(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to the session Mini oral session: GU tumours, prostate, penile and testis. Dr. Karen Autio presented the abstract 2385MO - Translational analyses of T-cell phenotypes and their association with clinical efficacy in the first-in-human (FIH) trial of JNJ-78278343 (pasritamig) in metastatic castration-resistant prostate cancer (mCRPC).
Dr. Autio began by highlighting that Human kallikrein-related peptidase 2 (KLK2) expression is highly specific to prostate adenocarcinoma and remains consistent throughout all disease stages.1 She presented data from the first-in-human (FIH) phase I trial of pasritamig in mCRPC, which included 21 dose-escalation cohorts exploring both subcutaneous (SC) and intravenous (IV) routes.
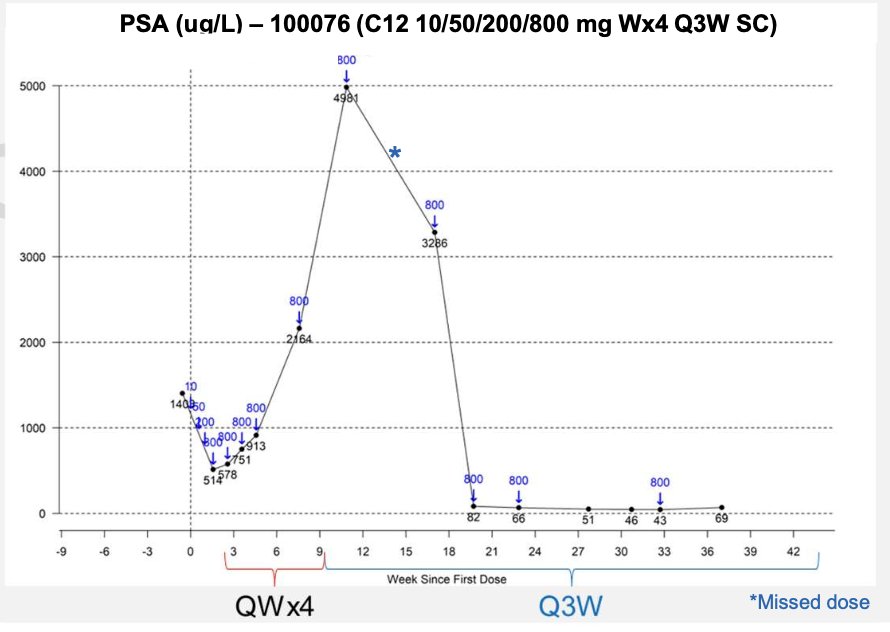
The trial employed a step-up dosing strategy to mitigate cytokine release syndrome, while IV dosing was selected to enhance exposure and reduce injection-site reactions. Different dosing intervals were evaluated, with Q6W identified as optimal for maintaining therapeutic concentrations and minimizing T-cell exhaustion. The recommended phase II dose (RP2D) was defined as SU1 3.5 mg on day 1, SU2 18 mg on day 8, TD 300 mg on day 15, followed by 300 mg every six weeks (all IV). Interestingly, PSA levels initially increased during Q1W SC dosing but declined when the dosing interval was extended to Q3W in a subset of patients, as shown in the figure below.
Dr. Autio discussed translational findings exploring why extending pasritamig dosing from every 3 weeks (Q3W) to every 6 weeks (Q6W) improved response rates. The hypothesis proposed that longer dosing intervals reduce T-cell terminal exhaustion and activation-induced T-cell death, thereby enhancing antitumor activity.
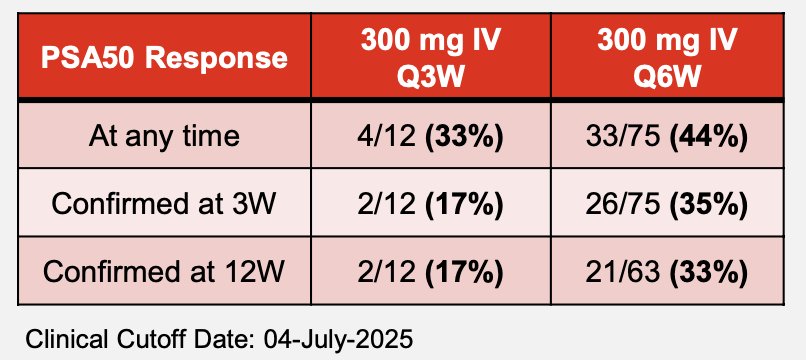
In the trial, PSA50 responses were observed more frequently with the 300 mg IV Q6W schedule compared to Q3W 44% versus 33% overall, and 35% versus 17% when confirmed at 3 weeks. These results suggest that less frequent dosing may help preserve effector and memory T-cell function, supporting a more sustained and effective immune response
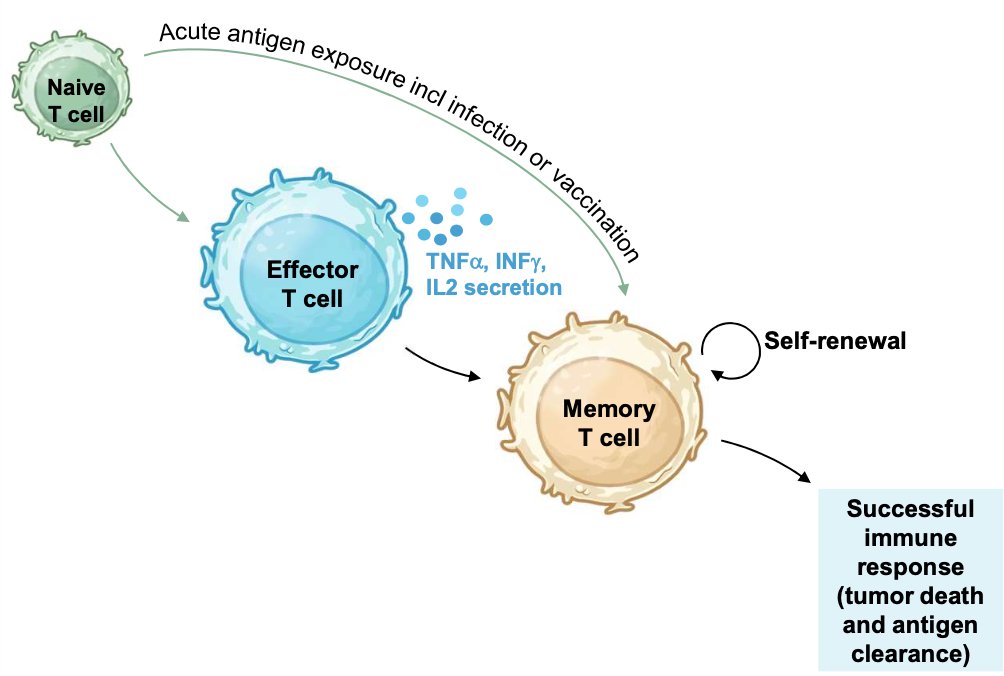
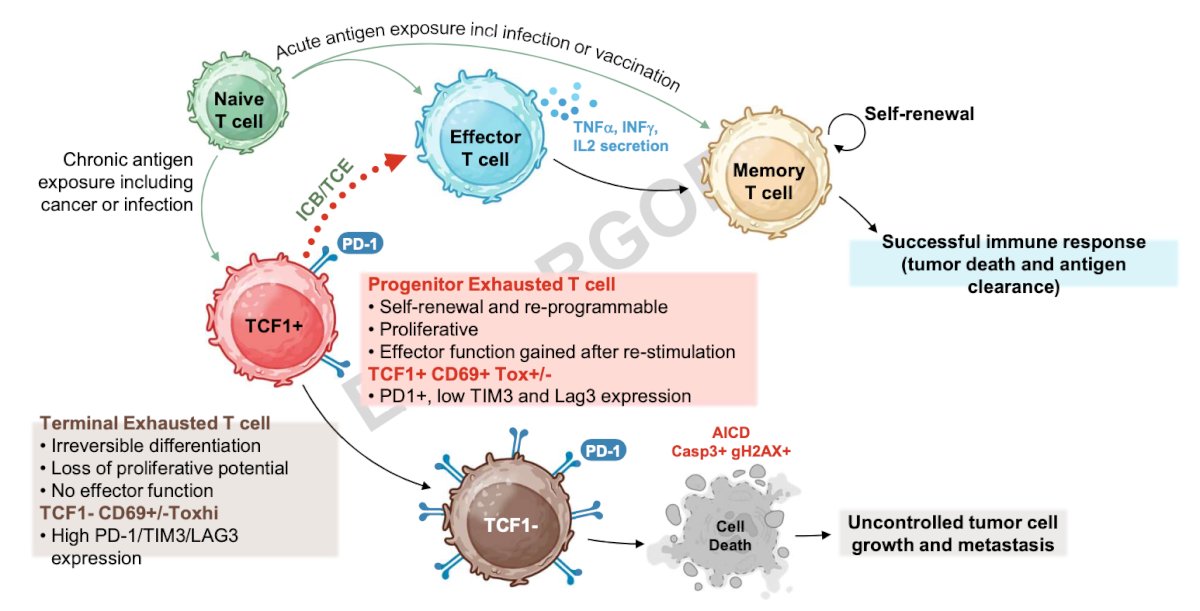
Moreover, Dr. Autio explained that dosing frequency directly influences T-cell exhaustion dynamics. Chronic antigen exposure, as seen in cancer, drives T cells toward a terminally exhausted state characterized by irreversible differentiation, loss of proliferative potential, lack of effector function, and high expression of exhaustion markers (PD-1, TIM3, LAG3). In contrast, maintaining appropriate dosing intervals—such as the Q6W schedule—helps preserve a pool of progenitor exhausted T cells (TCF1⁺ CD69⁺ Tox⁺/⁻), which retain self-renewal capacity and the ability to regain effector function upon re-stimulation. With continued exposure, these TCF1⁺ progenitor cells eventually transition into terminally exhausted T cells (TCF1⁻ CD69⁺/⁻ Tox^hi), marking irreversible loss of proliferative and functional potential.
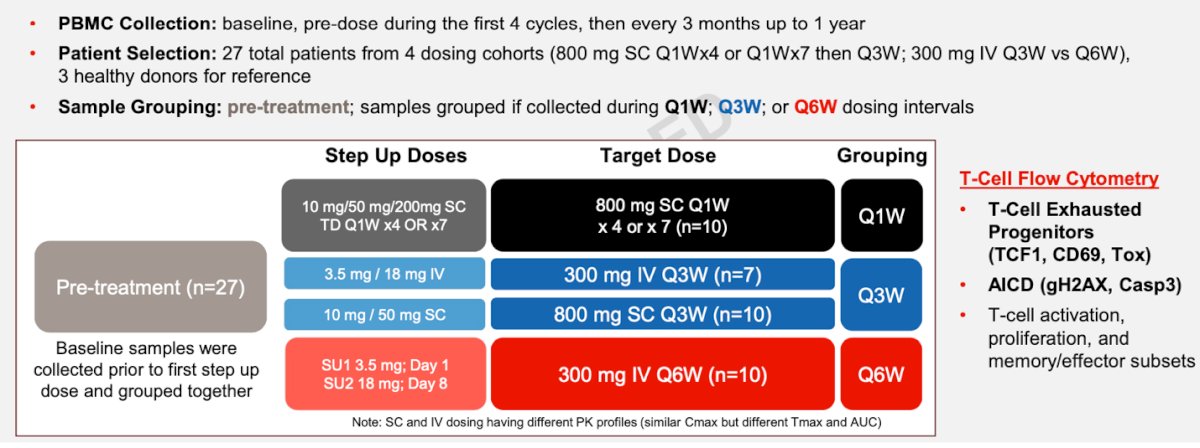
For this analysis, peripheral blood mononuclear cells (PBMCs) were collected at baseline, before each of the first four treatment cycles, and then every three months for up to one year. A total of 27 patients from four dosing cohorts including both SC and IV schedules (800 mg SC Q1W or Q3W; 300 mg IV Q3W or Q6W) were included, alongside three healthy donors for reference. Samples were grouped according to dosing interval (Q1W, Q3W, or Q6W). Flow cytometry evaluated T-cell exhaustion progenitors (TCF1, CD69, Tox), activation-induced cell death markers (gH2AX, Casp3), and T-cell activation, proliferation, and memory/effector subsets to characterize the immunologic effects of different dosing regimens as illustrated below.
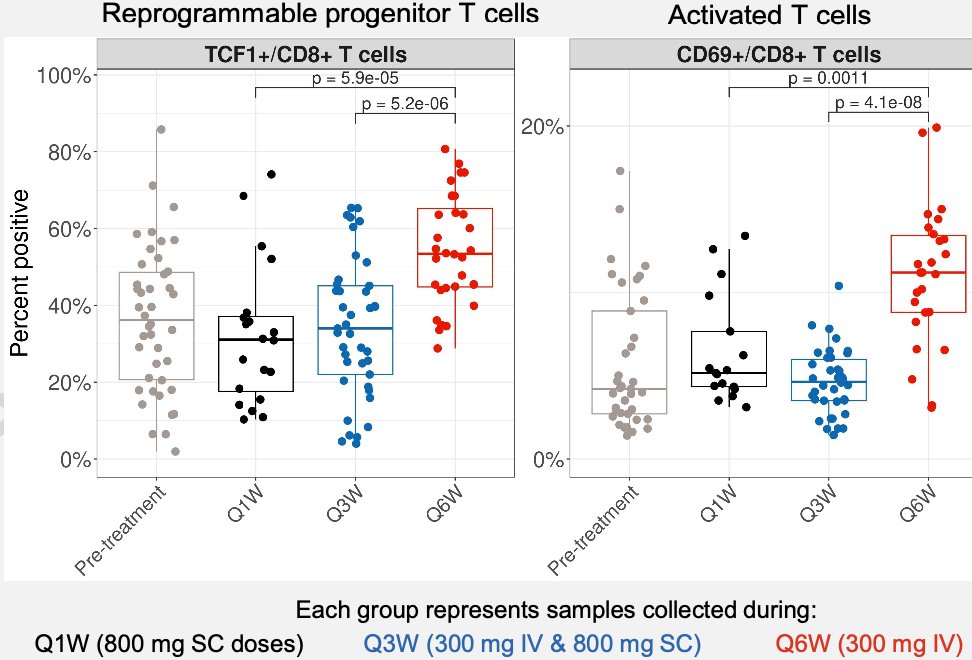
Lastly, Dr. Autio reported that less frequent Q6W dosing appeared to promote more productive T-cell responses by reducing T-cell exhaustion. Flow cytometry analyses showed that Q6W dosing preserved higher proportions of TCF1+/CD8+ progenitor T cells, which remain reprogrammable and capable of effector reactivation, compared to Q1W and Q3W schedules (p < 0.001). Similarly, CD69+/CD8+ activated T cells, an early activation subset associated with migration from lymphoid tissue into circulation, were significantly enriched with Q6W dosing.
Dr Autio concluded their presentation with the following key points:
- Biomarker analyses of PBMCs support the proposed mechanism of action of pasritamig and the recommended RP2D (SU1 3.5 mg / SU2 18 mg / 300 mg IV Q6W).
- Increasing the dosing interval from Q1W or Q3W to Q6W mitigates pasritamig-induced overactivation of T cells, T-cell exhaustion, and activation-induced T-cell death (AICD).
- Dosing pasritamig every six weeks maintains the peripheral pool of a re-programmable, stem-like CD8 T-cell population capable of rapidly differentiating into anti-tumor effector T cells.
- As reported at ASCO 2025, the Q6W schedule enables outpatient dosing with a favorable safety profile.
- The key learning of this analysis is that because the mechanism of action of T-cell engagers differs fundamentally from other therapeutic modalities, dose optimization should incorporate both immune parameter and pharmacokinetic analyses.
- Ongoing studies continue to evaluate the association between immune fitness, exhaustion, and clinical response or resistance.
- Pasritamig is now being investigated in the phase 3 KLK2-comPAS trial (NCT04898634)
Presented by: Karen Autio, MD, MSc, Memorial Sloan Kettering Cancer Center, New York, NY, United States of America
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.
Related content: Phase 1 Dosing Strategy and Translational Findings for Investigational Therapy Pasritamig - Karen Autio
Reference: