(UroToday.com) The 2026 SESAUA annual meeting featured a bladder cancer session and presentation by Dr. Katie Murray discussing characterization of recurrence, progression, and time to cystectomy among patients undergoing gemcitabine intravesicle system monotherapy in BCG-unresponsive high-risk non-muscle invasive bladder cancer. Patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer have limited treatment options and a high risk of disease progression.
Standard of care for BCG-unresponsive high-risk non-muscle invasive bladder cancer is radical cystectomy, however extirpative surgery is a life-changing operation associated with significant morbidity and mortality rates, as well as a negative impact on quality of life. TAR-200 is a novel intravesical drug-releasing system designed to provide sustained delivery of gemcitabine in the bladder. SunRISe-1 is an ongoing phase 2b parallel-cohort study assessing TAR-200 in patients with BCG-unresponsive high-risk non-muscle invasive bladder cancer who were ineligible for or refused radical cystectomy. At the SESAUA 2026 annual meeting, Dr. Murray and colleagues reported recurrence, progression, and time to cystectomy analyses in patients receiving TAR-200 monotherapy (Cohort 2).
Enrolled patients ≥18 years of age and ECOG performance status 0-2 had histologically confirmed CIS ± papillary disease (high-grade Ta, any T1), after adequate BCG, with the last dose ≤12 months from CIS diagnosis. TAR-200 was dosed every three weeks through week 24, then every 12 weeks until week 96. The primary endpoint was the overall complete response rate. Secondary endpoints included: duration of response, overall survival, safety, and tolerability:

Response assessments included: cystoscopy, centrally assessed urine cytology (every 12 weeks for 2 years, every 24 weeks thereafter), centrally assessed biopsy (week 24/week 48), and local imaging every 24 weeks. Patients with centrally assessed disease recurrence or progression were staged based on TNM classification by the investigator. Subsequent therapies were reported.
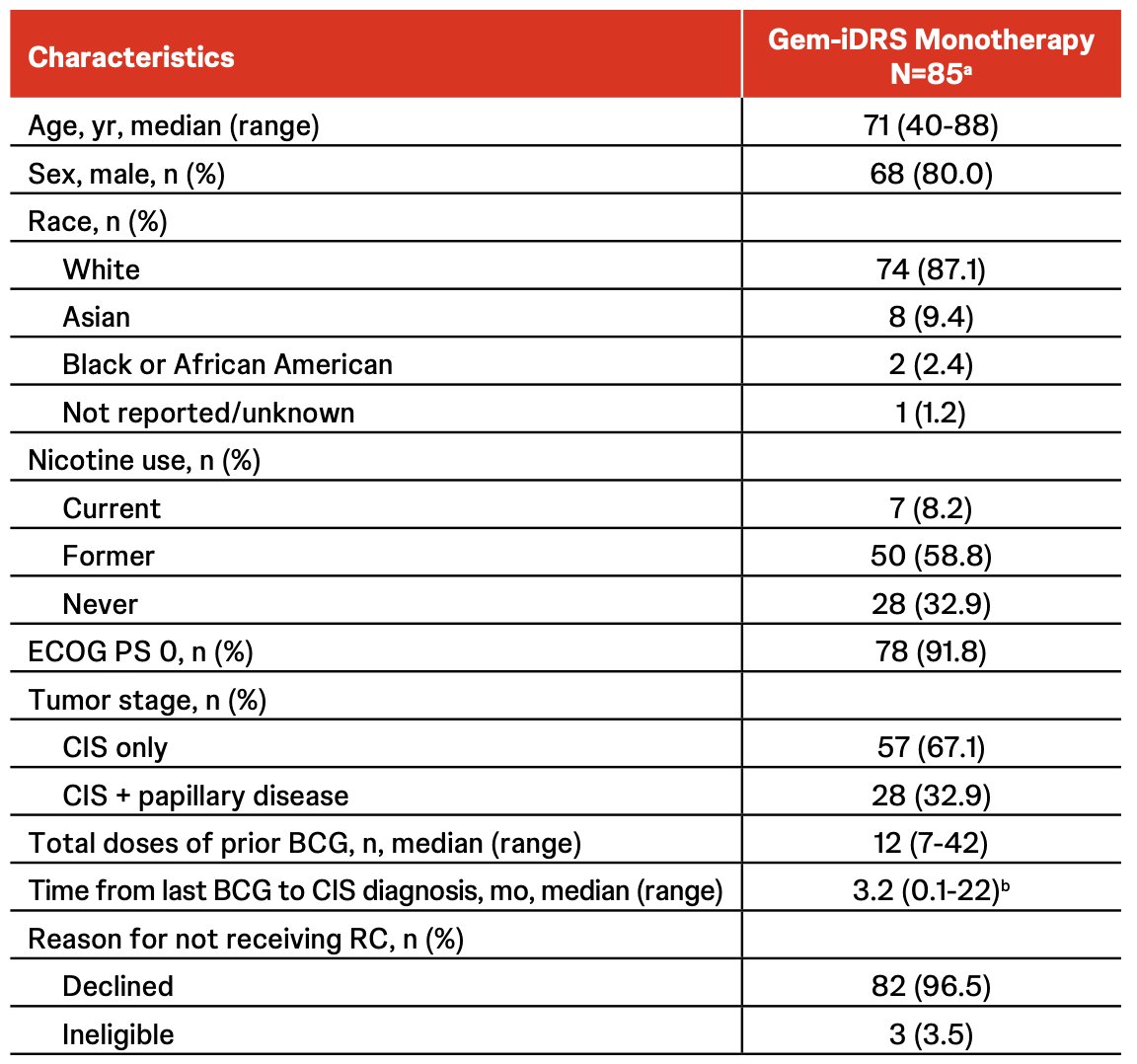
At the data cutoff of March 31, 2025, there were 85 patients who received TAR-200 monotherapy. The median age was 71.0 years (range, 40-88), 80.0% were male, and 32.9% had concurrent papillary disease. The baseline characteristics were as follows in the table below:
The complete response rate was 82.4%, and with a median follow-up of 20.2 months (range: 2-48):
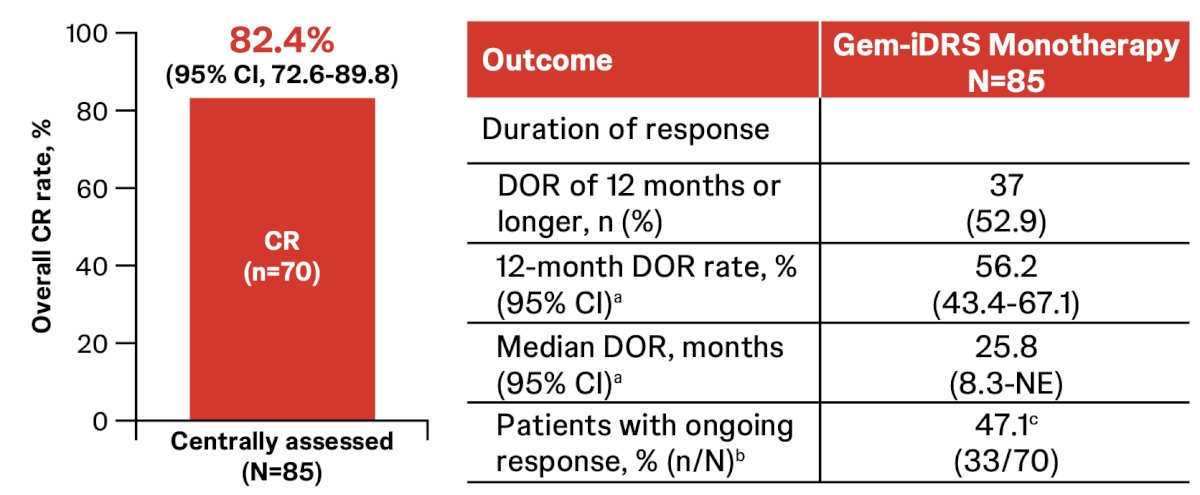
There were 37/70 responders (52.9%) that had a duration of response of ≥12 months, with 37 patients that remained in complete response at the data cutoff: 33 (47.1%) with ongoing responses, and 4 permanently censored. Disease persistence, progression, or recurrence occurred in 41/85 patients (48.2%; of whom 30 were responders), the majority as persistence or recurrence of high-risk non-muscle invasive bladder cancer (CIS/Ta/T1):
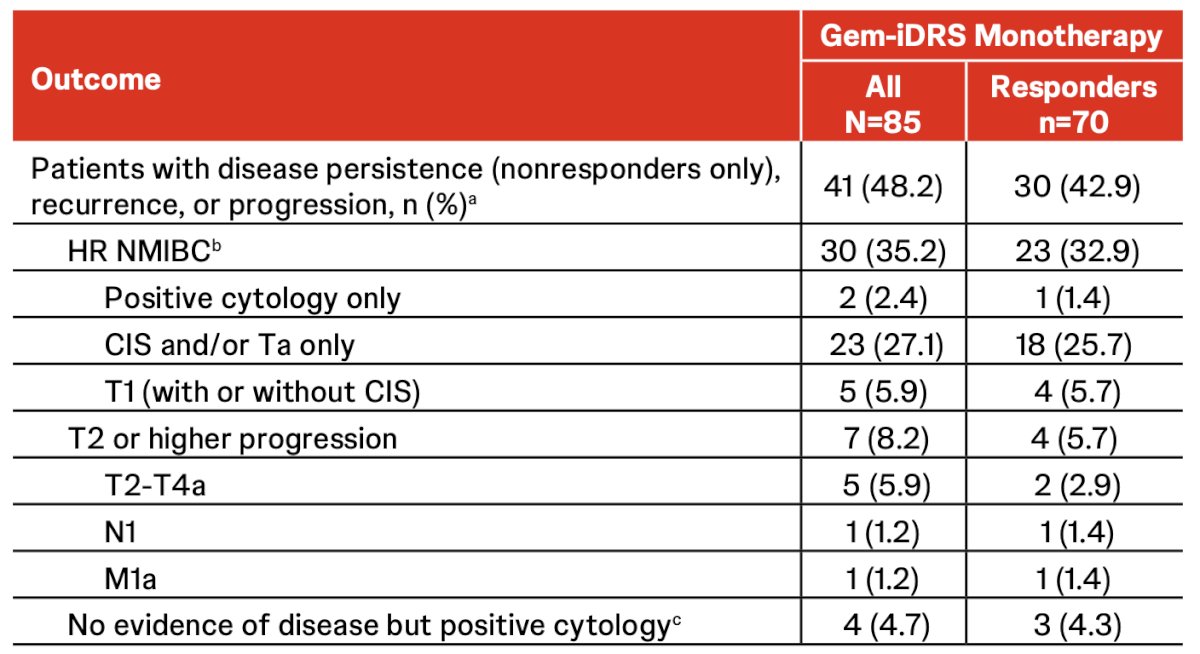
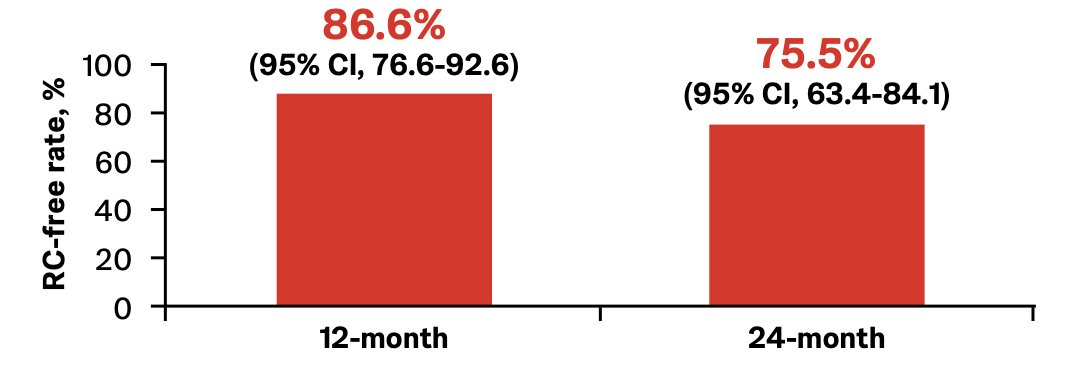
Progression to T2 or higher disease (any N+/M+) was observed in 7 of 85 patients (8.2%), including 1 with metastatic disease, and 5 patients (5.9%) who had disease progression within 1 year and 2 (2.4%) after 1 year. There was no observed difference in progression rates based on baseline stage (CIS +/- Ta versus T1). There were 7 deaths (unrelated to treatment), and 18/85 patients (21.2%) had radical cystectomy, of which 12 (14.1%) were responders. The median time to cystectomy was not estimable, and the estimated 12- and 24-month radical cystectomy free rates were 86.6% (95% CI 76.6-92.6) and 75.5% (95% CI 63.4-84.1), respectively:
There were 15 of 18 patients who underwent radical cystectomy who had TNM staging done locally by the investigator, and the majority were classified as TIS/CIS:

Dr. Murray concluded her presentation discussing characterization of recurrence, progression, and time to cystectomy among patients undergoing gemcitabine intravesicle system monotherapy in BCG-unresponsive high-risk non-muscle invasive bladder cancer with the following take-home points:
- Recurrence and progression data support the gemcitabine intravesicle system monotherapy, which was recently granted FDA approval, as a novel treatment option for patients with BCG-unresponsive CIS with or without papillary disease
- Gemcitabine intravesicle system monotherapy is associated with a high complete response rate and durable responses, minimal risk of disease progression to a more advanced (≥T2) disease stage, and potential delay to radical cystectomy
- The low rate of radical cystectomy in cohort 2 of SunRISe-1 highlights that gemcitabine intravesicle system treatment may result in a potential delay to radical cystectomy
- These results compare favorably with standard of care progression rates of ~20% and support TAR-200 as a novel bladder-sparing treatment for patients with BCG-unresponsive CIS ± papillary disease
Presented by: Katie Murray, DO, MS, FACS, Urologic Oncologist, Department of Urology, NYU Grossman School of Medicine, Chief of Urology Service, Bellevue Hospital Center, NYU Langone Health, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 Southeastern Section of the American Urological Association (SESAUA) Annual Meeting, San Juan, PR, Wed, Mar 18 – Sat, Mar 21, 2026.
Related Content:
SES AUA 2026: Physician Experiences with the Gemcitabine Intravesical System in High Risk NMIBC: A Qualitative Study of SunRISe Trial Investigators
Phase III SunRISe-2 Trial Compares Gem-iDRS and Cetrelimab to Chemoradiation for MIBC Bladder Preservation - Andrea Necchi