(UroToday.com) The 2026 European Association of Urology (EAU) Annual Meeting held in London, U.K., between March 13th and 16th 2026, was host to the Hormone-sensitive metastatic prostate cancer: Thematic Session. Dr. Gero Kramer discussed Who benefits from intensification with docetaxel?
Dr. Kramer began by emphasizing that ADT + ARPI doublet therapy is now the standard of care for patients with metastatic hormone-sensitive prostate cancer (mHSPC), a recommendation consistently reflected across contemporary clinical guidelines. Data from multiple phase III trials, including LATITUDE, STAMPEDE, ENZAMET, ARCHES, TITAN, and ARANOTE, demonstrate a clear overall survival benefit with the addition of an ARPI to ADT across different disease volumes.1-6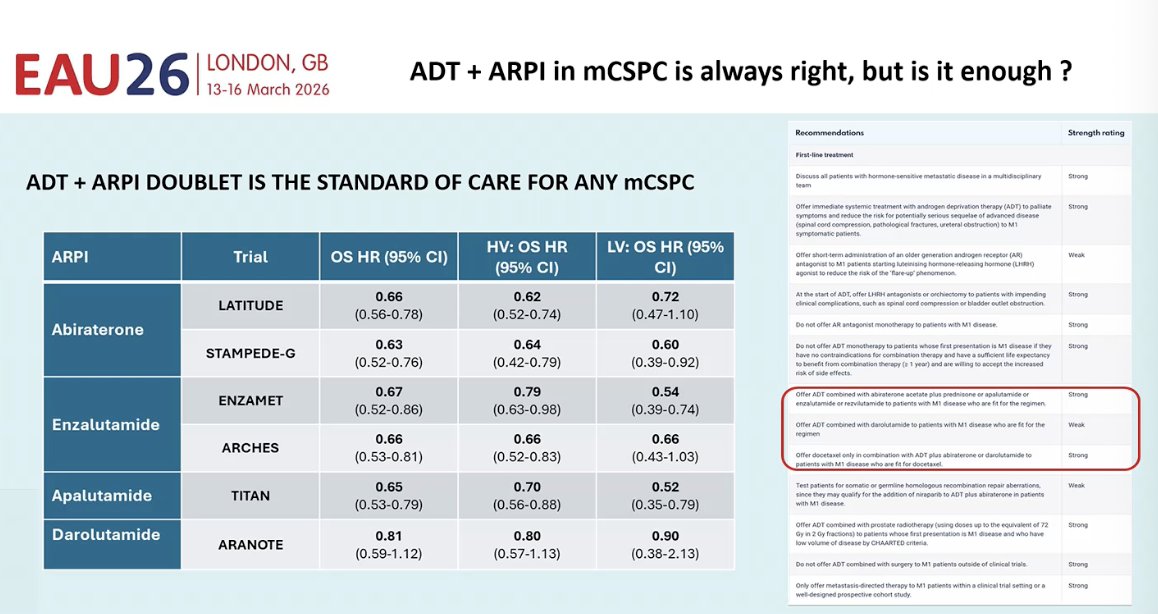
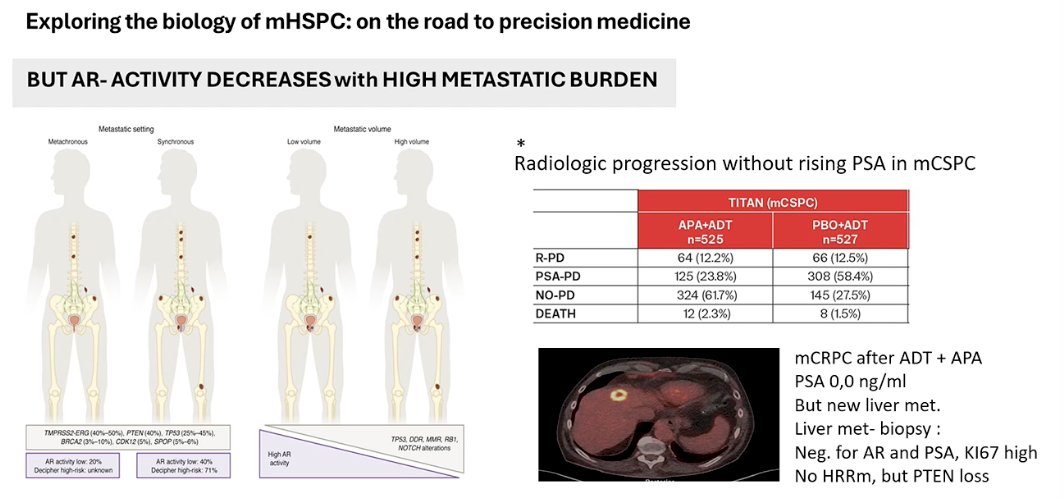
Dr. Kramer then discussed the emerging biological differences between patients with high- and low-volume mHSPC, noting that distinct genomic profiles may underlie these clinical phenotypes. For example, alterations such as PTEN loss appear more frequently in patients with higher metastatic burden, suggesting different tumor biology. He also highlighted data from the TITAN trial5 showing that approximately 10% of patients may experience radiologic progression without a corresponding rise in PSA, reflecting AR-independent disease biology. As an example, he presented a case of a patient treated with ADT + apalutamide who developed a new liver metastasis despite a PSA of 0.0 ng/mL; biopsy confirmed an AR- and PSA-negative tumor with high Ki-67 and PTEN loss, illustrating the potential emergence of aggressive AR-independent clones.
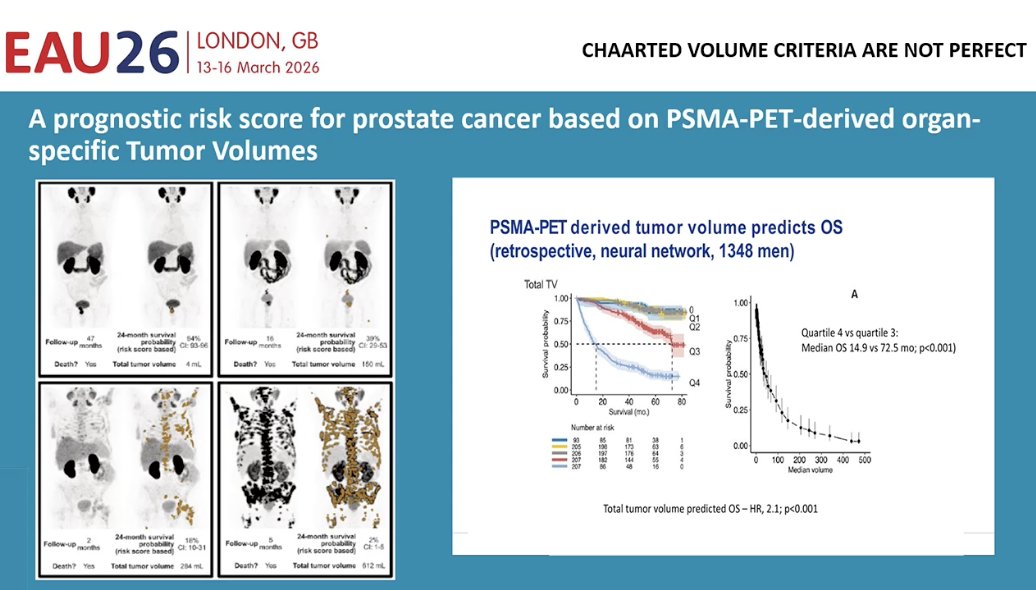
He also noted that current clinical definitions of disease volume, such as the CHAARTED criteria, may be imperfect and may not fully capture the biological heterogeneity of mHSPC. Emerging data suggest that PSMA-PET–derived tumor burden may provide a more precise prognostic assessment. In a retrospective analysis using neural network modeling in more than 1,300 patients, higher total tumor volume on PSMA-PET was strongly associated with worse overall survival. Patients with the highest PSMA-derived tumor burden had markedly shorter survival compared with those with lower tumor volumes, highlighting the potential of advanced imaging-based metrics to refine risk stratification beyond traditional high- versus low-volume classifications.7
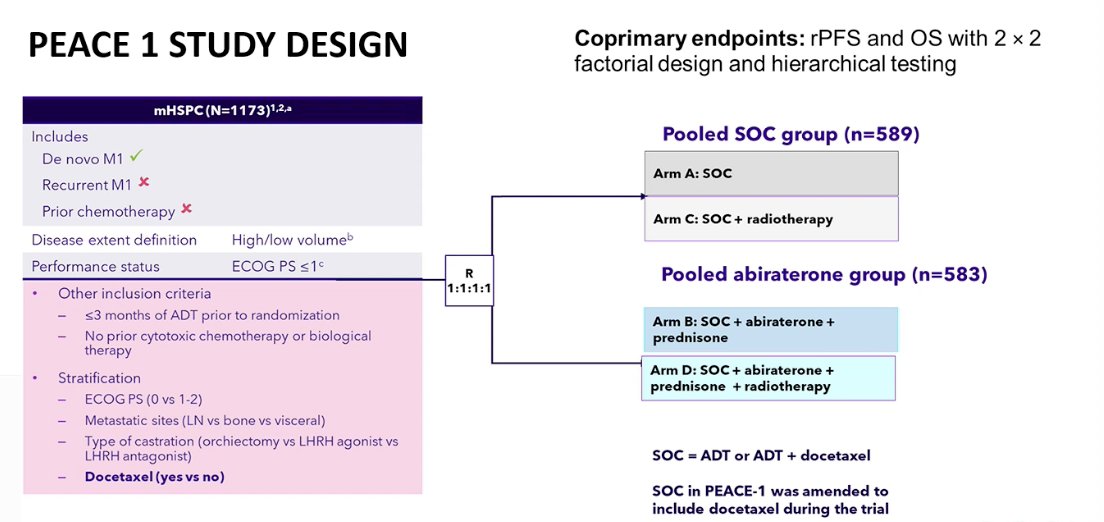
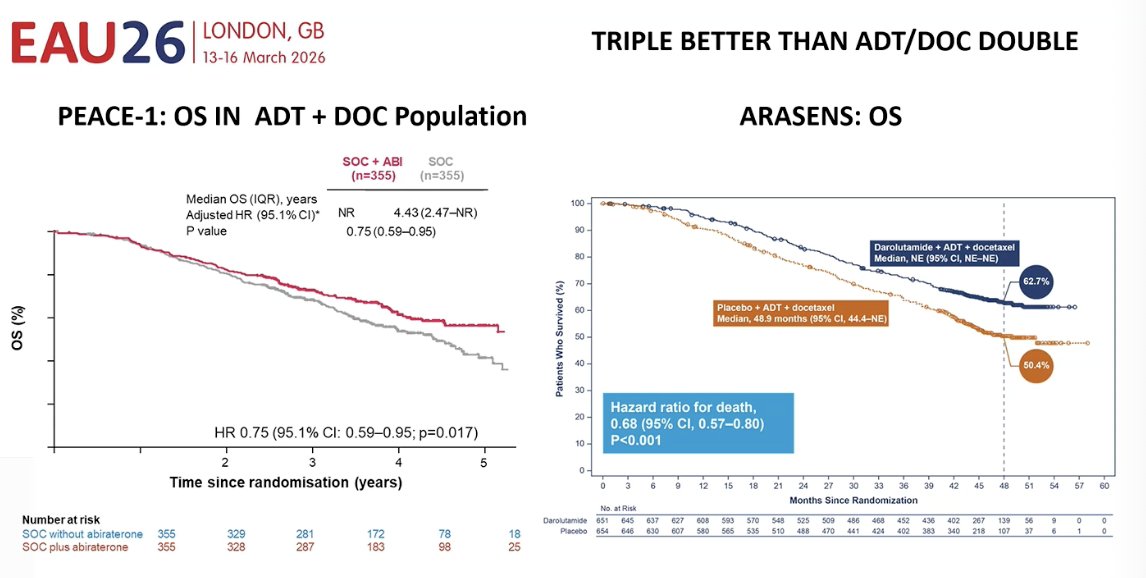
To address the question of treatment intensification, Dr. Kramer discussed the PEACE-1 trial, a phase III study evaluating the addition of abiraterone to standard of care in patients with mHSPC. The trial used a 2 × 2 factorial design and enrolled patients with de novo or recurrent metastatic disease, stratified by disease volume and docetaxel use. Patients were randomized to receive standard of care (ADT with or without docetaxel) with or without abiraterone and with or without prostate radiotherapy. The co-primary endpoints were radiographic progression-free survival (rPFS) and overall survival (OS).8 The study design is shown below.
Furthermore, he discussed the ARASENS trial, a phase III study evaluating the addition of darolutamide to ADT and docetaxel in patients with mHSPC. In this study, 1,306 patients who were candidates for both ADT and docetaxel were randomized to receive darolutamide plus ADT and docetaxel or placebo plus ADT and docetaxel. The primary endpoint was overall survival, with secondary endpoints including time to castration-resistant disease, symptomatic skeletal events, pain progression, and initiation of subsequent therapy.1

Results from both trials suggest that triplet therapy provides greater benefit than ADT + docetaxel alone. In the PEACE-1 study, the addition of docetaxel to ADT and abiraterone significantly improved overall survival compared with ADT + Abiraterone alone (HR 0.75). Similarly, in the ARASENS trial, the addition of docetaxel to darolutamide and ADT l led to a significant improvement in overall survival, reducing the risk of death by 32% (HR 0.68). Together, these trials support treatment intensification with triplet therapy in appropriate patients with mHSPC.1-8
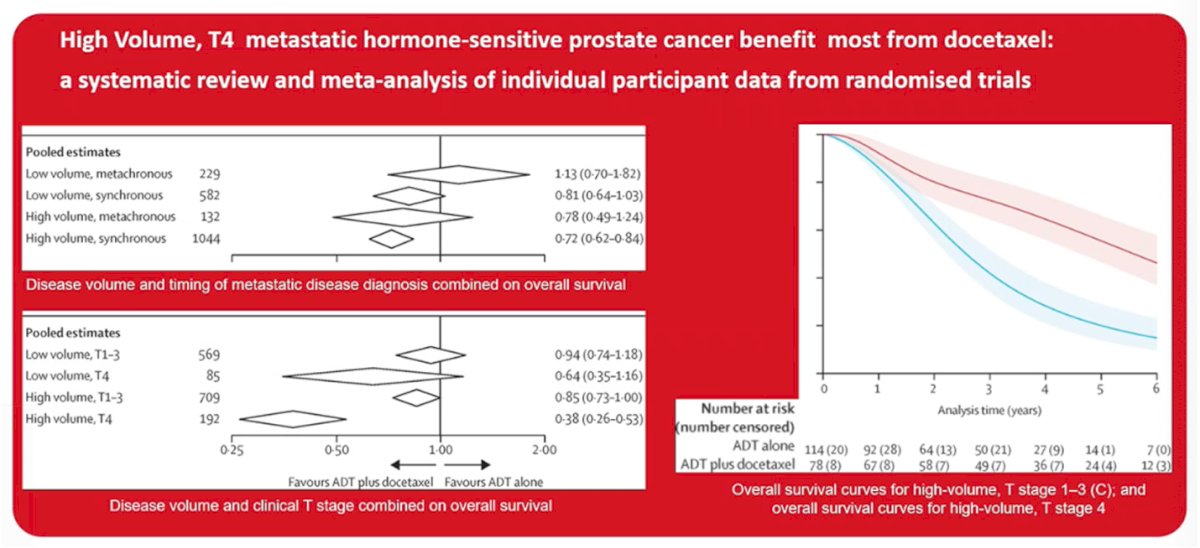
Dr. Kramer also discussed a meta-analysis of individual participant data from randomized trials evaluating the benefit of docetaxel in mHSPC. The analysis showed that patients with high-volume synchronous disease derive the greatest benefit from the addition of docetaxel to ADT, with a clear improvement in overall survival. In contrast, the benefit appeared more limited in patients with low-volume or metachronous disease.
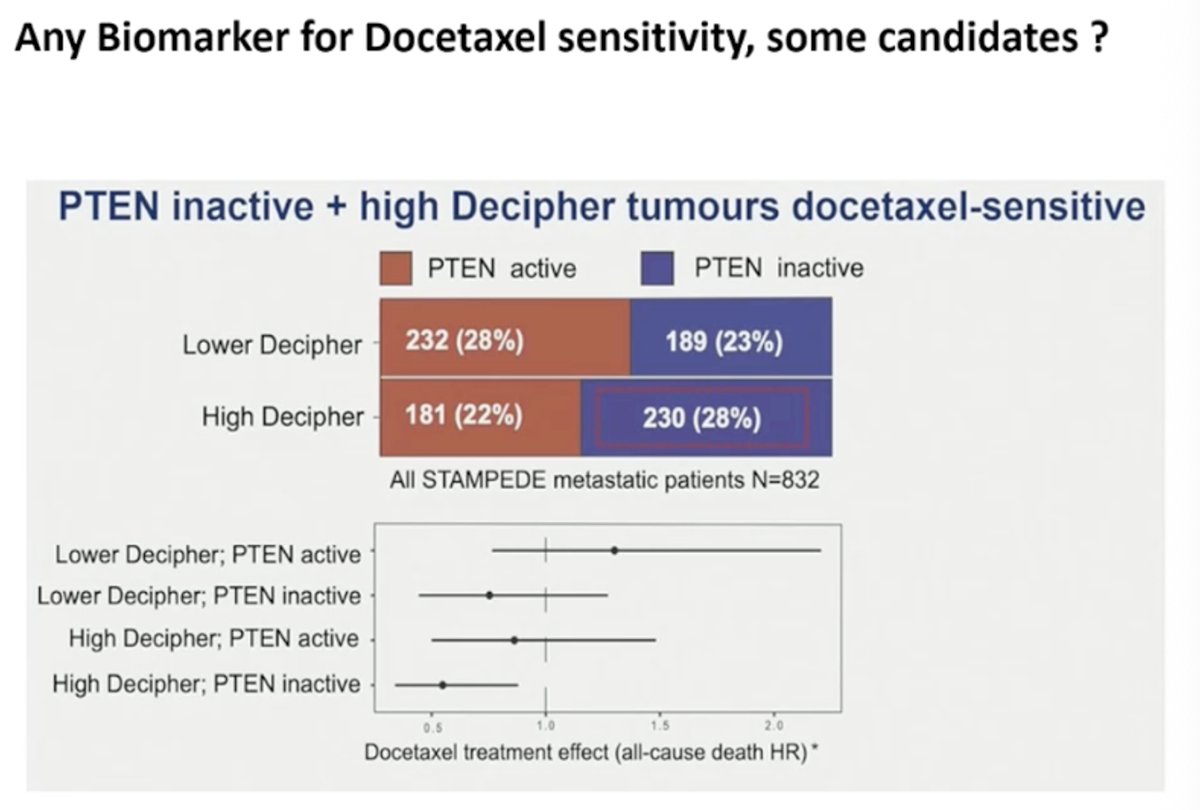
There are emerging efforts to identify biomarkers that may predict sensitivity to docetaxel. Data from translational analyses suggest that tumors with PTEN loss combined with a high Decipher genomic score may be more sensitive to docetaxel. In analyses of metastatic patients from the STAMPEDE dataset, this molecular profile appeared to identify a subgroup with greater benefit from docetaxel, highlighting the potential for biomarker-guided treatment selection in the future.
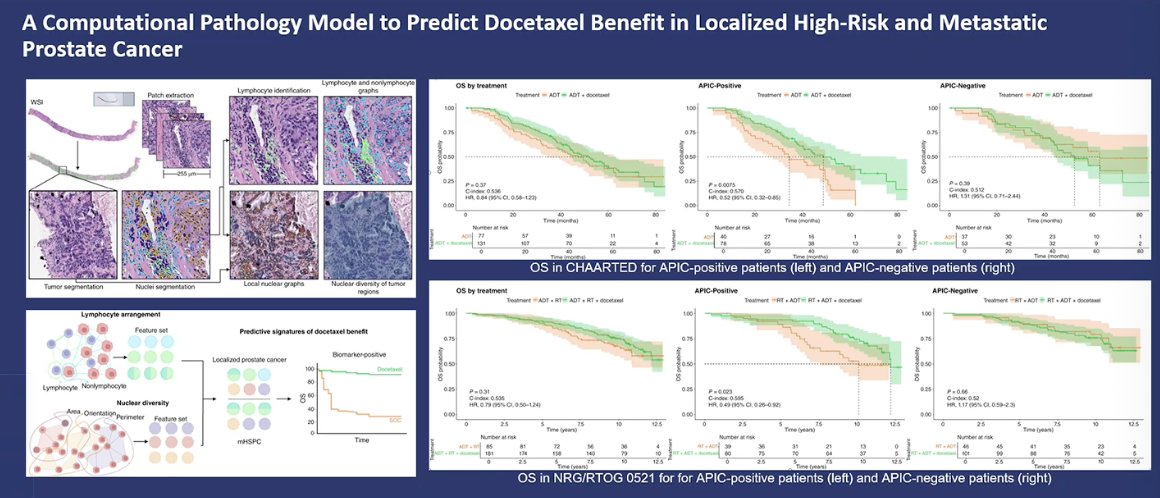
He also discussed emerging work using computational pathology to predict which patients may benefit from docetaxel. In this approach, artificial intelligence analyzes prostate biopsy images to quantify features such as nuclear heterogeneity and tumor architecture. Using these image-based biomarkers, investigators developed the APIC score, which stratifies patients into APIC-positive and APIC-negative groups. In retrospective analyses of trials such as CHAARTED and NRG/RTOG 0521, patients classified as APIC-positive appeared to derive a survival benefit from the addition of docetaxel, suggesting that AI-driven pathology models may help guide treatment selection in the future.
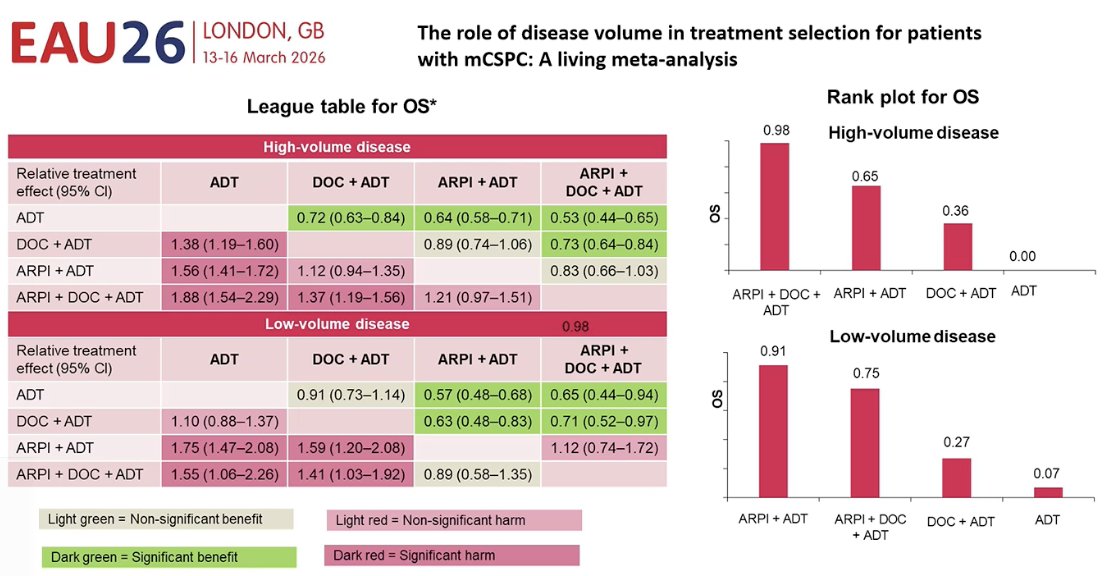
He also reviewed several meta-analyses evaluating the role of disease volume in treatment selection. These analyses consistently show that patients with high-volume mCSPC derive the greatest benefit from treatment intensification with docetaxel. In contrast, for patients with low-volume disease, outcomes appear to be driven primarily by ARPI-based therapy, with ADT + ARPI generally providing the greatest survival benefit.
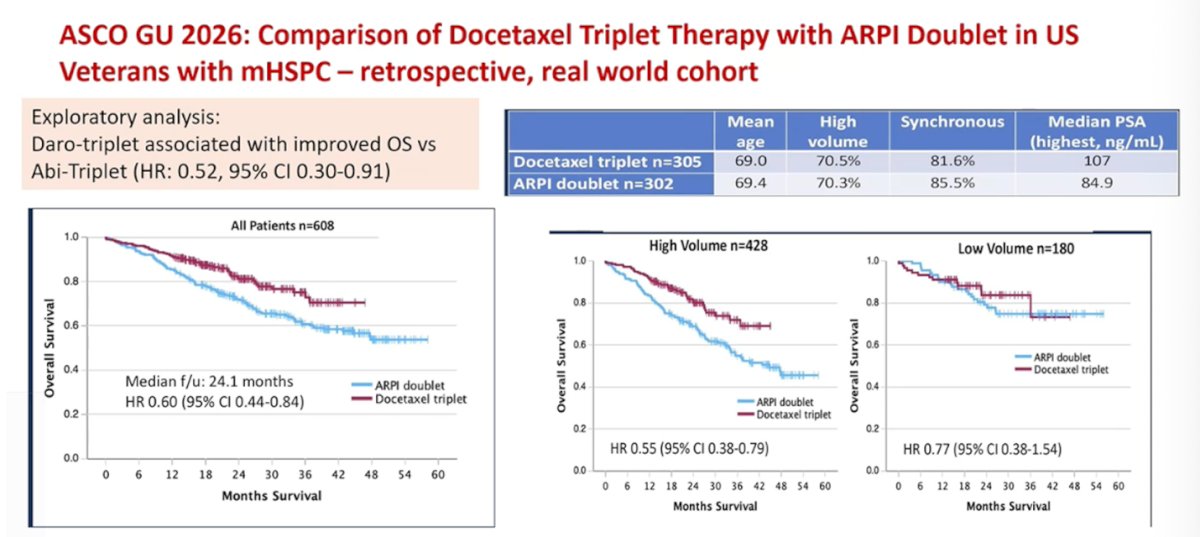
Dr. Kramer also highlighted recent real-world data comparing triplet therapy with ARPI-based doublets. In a retrospective analysis of U.S. veterans with mHSPC presented at ASCO GU 2026, docetaxel-based triplet therapy was associated with improved overall survival compared with ADT + ARPI doublet therapy. Although the study was retrospective and relatively small, the findings suggested a potential survival advantage with triplet therapy, particularly among patients with high-volume disease, providing additional real-world support for treatment intensification in selected patients.
Dr. Kramer also discussed the ARASAFE study, presented at ESMO 2025, which evaluated two different docetaxel schedules in patients receiving darolutamide + ADT for mHSPC. The study compared the standard regimen of docetaxel 75 mg/m² every three weeks with a modified regimen of 50 mg/m² every two weeks. The two-week schedule was associated with significantly lower rates of grade 3–5 adverse events (61.2% vs 78.9%), suggesting that a biweekly docetaxel regimen may represent a safer alternative when used as part of triplet therapy.

Dr. Kramer also discussed emerging data suggesting that treatment sequencing within triplet therapy may influence outcomes. In a retrospective multicenter Austrian real-world cohort of nearly 100 patients with mCSPC, non-simultaneous initiation of triplet therapy was associated with worse outcomes. Specifically, starting an ARPI before chemotherapy was linked to shorter progression-free survival (p=0.025). The hypothesis is that early ARPI exposure may suppress tumor proliferation, potentially reducing the cytotoxic impact of docetaxel, which is most effective in actively dividing cells. These findings suggest that administering docetaxel shortly after ADT initiation, before introducing an ARPI, may optimize the biological effectiveness of chemotherapy within triplet therapy.
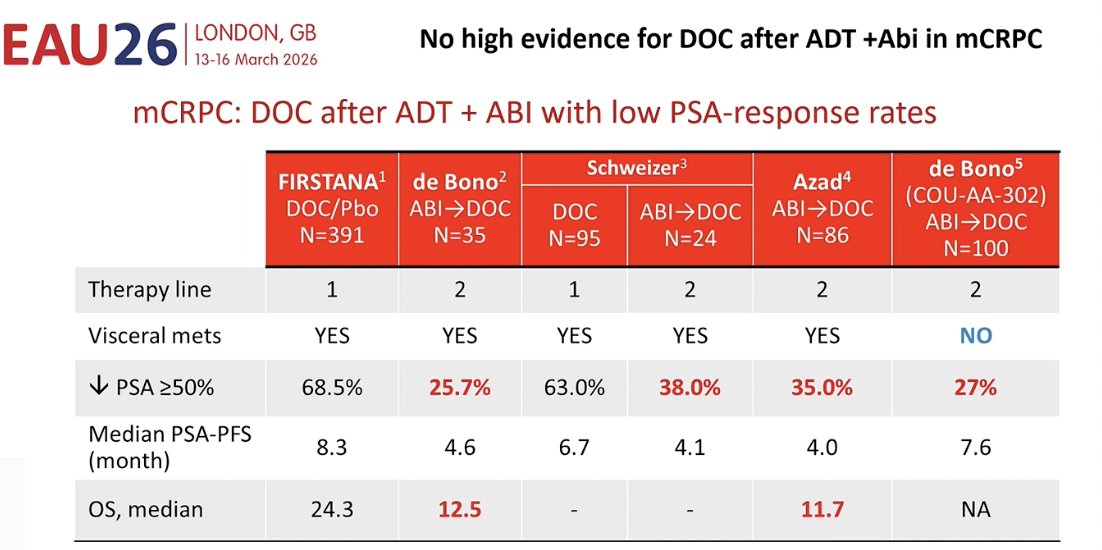
Notably, he highlighted that there is limited high-level evidence supporting the use of docetaxel after prior treatment with ADT + abiraterone in the mCRPC setting. Available data from several studies suggest relatively low PSA response rates when docetaxel is administered after abiraterone, generally ranging between approximately 25% and 38%. These findings raise concerns about potential cross-resistance and suggest that the effectiveness of docetaxel may be reduced when used after prior ARPI exposure.
Finally, he noted that expert opinion from the APCCC also reflects a selective approach to treatment intensification. In voting during the consensus meeting, most panelists supported the use of triplet therapy (ADT + docetaxel + ARPI) in the majority of patients with high-burden mHSPC who are fit for chemotherapy, although a substantial proportion favored restricting it to selected patients. When asked what factors most influence the decision to use triplet therapy, the leading considerations were high-volume disease and synchronous metastatic presentation, highlighting that disease burden and timing of metastases remain key clinical determinants when selecting patients for treatment intensification.

Dr. Kramer concluded his presentation with the following key points:
- The “classic triplet” (ADT + darolutamide + docetaxel) likely provides benefit over ADT + ARPI doublet in patients with biologically aggressive tumors
- These patients are often characterized by high tumor volume, large local tumor burden, and PSA-low–secreting disease
- Biomarker-driven treatment selection is an active area of research
- Potential candidates include APIC, Decipher, PTEN, RB1, SPOP, and other genomic alterations
- Alternative treatment schedules are also being explored
- A biweekly docetaxel regimen may improve tolerability, and treatment sequencing within triplet therapy may influence outcomes (e.g., darolutamide after docetaxel)
- It remains unclear whether one triplet strategy (e.g., darolutamide-based) is superior to others, such as abiraterone-based triplets
- Novel triplet strategies are also under investigation (PSMAdd, CAPItello, AMPLITUDE), raising the question of what role the classic triplet will play moving forward
Presented by: Gero Kramer, MD, Urologist, Medical University of Vienna, Vienna, Austria.
Written by: Julian Chavarriaga, MD, Assistant Professor, Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on X during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
References:- Smith MR, Hussain M, Saad F, Fizazi K, Sternberg CN, Crawford ED, Kopyltsov E, Park CH, Alekseev B, Montesa-Pino Á, Ye D, Parnis F, Cruz F, Tammela TLJ, Suzuki H, Utriainen T, Fu C, Uemura M, Méndez-Vidal MJ, Maughan BL, Joensuu H, Thiele S, Li R, Kuss I, Tombal B; ARASENS Trial Investigators. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022 Mar 24;386(12):1132-1142. doi: 10.1056/NEJMoa2119115. Epub 2022 Feb 17. PMID: 35179323; PMCID: PMC9844551.
- Kyriakopoulos CE, Chen YH, Carducci MA, Liu G, Jarrard DF, Hahn NM, Shevrin DH, Dreicer R, Hussain M, Eisenberger M, Kohli M, Plimack ER, Vogelzang NJ, Picus J, Cooney MM, Garcia JA, DiPaola RS, Sweeney CJ. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer: Long-Term Survival Analysis of the Randomized Phase III E3805 CHAARTED Trial. J Clin Oncol. 2018 Apr 10;36(11):1080-1087. doi: 10.1200/JCO.2017.75.3657. Epub 2018 Jan 31. PMID: 29384722; PMCID: PMC5891129.
- Sweeney CJ, Martin AJ, Stockler MR, Begbie S, Cheung L, Chi KN, Chowdhury S, Frydenberg M, Horvath LG, Joshua AM, Lawrence NJ, Marx G, McCaffrey J, McDermott R, McJannett M, North SA, Parnis F, Parulekar W, Pook DW, Reaume MN, Sandhu SK, Tan A, Tan TH, Thomson A, Vera-Badillo F, Williams SG, Winter D, Yip S, Zhang AY, Zielinski RR, Davis ID; ENZAMET trial investigators and Australian and New Zealand Urogenital and Prostate Cancer Trials Group. Testosterone suppression plus enzalutamide versus testosterone suppression plus standard antiandrogen therapy for metastatic hormone-sensitive prostate cancer (ENZAMET): an international, open-label, randomised, phase 3 trial. Lancet Oncol. 2023 Apr;24(4):323-334. doi: 10.1016/S1470-2045(23)00063-3. PMID: 36990608.
- Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, Özgüroğlu M, Ye D, Feyerabend S, Protheroe A, Sulur G, Luna Y, Li S, Mundle S, Chi KN. Abiraterone acetate plus prednisone in patients with newly diagnosed high-risk metastatic castration-sensitive prostate cancer (LATITUDE): final overall survival analysis of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2019 May;20(5):686-700. doi: 10.1016/S1470-2045(19)30082-8. Epub 2019 Apr 12. PMID: 30987939.
- Chi KN, Chowdhury S, Bjartell A, Chung BH, Pereira de Santana Gomes AJ, Given R, Juárez A, Merseburger AS, Özgüroğlu M, Uemura H, Ye D, Brookman-May S, Mundle SD, McCarthy SA, Larsen JS, Sun W, Bevans KB, Zhang K, Bandyopadhyay N, Agarwal N. Apalutamide in Patients With Metastatic Castration-Sensitive Prostate Cancer: Final Survival Analysis of the Randomized, Double-Blind, Phase III TITAN Study. J Clin Oncol. 2021 Jul 10;39(20):2294-2303. doi: 10.1200/JCO.20.03488. Epub 2021 Apr 29. PMID: 33914595.
- Saad F, Vjaters E, Shore N, Olmos D, Xing N, Pereira de Santana Gomes AJ, Cesar de Andrade Mota A, Salman P, Jievaltas M, Ulys A, Jakubovskis M, Kopyltsov E, Han W, Nevalaita L, Testa I, Le Berre MA, Kuss I, Haresh KP; ARANOTE Study Investigators. Darolutamide in Combination With Androgen-Deprivation Therapy in Patients With Metastatic Hormone-Sensitive Prostate Cancer From the Phase III ARANOTE Trial. J Clin Oncol. 2024 Dec 20;42(36):4271-4281. doi: 10.1200/JCO-24-01798. Epub 2024 Sep 16. PMID: 39279580; PMCID: PMC11654448.
- Seifert R, Rasul S, Seifert KE, Eveslage M, Rahbar Nikoukar L, Kessel K, Schäfers M, Yu J, Haug AR, Hacker M, Bögemann M, Bodei L, Morris MJ, Hofman MS, Rahbar K. A Prognostic Risk Score for Prostate Cancer Based on PSMA PET-derived Organ-specific Tumor Volumes. Radiology. 2023 May;307(4):e222010. doi: 10.1148/radiol.222010. Epub 2023 Apr 18. PMID: 37070991; PMCID: PMC10838189.
- Fizazi K, Foulon S, Carles J, Roubaud G, McDermott R, Fléchon A, Tombal B, Supiot S, Berthold D, Ronchin P, Kacso G, Gravis G, Calabro F, Berdah JF, Hasbini A, Silva M, Thiery-Vuillemin A, Latorzeff I, Mourey L, Laguerre B, Abadie-Lacourtoisie S, Martin E, El Kouri C, Escande A, Rosello A, Magne N, Schlurmann F, Priou F, Chand-Fouche ME, Freixa SV, Jamaluddin M, Rieger I, Bossi A; PEACE-1 investigators. Abiraterone plus prednisone added to androgen deprivation therapy and docetaxel in de novo metastatic castration-sensitive prostate cancer (PEACE-1): a multicentre, open-label, randomised, phase 3 study with a 2 × 2 factorial design. Lancet. 2022 Apr 30;399(10336):1695-1707. doi: 10.1016/S0140-6736(22)00367-1. Epub 2022 Apr 8. PMID: 35405085.