(UroToday.com) The 2026 GU ASCO annual meeting featured a prostate cancer session and a presentation by Dr. Alicia Morgans discussing the impact of hospitalizations on health-related quality of life and overall survival in metastatic castration sensitive prostate cancer (mCSPC) from the ARANOTE trial. Management of mCSPC has evolved substantially over the past decade, with several phase III trials demonstrating improved overall survival and progression free survival through the addition of androgen receptor pathway inhibitors to ADT treatments improving overall survival and progression-free survival. Darolutamide is a structurally distinct androgen receptor pathway inhibitor designed to minimize drug–drug interactions and adverse events.
In the phase III ARANOTE trial, darolutamide + ADT significantly improved radiographic progression-free survival versus ADT alone (HR 0.54, 95% CI 0.41–0.71; p<0.0001).1 Importantly, all-cause hospitalization rates were comparable between darolutamide and placebo (0.426, 95% CI 0.174–1.039 versus 0.424, 95% CI 0.278–0.646). While treatment advances have improved survival and health-related quality of life, the impact of disease or treatment-related hospitalizations on health-related quality of life and overall survival in mCSPC remains poorly characterized. Using data from the ARANOTE trial, Dr. Morgans and colleagues evaluated whether hospitalizations that occurred within 60 days prior to outcome data collection – either before or during participation in the trial - have an impact on health-related quality of life and overall survival.
Health-related quality of life was assessed using the Functional Assessment of Cancer Therapy–Prostate (FACT-P) instrument. FACT-P total scores from all available study visits were modeled longitudinally with generalized estimating equations. Covariates included the number of prior all-cause hospitalizations, hospitalizations due to treatment-related adverse events, baseline pain (<4 versus ≥4), baseline ECOG performance status (0–1 versus 2), fatigue (any grade adverse event during participation in the trial), baseline age, and baseline weight. Overall survival was evaluated using time-varying Cox proportional hazards regression. Covariates for the overall survival model included treatment, treatment-emergent adverse events, and the number of prior all-cause hospitalizations.
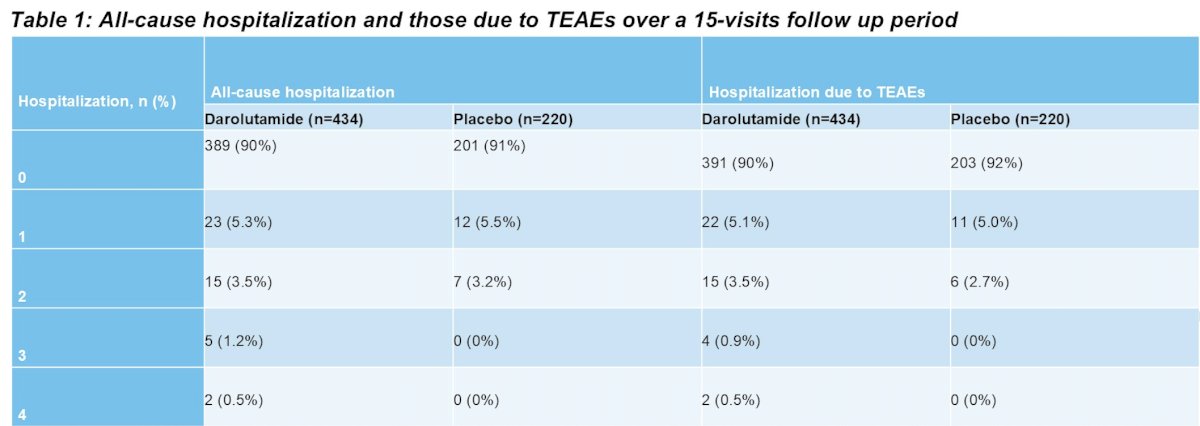
Of 654 patients, there were 64 total hospitalizations occurring within 60 days of FACT-P data collection. All cause hospitalizations occurred among 45 participants (10%) in the darolutamide group and 19 participants in the placebo group:
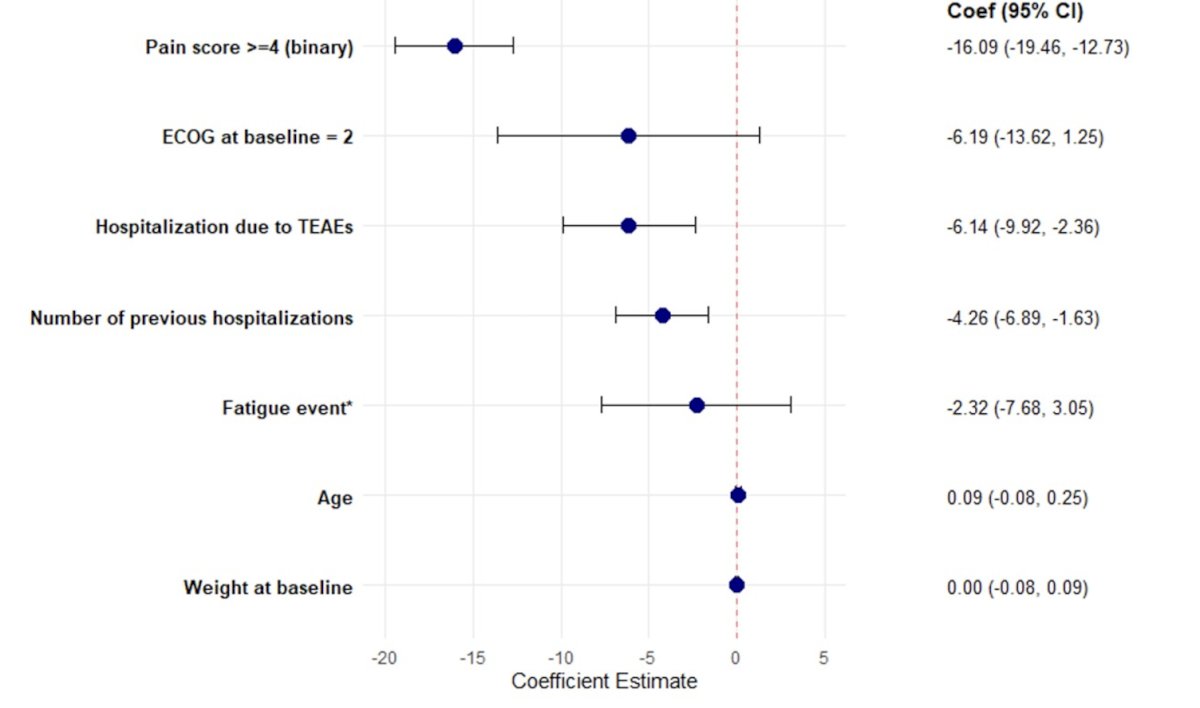
Both the number of previous hospitalizations (–4.26 points; 95% CI –6.89 to –1.63; p < 0.001) and hospitalization due to treatment-emergent adverse events (–6.14 points; 95% CI –9.92 to –2.36; p < 0.001) were significantly associated with lower FACT-P total scores. Baseline pain ≥4 was the strongest negative predictor of health-related quality of life (–16.09 points; 95% CI –19.46 to –12.73; p < 0.001). ECOG performance status of 2 at baseline (–6.19; 95% CI –13.62 to 1.25; p = 0.10) and fatigue (–2.32; 95% CI –7.68 to 3.05; p = 0.40) were also associated with lower health-related quality of life but did not reach statistical significance. Age (0.09; 95% CI –0.08 to 0.25; p = 0.29) and baseline weight (0; 95% CI –0.08 to 0.09; p = 0.96) had minimal effects:
In survival analyses, treatment-emergent adverse event-related hospitalization was not associated with mortality risk (HR 0.99, 95% CI 0.56-1.77; p = 0.98). Each additional prior hospitalization was associated with a 52% increase in the hazard of death (HR 1.52; 95% CI 1.39–1.66; p < 0.0001).
Dr. Morgans concluded her presentation discussing the impact of hospitalizations on health-related quality of life and overall survival in mCSPC from the ARANOTE trial with the following take-home points:
- Prior hospitalizations were a consistent determinant of both reduced health-related quality of life and shorter overall survival in men with mCSPC, while baseline pain was the strongest driver of health-related quality of life decline
- A post hoc analysis from the ARANOTE trial,1 found that darolutamide was associated with lower rates of hospitalization compared to placebo
- Taken together, these findings highlight that treatments that decrease hospitalization with favorable tolerability profiles, such as darolutamide, may help sustain quality of life and survival by minimizing hospitalization burden
Presented by: Alicia Morgans, MD, MPH, Genitourinary Medical Oncologist, Medical Director of Survivorship Program at Dana-Farber Cancer Institute, Boston, Massachusetts
Reference: