(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between September 17th and 21st was host to the session Mini oral session: GU tumours, prostate, penile and testis. Dr. Pasquale Rescigno was the invited Discussant for abstracts 2348MO and 2385MO.
2384MO - First interim efficacy analysis of the Phase 1/2 PETRANHA trial of saruparib + androgen receptor pathway inhibitors (ARPI) in patients (pts) with metastatic prostate cancerDr. Rescigno began by highlighting that three phase III trials: PROpel, TALAPRO-2, and MAGNITUDE have now evaluated the combination of androgen receptor pathway inhibitors (ARPIs) with PARP inhibitors (PARPi) in patients with metastatic castration-resistant prostate cancer (mCRPC).1-3 Each study incorporated similar design features, testing the efficacy of ARPI plus PARPi versus ARPI plus placebo, with radiographic progression-free survival (rPFS) as the primary endpoint, as illustrated below.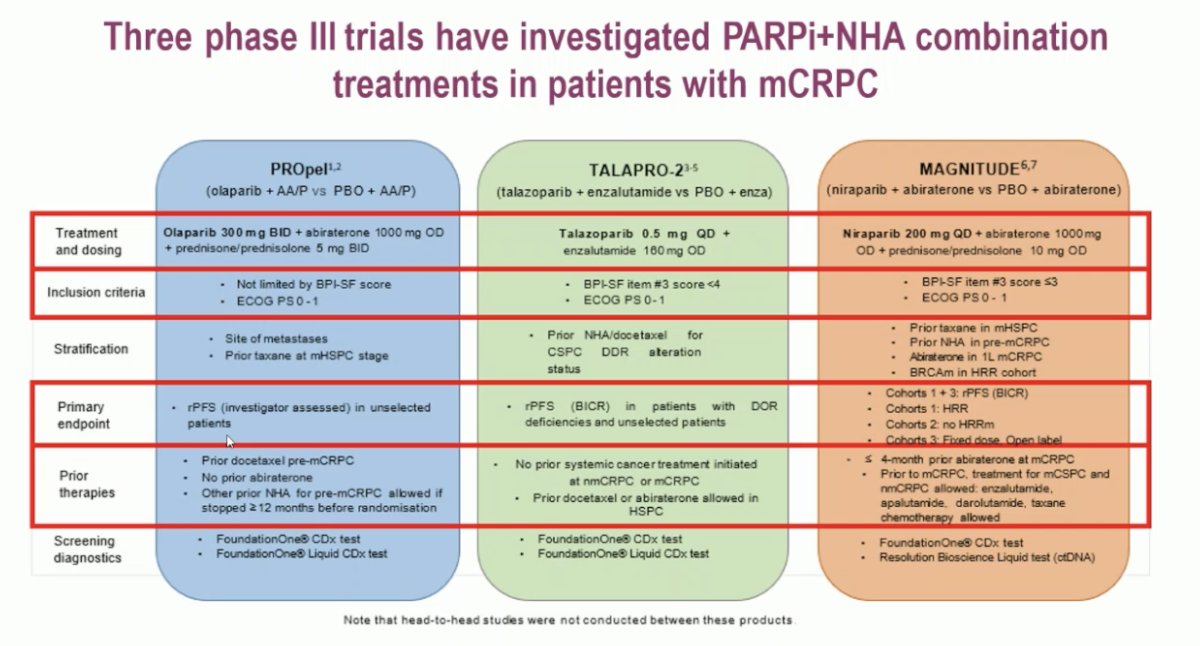
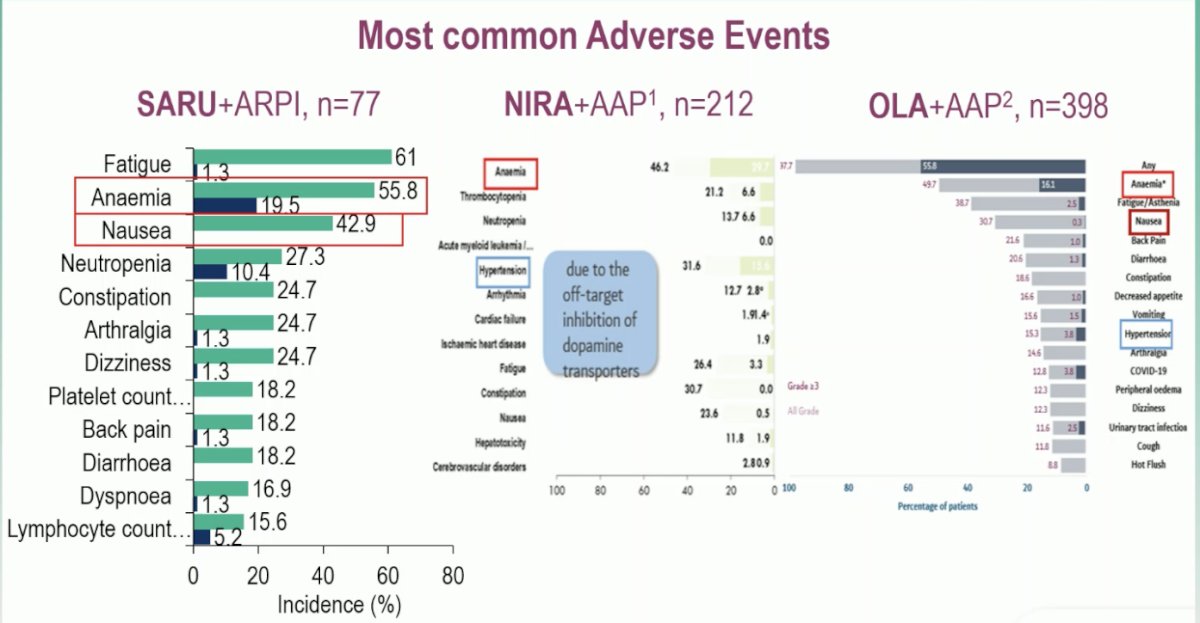
Dr. Rescigno noted that saruparib, being a more selective PARP inhibitor, is theoretically associated with lower off-target toxicity compared to other agents in its class. However, anemia remains the most prominent and dose-limiting adverse event observed across studies, consistent with the class effect of PARPi. Interestingly, hypertension, which was notably common in the MAGNITUDE study with niraparib, was not observed with saruparib, suggesting a more favorable cardiovascular safety profile.
Dr. Rescigno highlighted that treatment discontinuation due to adverse events (AEs) varied across the PARPi + ARPI phase III studies. In PROpel, discontinuation of olaparib occurred in approximately 17%, while in TALAPRO-2, talazoparib discontinuation reached 13%. In MAGNITUDE, niraparib showed similar rates of dose interruptions and reductions, underscoring the need for careful toxicity management. Notably, in the PETRANHA study, discontinuation rates for saruparib were slightly lower, 10.4% for saruparib and 3.9% for ARPI, suggesting a somewhat more favorable tolerability profile compared with prior PARP inhibitor combinations.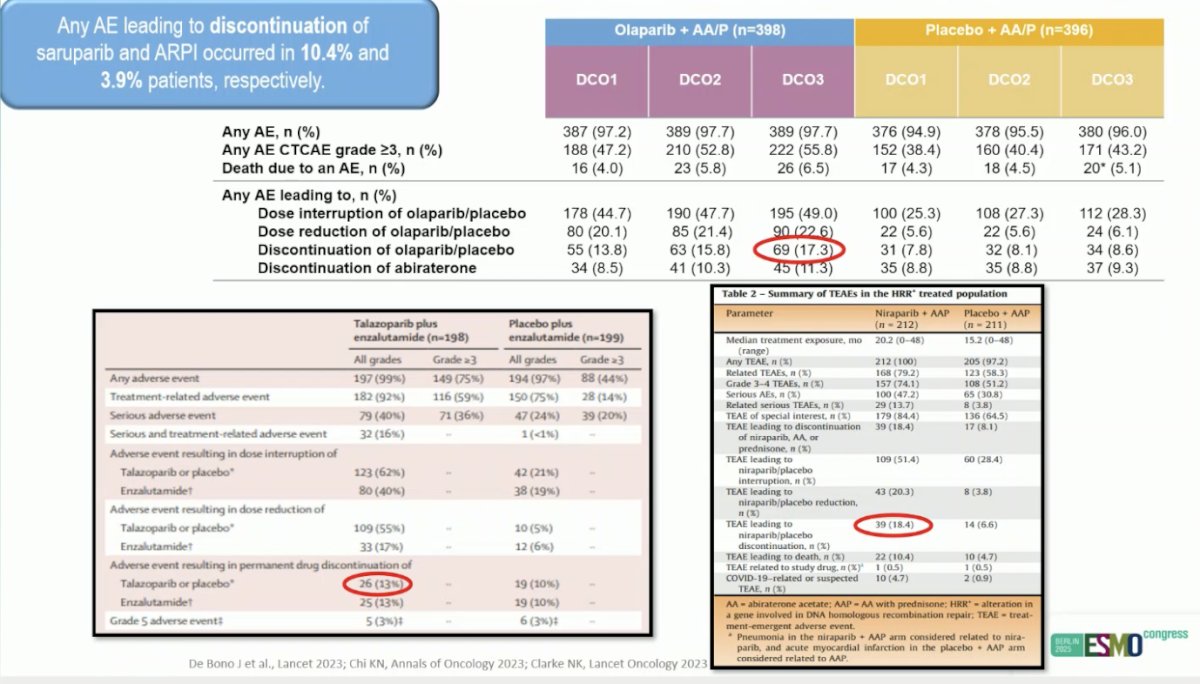
Dr. Rescigno noted that, while cross-trial comparisons should be avoided given the early-phase nature of this study (Phase 2), the best overall response rate (ORR) observed with saruparib plus ARPI was promising 25% among patients with prior ARPI-treated mCRPC, 73.3% in ARPI-naïve mCRPC, and 100% in mCSPC. Interestingly, among the two responders in the pretreated mCRPC cohort, one had a BRCA2 mutation and the other a CDK12 alteration, suggesting that even in later lines, selected molecular subsets may still derive meaningful benefit from PARP inhibition.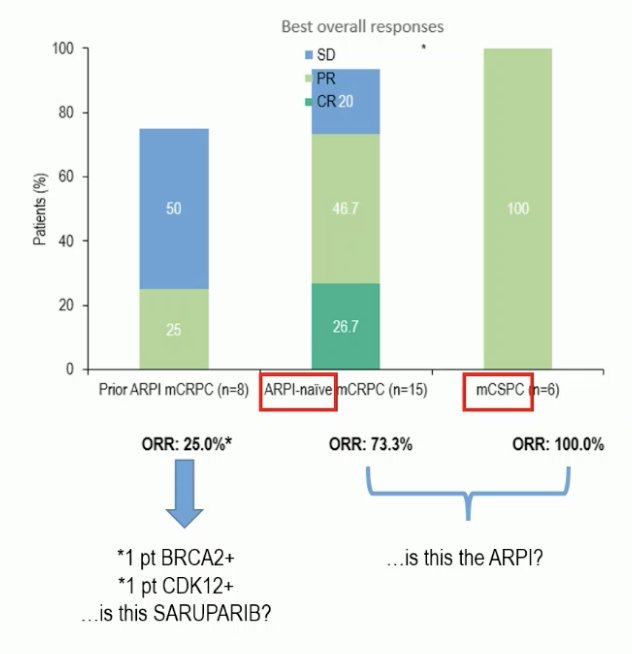
Regarding PSA dynamics, Dr. Rescigno highlighted that among patients treated with saruparib, a high proportion achieved meaningful biochemical responses. Specifically, 83% of patients in the mCSPC cohort reached an undetectable PSA (≤0.2 ng/mL), while PSA-90 responses were observed in 100% of these patients.
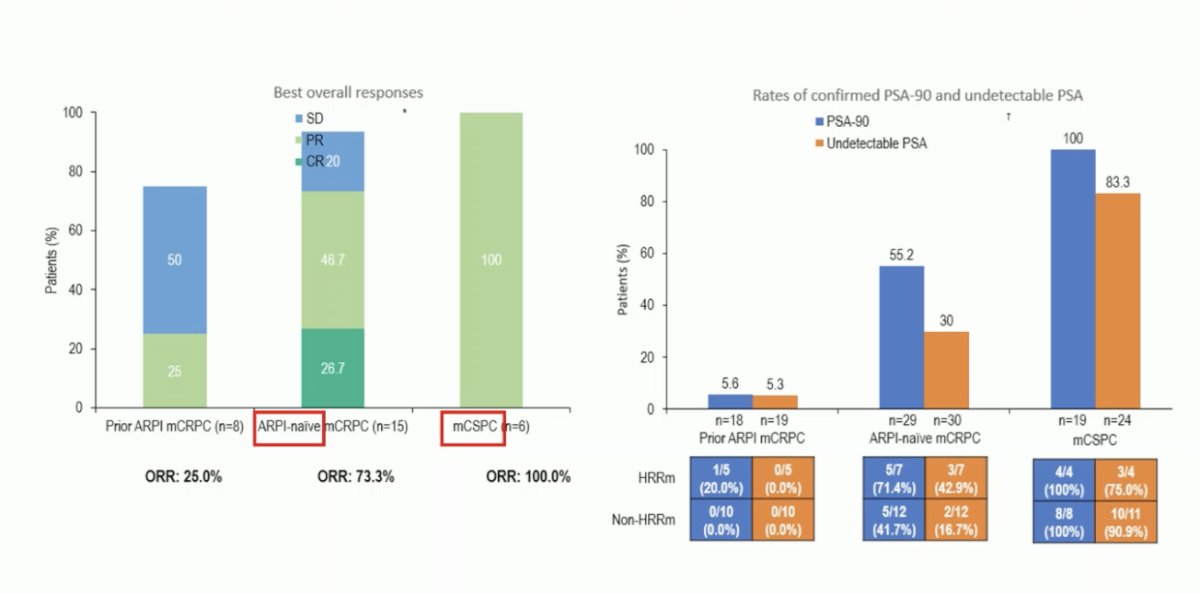
Again, while direct comparisons between phase II and phase III trials are not appropriate, the PETRANHA results provide useful context within the broader mHSPC landscape. In key phase III studies such as ENZAMET, ARCHES, TITAN, LATITUDE, and ARANOTE, PSA90 rates ranged from approximately 68% to 79%, with 58–73% of patients achieving PSA ≤0.2 ng/mL. In contrast, PETRANHA demonstrated PSA-90 and undetectable PSA rates of 100% and 83%, respectively, in the mCSPC cohort, suggesting strong biochemical activity.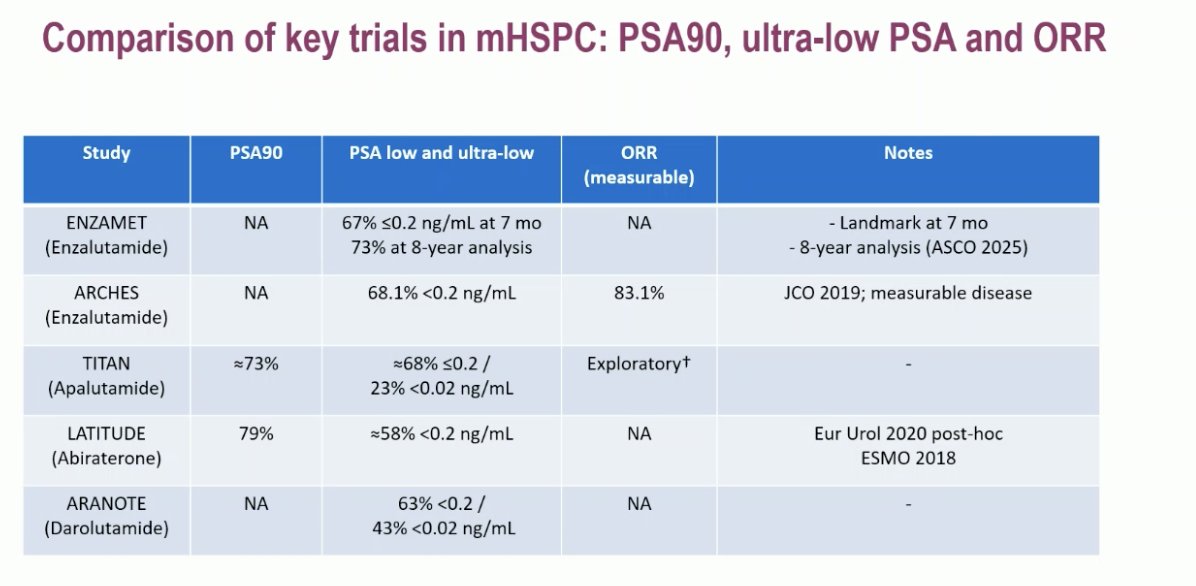
Dr. Rescigno concluded this discussion of the PETRANHA study with the following key messages:
- Saruparib’s safety with ARPIs looks broadly in line with other PARP inhibitors, and early signals suggest a lower treatment-discontinuation rate—but this needs confirmation in larger datasets.
- Efficacy remains preliminary; current data are encouraging but not definitive.
- The phase 3 EvoPAR-Prostate01 trial (NCT06120491) is ongoing, testing saruparib + ARPI versus ARPI + placebo in mHSPC. An open question for the field is whether single-agent PARP inhibition should also be evaluated in BRCA1/2-mutated mHSPC.
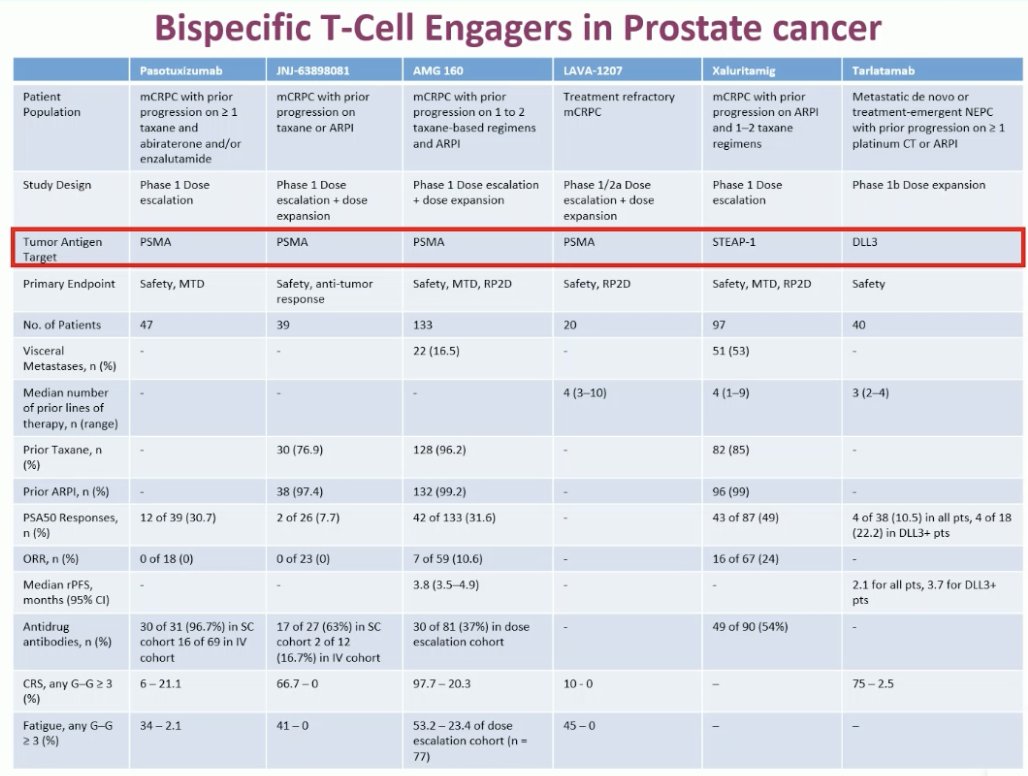
Pasritamig is a first-in-class bispecific T-cell engager antibody that simultaneously binds to CD3 receptor complexes on T cells and to KLK2 on tumor cells, redirecting T-cell cytotoxicity toward KLK2-expressing prostate cancer cells. In the phase I JCO-published study, different dosing schedules were evaluated, and patients receiving the 300 mg IV every 6 weeks regimen tended to remain on treatment longer compared to those on the every-3-weeks schedule.4 This suggests a potentially more tolerable and sustainable dosing approach, supporting further investigation of this novel immunotherapeutic strategy in advanced prostate cancer.
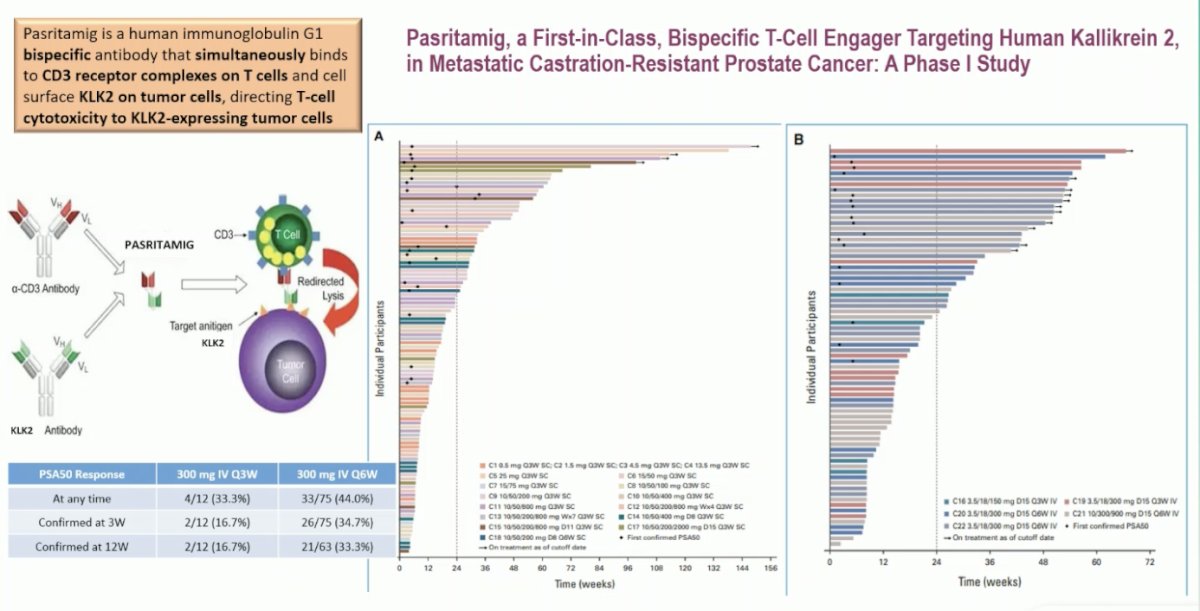
Chronic antigen exposure in cancer leads to T-cell exhaustion a state where T cells lose their proliferative and effector capacity while upregulating inhibitory receptors like PD-1, TIM3, and LAG3. Maintaining longer dosing intervals, such as the Q6W schedule, may help preserve progenitor exhausted T cells (TCF1⁺), which can still renew and regain function upon reactivation. This balance between activation and rest is a finely regulated process involving other immune cells, including dendritic cells in tumor-draining lymph nodes as shown in the figure below.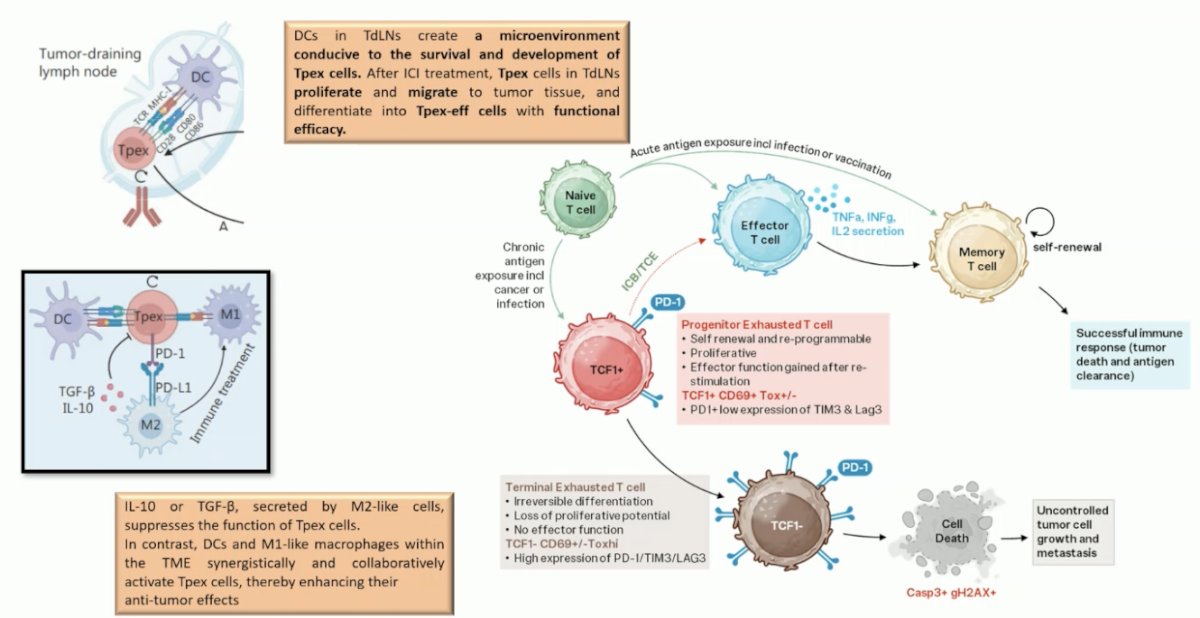
Moreover, these findings carry broader implications beyond bispecific T-cell engagers. They may also inform the optimization of CAR-T cell therapies and cancer vaccines. CAR-T therapy, while highly effective in hematologic malignancies, has shown limited success in solid tumors likely due to T-cell exhaustion. The transcription factor BLIMP1 (encoded by PRDM1) plays a central role in driving CD8⁺ T-cell exhaustion, and modulation of the BLIMP1–TCF-1 axis could enhance CAR-T cell persistence and proliferative capacity, potentially improving outcomes in solid tumors.
Similarly, insights from single-cell RNA sequencing studies in murine models have shown that cancer vaccination induces two major CD8⁺ T-cell subsets within the tumor microenvironment: progenitor-exhausted (TCF-1⁺) and transiently exhausted (CX3CR1⁺ GzmB⁺) populations. Notably, the route of vaccine administration appears to shape this balance intravenous delivery generates a higher proportion of progenitor-exhausted T cells (80%) compared with subcutaneous injection (35%), suggesting a stronger and more durable anti-tumor response. These observations highlight how fine-tuning T-cell exhaustion dynamics could guide the next wave of immunotherapy innovation across multiple platforms.

Presented by: Pasquale Rescigno, MD, Medical Oncologist and Senior Clinical Lecturer at Newcastle University, Newcastle upon Tyne, United Kingdom
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between September 17th and 21st.
References:
- Saad F, Clarke NW, Oya M, Shore N, Procopio G, Guedes JD, Arslan C, Mehra N, Parnis F, Brown E, Schlürmann F, Joung JY, Sugimoto M, Sartor O, Liu YZ, Poehlein C, Barker L, Del Rosario PM, Armstrong AJ. Olaparib plus abiraterone versus placebo plus abiraterone in metastatic castration-resistant prostate cancer (PROpel): final prespecified overall survival results of a randomised, double-blind, phase 3 trial. Lancet Oncol. 2023 Oct;24(10):1094-1108. doi: 10.1016/S1470-2045(23)00382-0. Epub 2023 Sep 12. Erratum in: Lancet Oncol. 2024 May;25(5):e180. doi: 10.1016/S1470-2045(24)00209-2. PMID: 37714168.
- Agarwal N, Azad AA, Carles J, Fay AP, Matsubara N, Szczylik C, De Giorgi U, Young Joung J, Fong PCC, Voog E, Jones RJ, Shore ND, Saad F, Dunshee C, Zschäbitz S, Oldenburg J, Lin X, Healy CG, Kalac M, Kennedy D, Fizazi K. Talazoparib plus enzalutamide in men with metastatic castration-resistant prostate cancer: final overall survival results from the randomised, placebo-controlled, phase 3 TALAPRO-2 trial. Lancet. 2025 Aug 2;406(10502):447-460. doi: 10.1016/S0140-6736(25)00684-1. Epub 2025 Jul 16. PMID: 40683290.
- Chi KN, Castro E, Attard G, Smith MR, Sandhu S, Efstathiou E, Roubaud G, Small EJ, de Santana Gomes AP, Rathkopf DE, Saad M, Gurney H, Jung W, Kim W, Dibaj S, Wu D, Zhang J, Lopez-Gitlitz A, Francis P, Olmos D. Niraparib and Abiraterone Acetate plus Prednisone in Metastatic Castration-resistant Prostate Cancer: Final Overall Survival Analysis for the Phase 3 MAGNITUDE Trial. Eur Urol Oncol. 2025 Aug;8(4):986-998. doi: 10.1016/j.euo.2025.04.012. Epub 2025 May 5. PMID: 40328571.
- Stein MN, Vinceneux A, Robbrecht D, Doger B, Autio KA, Schweizer MT, Calvo E, Medina L, Van Dongen M, Deville JL, Bernard-Tessier A, Ghosh D, Shotts K, Shen F, Jaiprasart P, Chaudhary R, Wu S, Cartee L, Schnepp R, Gaut D, Lauring J, Wang SC, Villalobos VM, Baldini C. Pasritamig, a First-in-Class, Bispecific T-Cell Engager Targeting Human Kallikrein 2, in Metastatic Castration-Resistant Prostate Cancer: A Phase I Study. J Clin Oncol. 2025 Aug;43(22):2515-2526. doi: 10.1200/JCO-25-00678. Epub 2025 Jun 1. PMID: 40450573; PMCID: PMC12288886.