected patients with metachronous oligometastatic disease.
Beyond biology, real-world factors strongly influence treatment delivery, including access to and affordability of ARPIs, the proportion of patients who are truly appropriate for docetaxel, and access to radiation. These issues vary substantially between community or regional settings, where patients are often older, frailer, and live farther from treatment centers, and high-volume urban academic centers. He added that regional differences in rates of de novo high-volume disease may also reflect differences in PSA testing and screening practices.
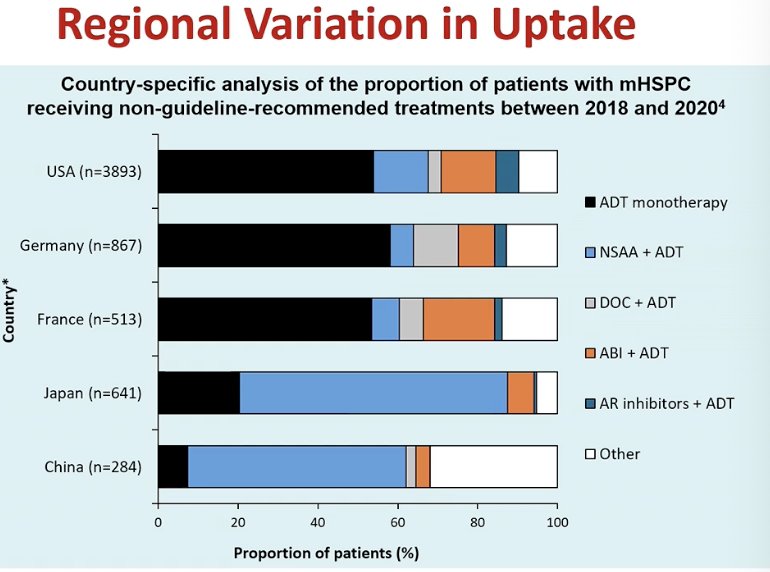
He further emphasized that despite strong evidence supporting treatment intensification, there remains substantial undertreatment worldwide. The first clear OS benefit for ADT + ARPI in mHSPC emerged in 2017, and the 2024 EAU guidelines now recommend offering ADT + ARPI to patients who are fit for the regimen. However, real-world data reveal large regional differences in uptake, with many patients still receiving ADT alone or other non–guideline-recommended treatments. In some datasets, up to 76% of patients were treated outside guideline recommendations, highlighting a significant gap between evidence and clinical practice. He highlighted the regional variation in uptake of clinical guidelines recommendations, as shown below.
Moreover, he highlighted that financial barriers play a major role in treatment uptake. Real-world data from Australia, where therapies are government funded, show that approximately 73% of patients receive guideline-recommended treatment, most commonly ADT + ARPI with or without docetaxel. This suggests that when patient out-of-pocket costs are minimized, adherence to evidence-based treatment strategies improves substantially
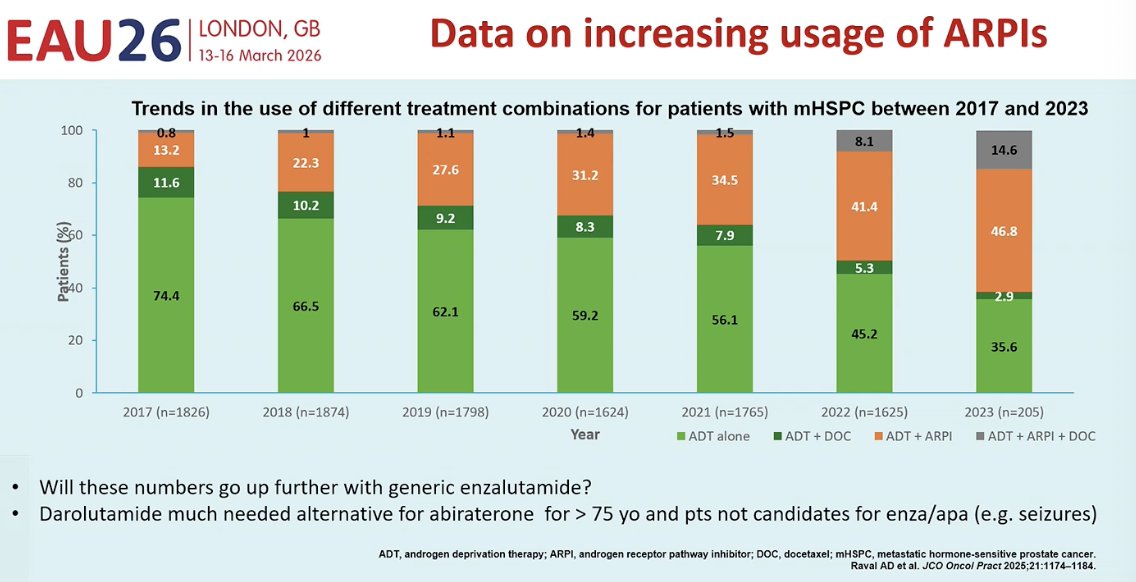
Notably, he also showed that treatment patterns in the United States are gradually shifting toward greater use of ARPIs. Between 2017 and 2023, the proportion of patients receiving ADT alone has steadily declined, while the use of ADT + ARPI, with or without docetaxel, has increased. Despite this progress, he raised two key questions moving forward: whether ARPI use will increase further as generic enzalutamide becomes available, and whether darolutamide may fill an important gap as an alternative for patients who are not candidates for abiraterone (e.g., >75 years) or who have contraindications to enzalutamide or apalutamide, such as seizure risk.
Dr. Sweeney concluded by sharing his vision for the future of mHSPC management, emphasizing several priorities that could help improve outcomes and reduce confusion in clinical practice:
- Global collaboration to identify reliable and affordable biomarkers
- Broad global access to biomarker testing to guide treatment decisions
- Better identification of who benefits from treatment intensification, such as docetaxel in mHSPC
- Maximizing efficacy while minimizing toxicity through more precise patient selection
- Advances in pharmacogenetics, similar to DPYD testing, are used to avoid severe toxicity with 5-FU
- Development of comparable predictive markers for mHSPC therapies
- Lower drug prices and the emergence of generics are improving treatment accessibility
- Reduced confusion for clinicians, supported by clearer data
- Consistent guidelines and unequivocal messaging to guide treatment decisions worldwide
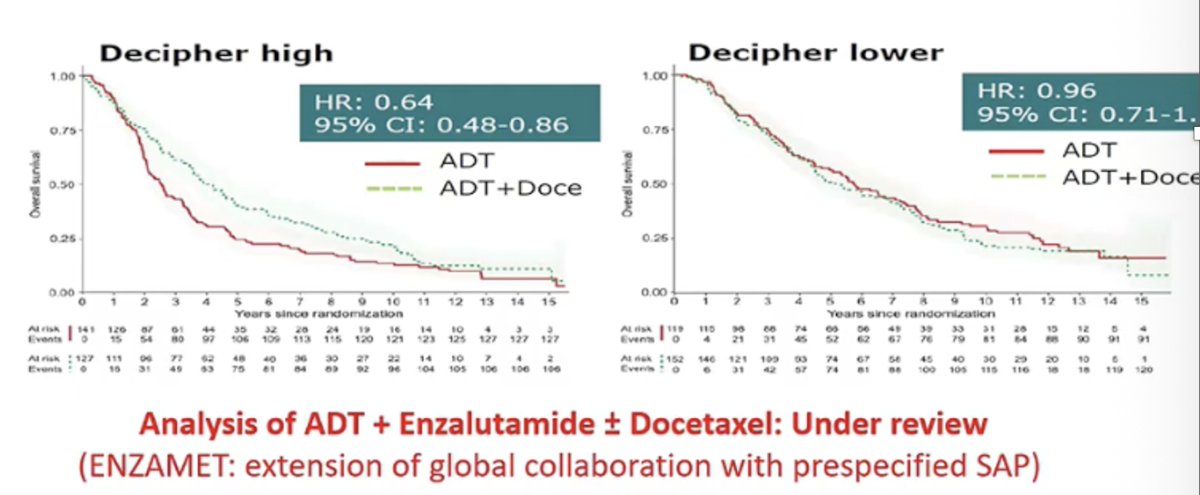
Lastly, he highlighted another potential model for consensus building through biomarker-driven patient selection. Using data from STAMPEDE, investigators evaluated the Decipher genomic classifier and found it may help identify which patients derive benefit from docetaxel when added to ADT. In this analysis, patients with a high Decipher score appeared to benefit from docetaxel, whereas those with lower scores derived little additional benefit. Building on this collaborative effort, investigators are now extending the analysis to the ENZAMET dataset3 to further determine which patients truly benefit from docetaxel, representing another step toward more precise, biomarker-guided treatment selection in mHSPC.
He concluded by emphasizing a simple message: ADT + ARPI should be the default backbone of therapy for all patients with mHSPC. He expressed hope that, moving forward, real-world practice will increasingly align with guideline recommendations so that more patients receive evidence-based treatment intensification.
Presented by: Christopher Sweeney, MBBS, South Australian Immunogenomics Cancer Institute, University of Adelaide, Adelaide, Australia
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:
- Smith MR, Hussain M, Saad F, Fizazi K, Sternberg CN, Crawford ED, Kopyltsov E, Park CH, Alekseev B, Montesa-Pino Á, Ye D, Parnis F, Cruz F, Tammela TLJ, Suzuki H, Utriainen T, Fu C, Uemura M, Méndez-Vidal MJ, Maughan BL, Joensuu H, Thiele S, Li R, Kuss I, Tombal B; ARASENS Trial Investigators. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142. doi: 10.1056/NEJMoa2119115. Epub 2022 Feb 17. PMID: 35179323; PMCID: PMC9844551.
- Kyriakopoulos CE, Chen YH, Carducci MA, Liu G, Jarrard DF, Hahn NM, Shevrin DH, Dreicer R, Hussain M, Eisenberger M, Kohli M, Plimack ER, Vogelzang NJ, Picus J, Cooney MM, Garcia JA, DiPaola RS, Sweeney CJ. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J Clin Oncol. 2018 Apr 10;36(11):1080-1087. doi: 10.1200/JCO.2017.75.3657. Epub 2018 Jan 31. PMID: 29384722; PMCID: PMC5891129.
- Sweeney CJ, Martin AJ, Stockler MR, Begbie S, Cheung L, Chi KN, Chowdhury S, Frydenberg M, Horvath LG, Joshua AM, Lawrence NJ, Marx G, McCaffrey J, McDermott R, McJannett M, North SA, Parnis F, Parulekar W, Pook DW, Reaume MN, Sandhu SK, Tan A, Tan TH, Thomson A, Vera-Badillo F, Williams SG, Winter D, Yip S, Zhang AY, Zielinski RR, Davis ID; ENZAMET trial investigators and Australian and New Zealand Urogenital and Prostate Cancer Trials Group. Testosterone suppression plus enzalutamide versus testosterone suppression plus standard antiandrogen therapy for metastatic hormone-sensitive prostate cancer (ENZAMET): an international, open-label, randomised, phase 3 trial. Lancet Oncol. 2023 Apr;24(4):323-334. doi: 10.1016/S1470-2045(23)00063-3. PMID: 36990608.
- Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, Özgüroğlu M, Ye D, Feyerabend S, Protheroe A, Sulur G, Luna Y, Li S, Mundle S, Chi KN. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2019 May;20(5):686-700. doi: 10.1016/S1470-2045(19)30082-8. Epub 2019 Apr 12. PMID: 30987939.
- Vale CL, Fisher DJ, Godolphin PJ, Rydzewska LH, Boher JM, Burdett S, Chen YH, Clarke NW, Fizazi K, Gravis G, James ND, Liu G, Matheson D, Murphy L, Oldroyd RE, Parmar MKB, Rogozinska E, Sfumato P, Sweeney CJ, Sydes MR, Tombal B, White IR, Tierney JF; STOPCAP Collaboration. Which patients with metastatic hormone-sensitive prostate cancer benefit from docetaxel: a systematic review and meta-analysis of individual participant data from randomised trials. Lancet Oncol. 2023 Jul;24(7):783-797. doi: 10.1016/S1470-2045(23)00230-9. PMID: 37414011; PMCID: PMC7616350.