(UroToday.com) The 2026 SESAUA annual meeting featured a prostate cancer session and presentation by Dr. Murilo de Almeida Luz discussing PSA and alkaline phosphatase decline in the EORTC PEACE-3 study evaluating the addition of radium-223 in metastatic castration resistant prostate cancer (mCRPC) starting enzalutamide.
Previously, the PEACE-3 trial showed that adding radium-223 to enzalutamide significantly improves investigator-assessed progression-free survival and overall survival in mCRPC with bone metastases.1 At the 2026 SESAUA annual meeting, Dr. de Almeida Luz and colleagues examined the effect of the combination on the decline in PSA and alkaline phosphatase.
From November 2015 to March 2023, 446 men with mCRPC and bone metastasis were randomized 1:1 to enzalutamide alone or combined with 6 cycles of radium-223. The trial design for PEACE-3 is as follows:
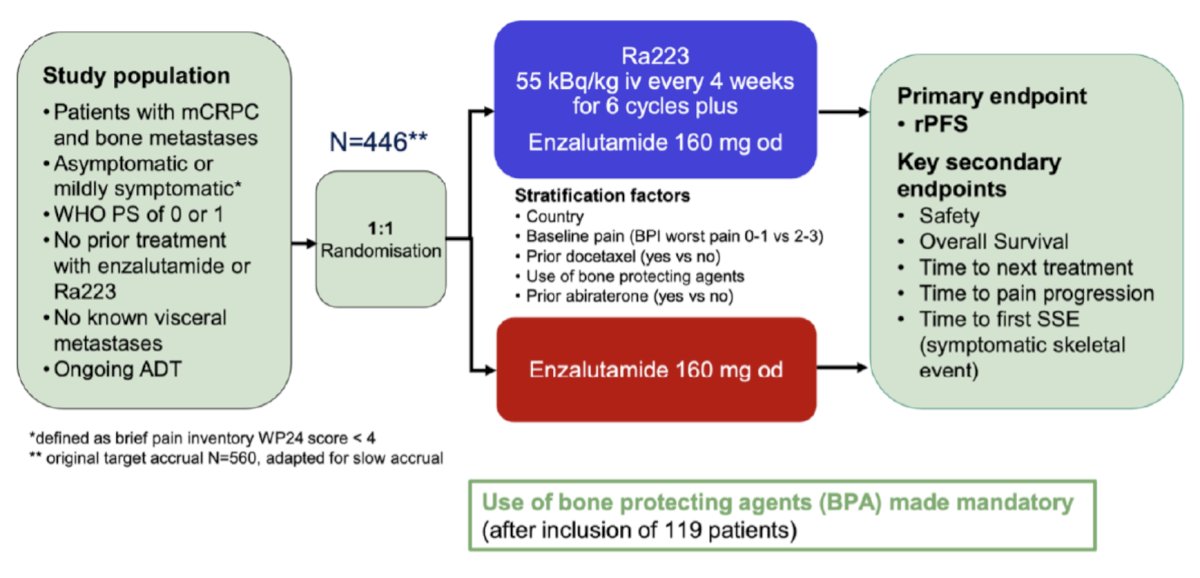
The PSA/alkaline phosphatase response rate was estimated at 6/12 months based on the drop from baseline in all PSA/alkaline phosphatase evaluable patients. For PSA, any decline ≥ 50 or 90% from baseline was considered a PSA response. For alkaline phosphatase, any decline of ≥30% from baseline was regarded as a response, with each response needing to be confirmed by a second evaluation at least three weeks later. Time to response was from treatment start until the first date a response was observed. Alkaline phosphatase normalization is a decline to ≤ 115 U/L in patients with baseline alkaline phosphatase levels>115 U/L.
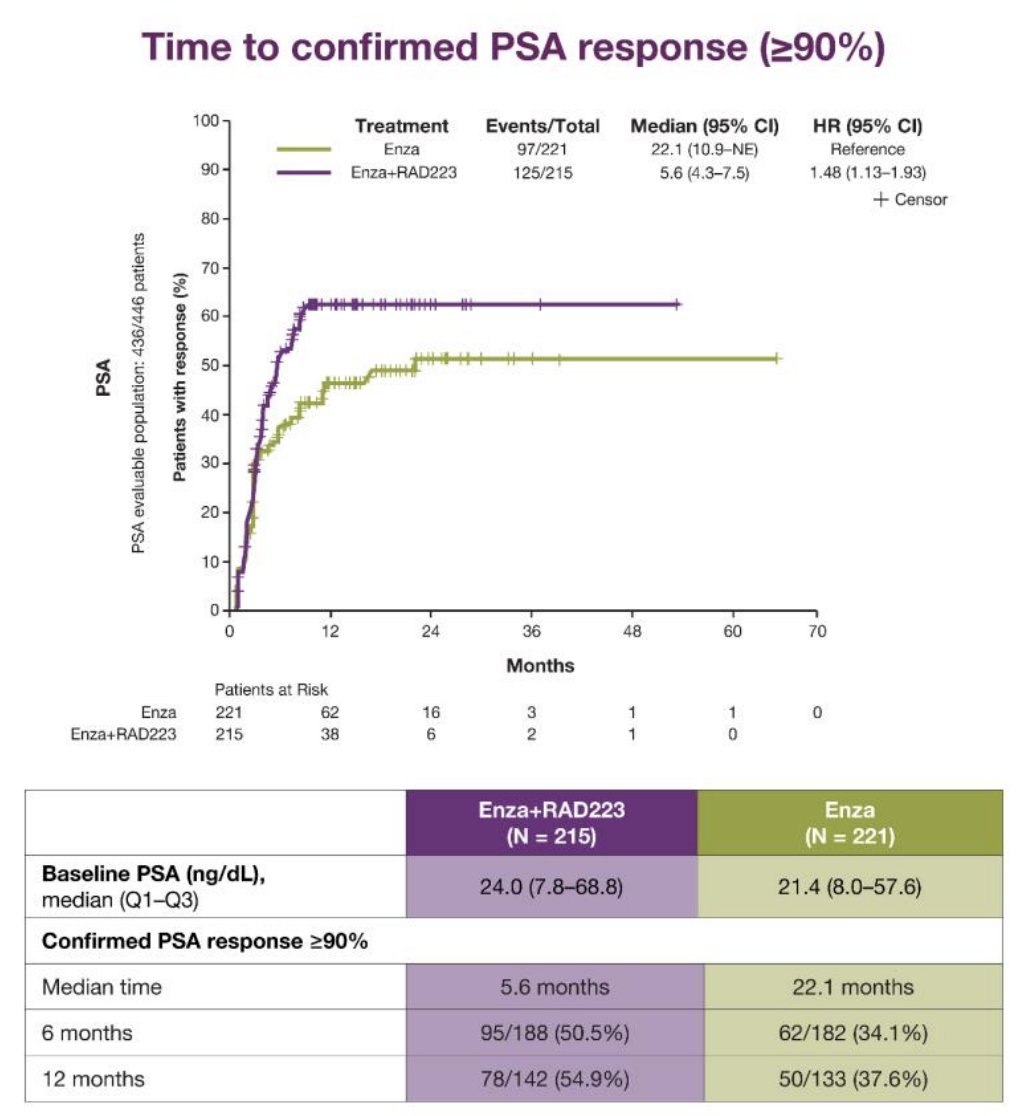
The baseline median PSA for enzalutamide + radium-223 was 24.0 (IQR 7.8-68.8) ng/dl, and 21.4 (IQR 8.0-57.6) ng/ml for enzalutamide. The median time to a PSA response > 50% in months was 2.79 (95% CI 2.56-3.02) in the enzalutamide + radium-223 arm and 2.76 (95% CI 2.63-2.79) in the enzalutamide arm (HR 1.00, 95% CI 0.80-1.24). PSA response rates ≥50% at 6 and 12 months were 77.1% (145/188) and 76.8% (109/142) in the enzalutamide + radium-223 arm, compared to 69.9% (127/182) and 66.2% (88/133) in the enzalutamide arm. The median time to a PSA response ≥ 90% was 5.6 months (95% CI 1.44-2.53) in the enzalutamide + radium-223 arm and 21. 4 months (95% CI 8.0-57.6) in the enzalutamide arm (HR 1.48, 95% CI 1.13-1.93). PSA response rates ≥90% at 6 and 12 months were 50.5% (95/188) and 54.9% (78/142) in the enzalutamide + radium-223 arm, compared to 34.1% (62/182) and 37.6% (50/133) in the enzalutamide arm:
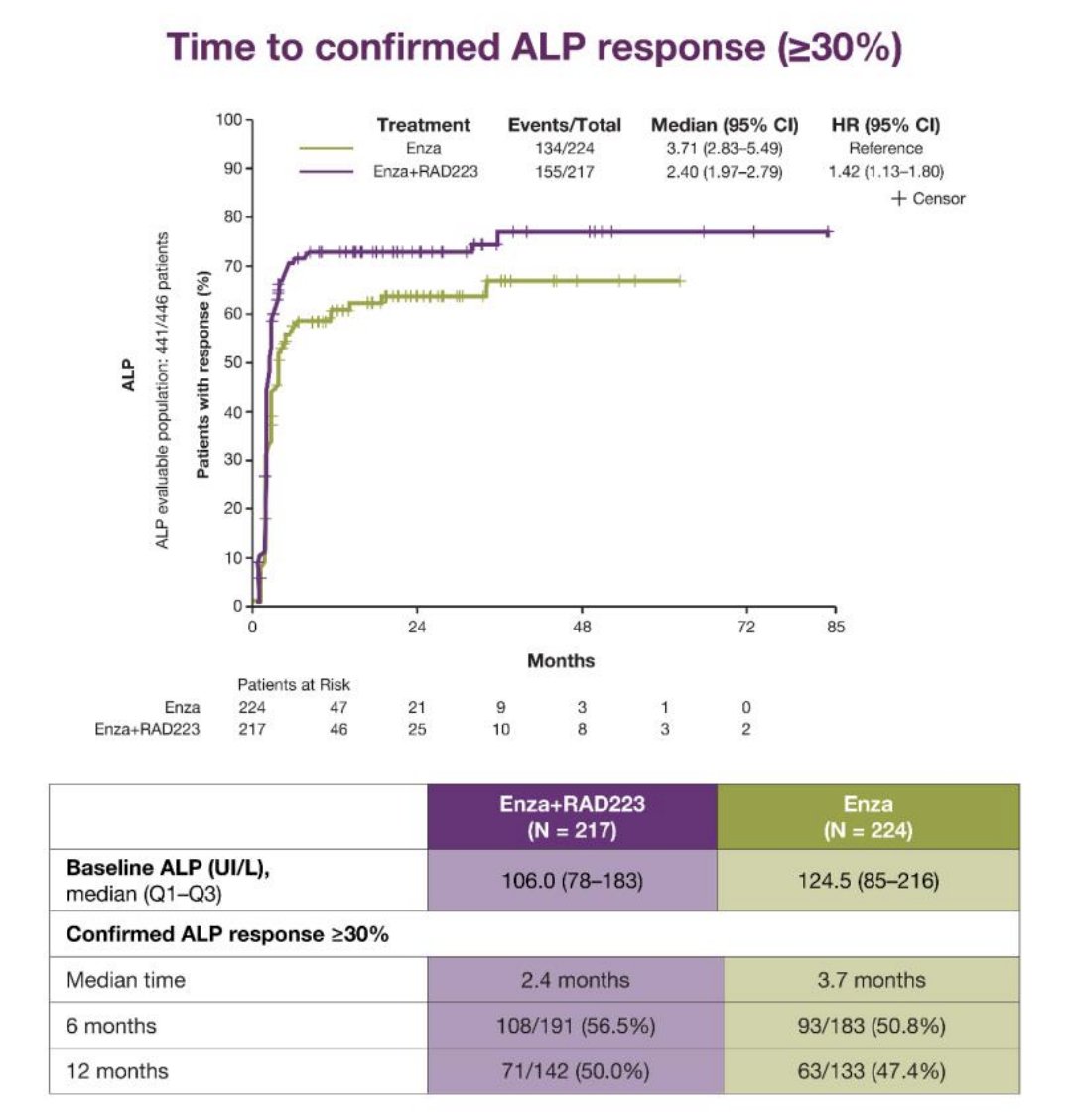
The baseline median alkaline phosphatase in the enzalutamide + radium-223 arm was 106 (IQR 78-183) UI/L, and in the enzalutamide arm was 124.5 (IQR 85-216). In the enzalutamide + radium-223 and enzalutamide arms, 45.6% (99/217) and 54.4% (122/224) of patients had alkaline phosphatase ≥ 115 UI/L at baseline. The enzalutamide + radium-223 arm had a median time to alkaline phosphatase response of> 30% of 2.40 (95% CI 1.97-2.79) months, while the enzalutamide arm had a median of 3.7 (95% CI 2.83-5.49) months (HR 1.42, 95% CI 1.13-1.80). Alkaline phosphatase >30% response rates at 6 and 12 months were 56.5% (108/191) and 50.0% (71/142) in enzalutamide + radium-223 and 50.8% (93/183) and 47.4% (63/133) for the enzalutamide arm:
The median time to alkaline phosphatase normalization in the enzalutamide + radium-223 arm was 1.97 (95% CI 1.87-2.50) months and 4.47 (95% CI 2.99-14.06) months in the enzalutamide arm (HR 1.42, 95% CI 1.13-1.80). At 6 and 12 months, the enzalutamide + radium-223 arm alkaline phosphatase normalization rates were 76.2% (64/84) and 77.4% (41/53), while 50.5% (47/93) and 61.3% (38/62) in the enzalutamide arm.
Dr. de Almeida Luz concluded his presentation discussing PSA and alkaline phosphatase decline in the EORTC PEACE-3 study with the following take-home points:
- The addition of six cycles of radium-223 to enzalutamide in the PEACE-3 trial improves PSA response time and rates (≥90%), alkaline phosphatase reduction time (≥30%), and alkaline phosphatase normalization time and rates at 6 and 12 months
- Along with significant investigator-assessed progression-free survival and overall survival results, this combination offers a more effective treatment strategy for patients with first-line mCRPC
Presented by: Murilo de Almeida Luz, MD, Hospital Erasto Gaertner, Curitiba, Brazil
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Southeastern Section of the American Urological Association (SESAUA) Annual Meeting, San Juan, PR, Wed, Mar 18 – Sat, Mar 21, 2026.Reference:
Related Content:
EAU 2026: Safety and Skeletal Event Profile of Radium-223 Combined with Enzalutamide in mCRPC: A Multicenter Retrospective Analysis in Japan
EAU 2026: Time-Dependent Survival Benefit of Enzalutamide + Radium-223 in mCRPC: Reconstructed Analysis of the PEACE-3 Trial