(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany between October 17th and 21st, 2025 was host to a renal and urothelial carcinoma proffered paper session. Dr. Lisa Pickering discussed the prior three abstract presentations:
- LBA96 - First-line Pembrolizumab-based Regimens for Advanced Clear Cell Renal Cell Carcinoma: KEYMAKER-U03 Substudy 03A
- LBA94 - LenCabo: A Randomized Phase II Multicenter Trial of Lenvatinib plus Everolimus versus Cabozantinib in Patients with Metastatic Clear Cell RCC that Progressed on PD-1 Immune Checkpoint Inhibition
- 2591O - Efficacy of Cabozantinib and Nivolumab in Cluster 1/2 Metastatic Clear Cell Renal Cell Carcinoma: Results from OPTIC RCC, a Phase II Trial of a Novel RNAseq-based Biomarker
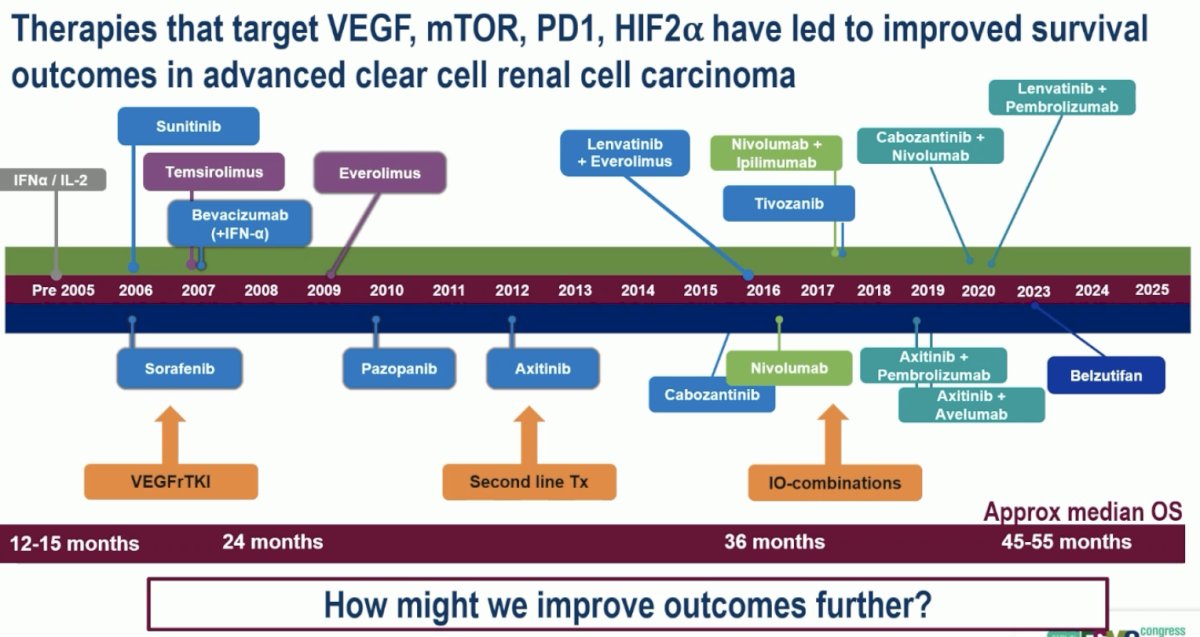
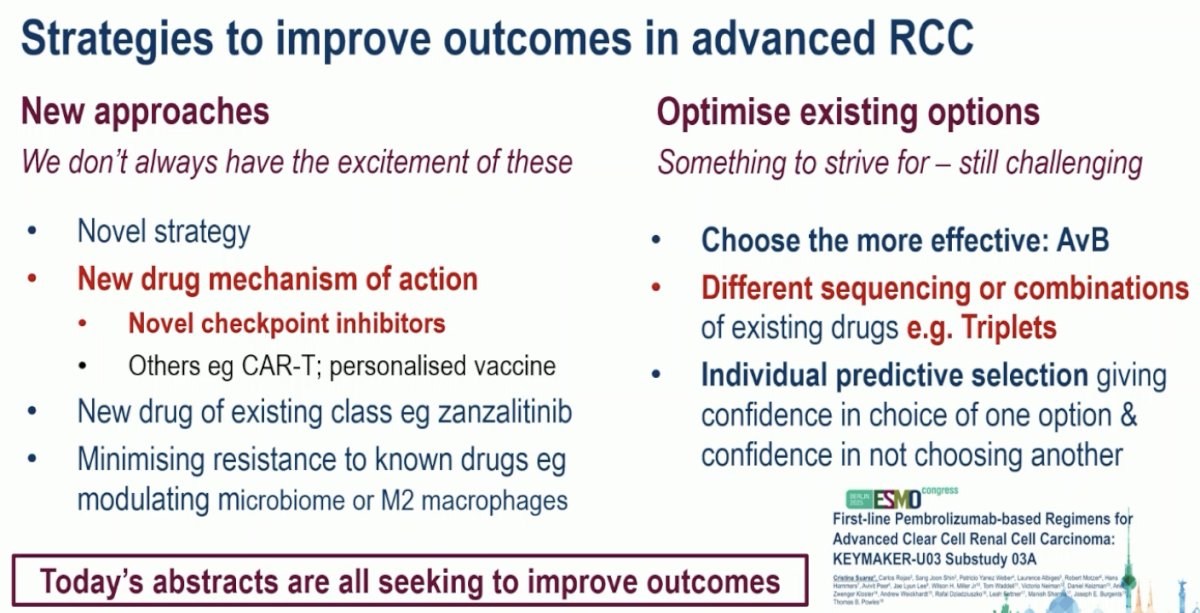
Over the past twenty years, therapies that target VEGF, mTOR, PD1, and HIF2α have been used sequentially or in combination leading to improved survival outcomes in advanced ccRCC.
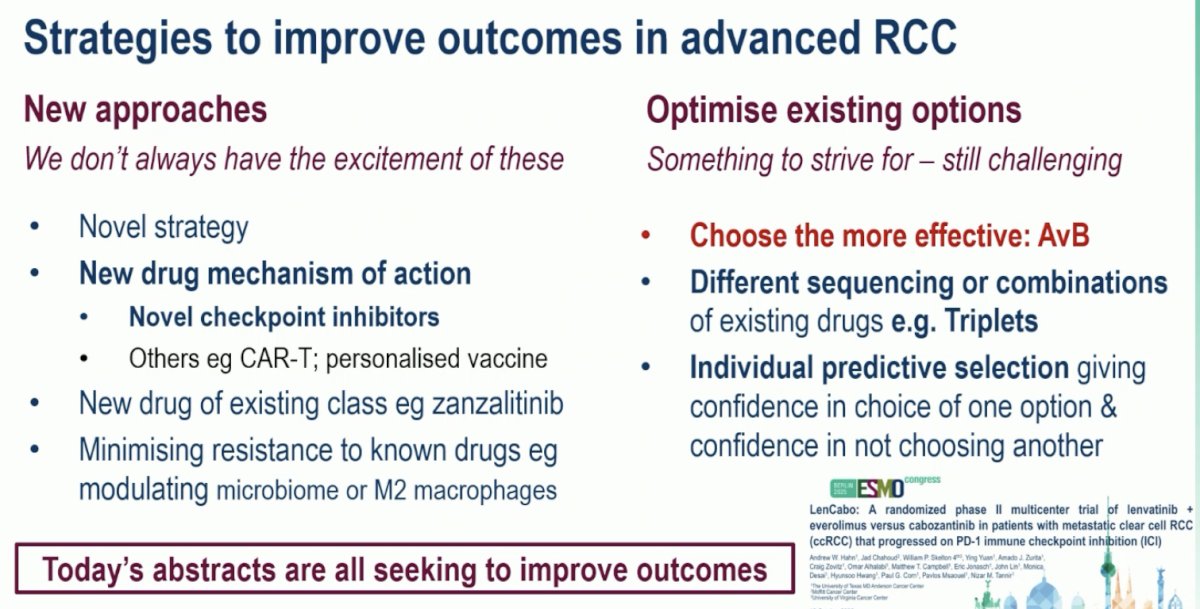
Strategies to further improve outcomes in advanced RCC potentially include using new agents with novel mechanisms of action or optimizing existing options:
Discussing LenCabo first, she noted that this trial addressed a real-life, relevant question for patients who have received an immune checkpoint inhibitor (ICI), but not lenvatinib or cabozantinib in the 1st line setting. These patients are routinely seen in clinics worldwide after progressing on 1st line regimens, including ipilimumab + nivolumab, pembrolizumab + axitinib, and axitinib + avelumab, among other ICI-based regimens. She noted that ~70% of patients in this trial had not received prior VEGF-directed therapy, and that this trial allowed for the inclusion of patients with treated brain metastases, which is clinically relevant.
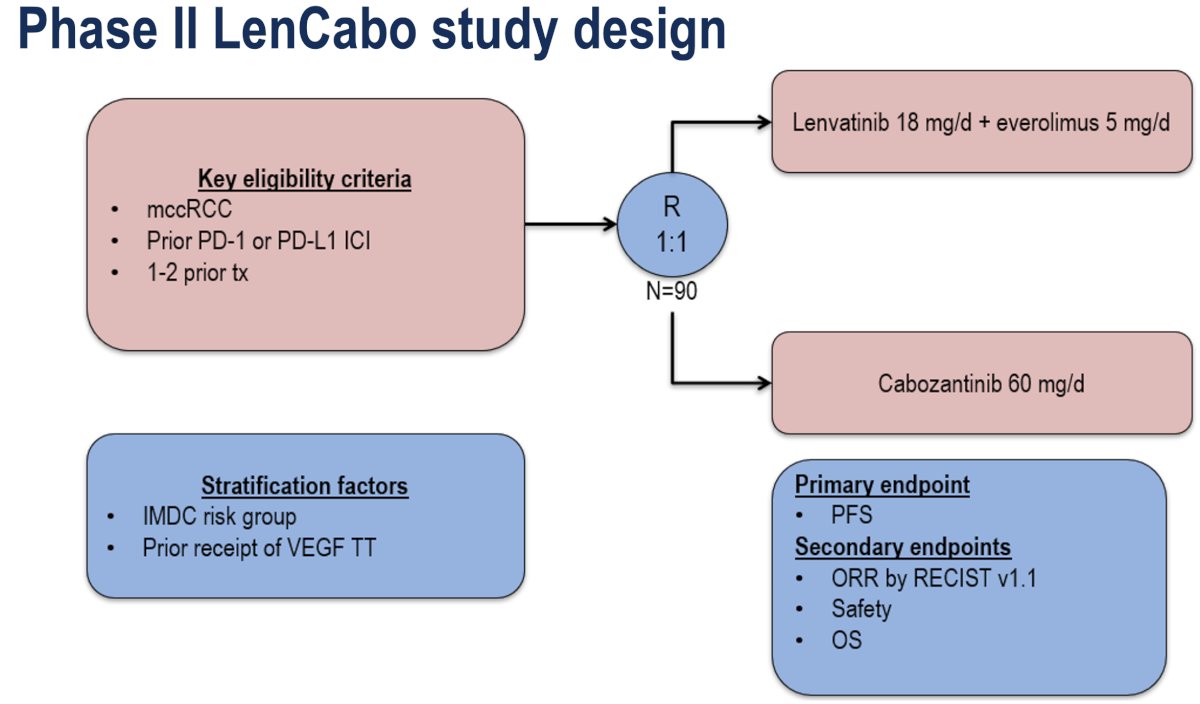
The study design of LenCabo is illustrated below. Patients with metastatic ccRCC who have received 1–2 prior lines of therapy, including an anti-PD-1 or PD-L1 immune checkpoint inhibitor, were randomized 1:1 to:
- Lenvatinib 18 mg daily + everolimus 5 mg daily
- Cabozantinib 60 mg daily
The primary endpoint was progression-free survival (PFS), with key secondary endpoints of objective response rate (ORR), safety, and overall survival (OS).
Patients receiving lenvatinib + everolimus had a 49% relative improvement in PFS (HR: 0.51, 95% CI: 0.29–0.89, p=0.02). Similarly, the ORR was superior in the lenvatinib + everolimus arm (53% versus 39%; OR: 1.87 ,p=0.17). No complete responses were observed.
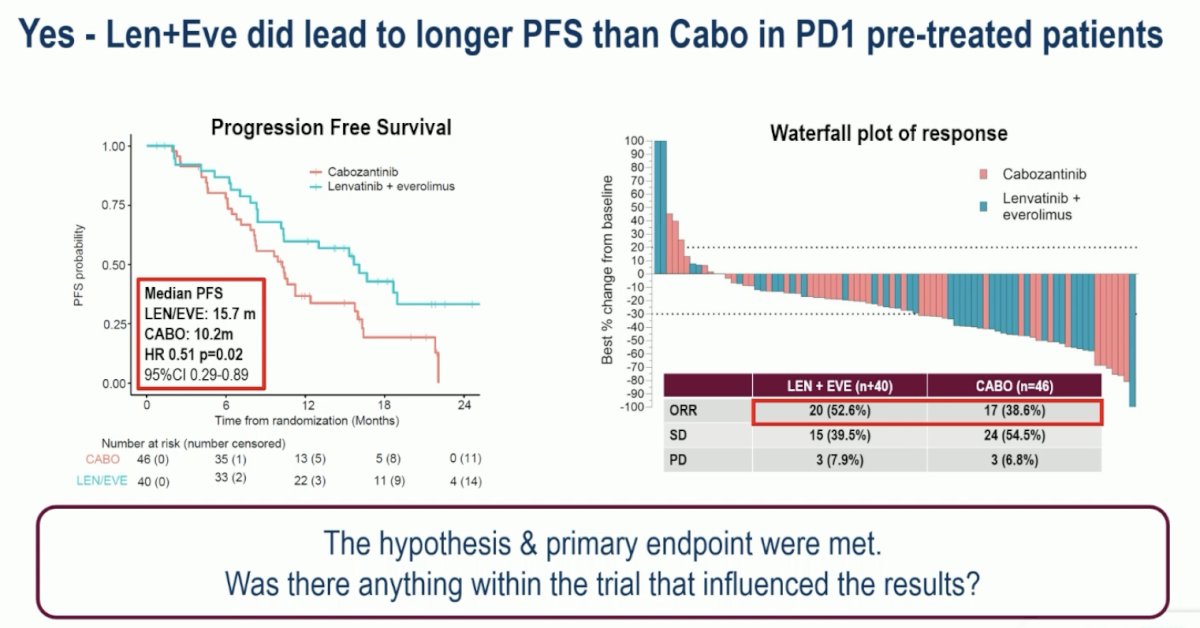
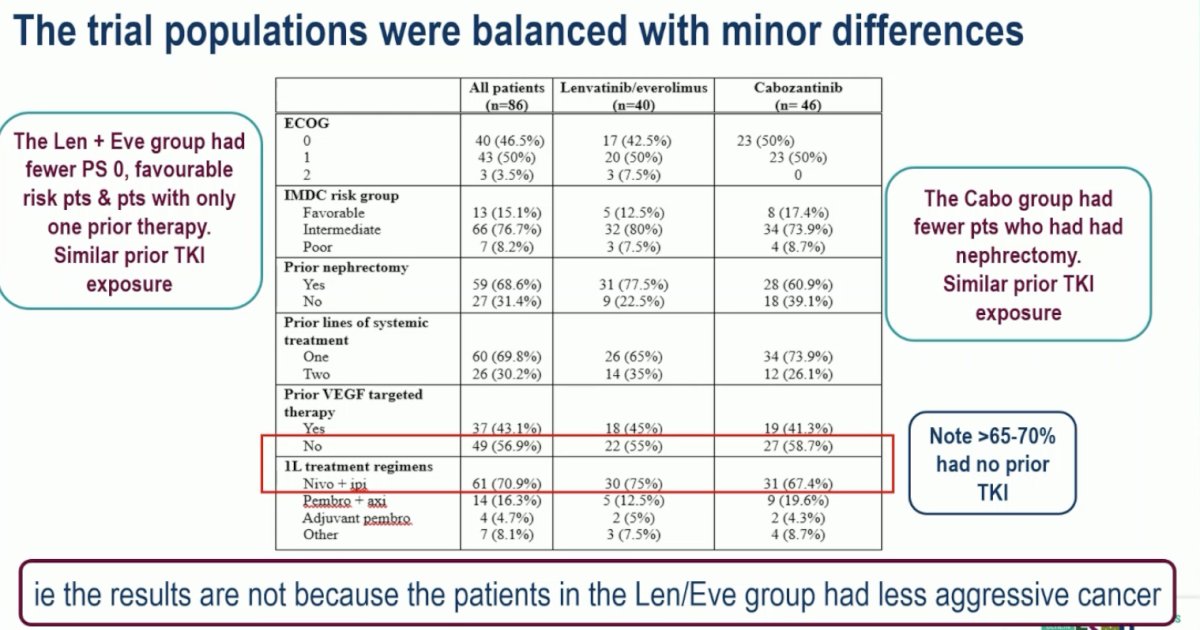
She highlighted that the two study arms were well-balanced for disease characteristics. In other words, the relative improvement in survival outcomes with lenvatinib + everolimus was not due to patients randomized to that arm having more favorable disease characteristics.
How do the efficacy outcomes for lenvatinib + everolimus and cabozantinib in this trial compare to those for the same agents in other trials? While these trials have different designs, populations, and prior therapies received and are, thus, not comparable, a general overview suggests that the ORR and PFS outcomes are broadly in line with prior experiences. Notably, there was a higher incidence of Grade 3-4 toxicity and treatment discontinuation with lenvatinib + everolimus, which is of utmost importance in patients being treated in later line advanced RCC settings.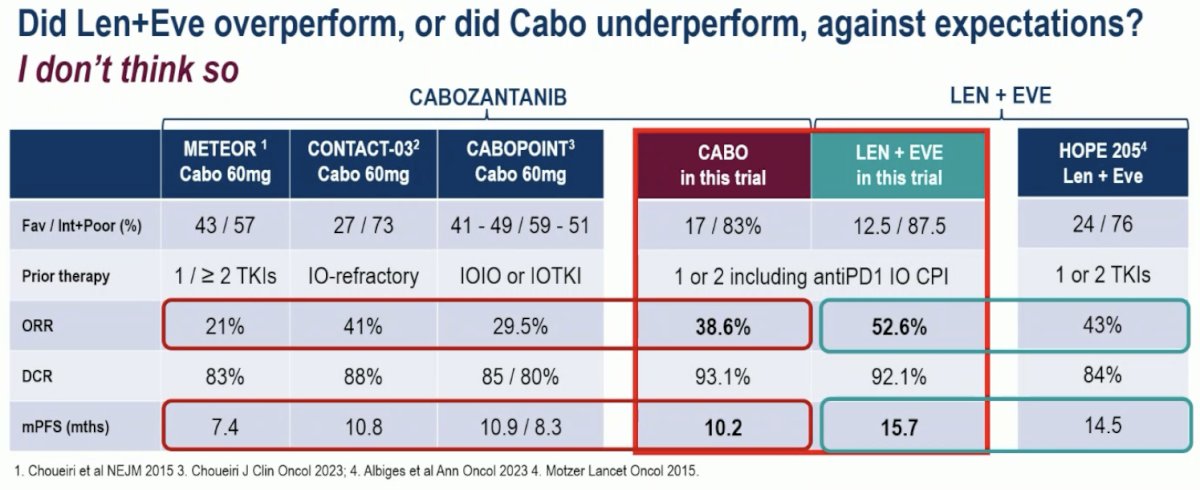
Will this trial change Dr. Pickering’s practice?
- Lenvatinib + everolimus is an active regimen, but its registrational study was a phase II trial, which has led to less uptake in clinical practice
- Cabozantinib is widely used and remains a standard of care option in the 2nd line setting
- Dr. Pickering will continue to use it
- This is a positive phase Il trial
- Although OS data are not yet mature
- This trial demonstrates the efficacy of lenvatinib + everolimus for ICI pre-treated patients with improved PFS & ORR compared with cabozantinib, albeit with higher toxicity
- Is it 'positive enough'? This will depend on the patient, physician, and their shared decision-making process
- We can consider using lenvatinib + everolimus in patients for whom the priority is response and for whom the higher toxicity rate is acceptable
Next, moving on to discuss KEYMAKER-U03 Substudy 03A, Dr. Pickering noted that this trial evaluated drugs with novel mechanisms of action and evaluates novel triplet regimens.
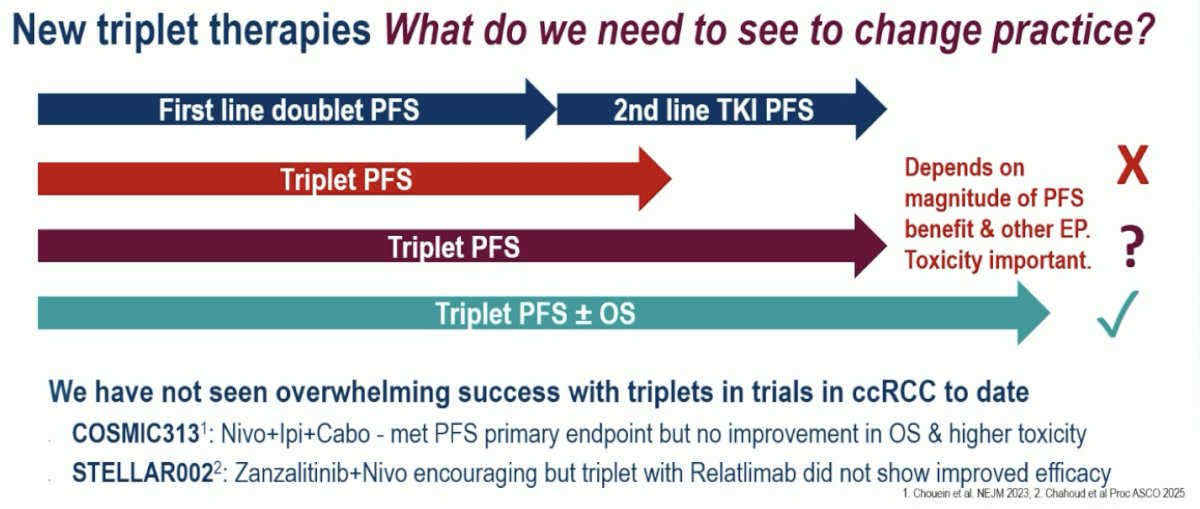
What are we looking for in triplet regimens? Ideally, these regimens should lead to improvements in MFS and OS, benefits which have not yet been observed in trials of triplet therapy (COSMIC313, STELLAR002).1,2
Substudy 03А (NCT04626479) of the umbrella phase 1/2 KEYMAKER-U03 trial was designed to evaluate novel pembrolizumab-based regimens in the first line setting for participants with advanced ccRCC. The study employed an adaptive design in which experimental arms were added and/or inactivated on a rolling basis with a continuous enrolling reference arm. The experimental arms each had a safety lead-in phase of 10 patients (40 total).
The study design of KEYMAKER-U03 Substudy 03A (NCT04626479) is illustrated below.
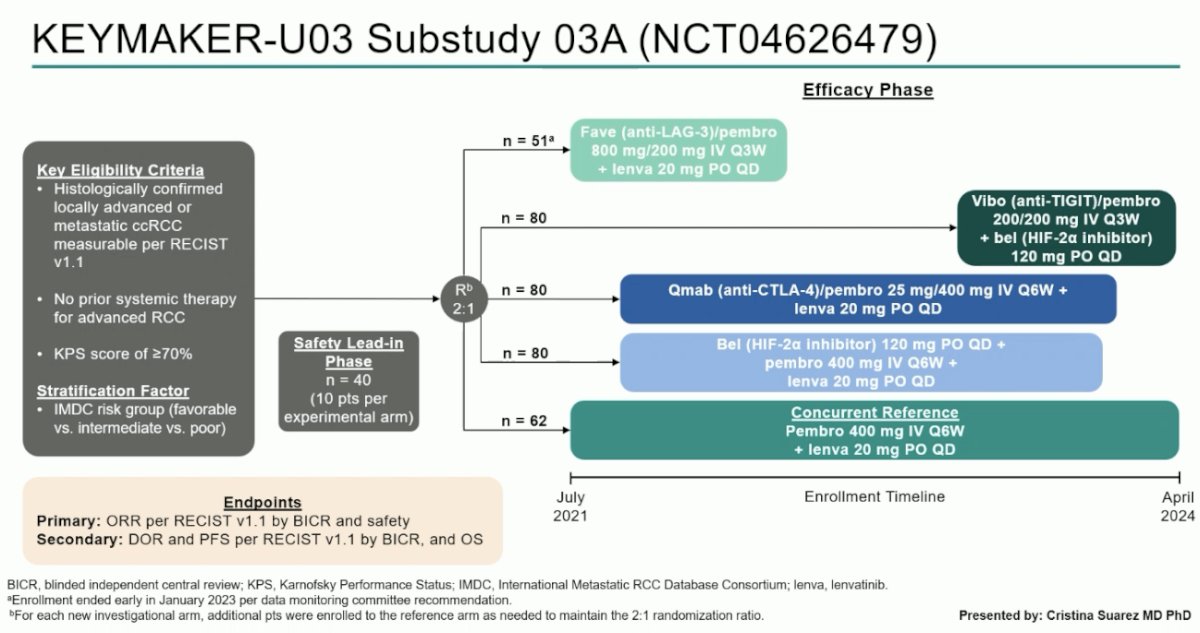
Eligible participants were those with histologically confirmed locally advanced or metastatic ccRCC with no prior systemic therapy for advanced RCC and excellent performance status. The 1st phase of the trial was a safety lead-in with 10 patients per experimental arm.
Following the lead-in phase, patients were randomized 2:1 as follows:
- Reference arm: Pembrolizumab + lenvatinib
- Experimental arms (open for enrollment at varying timepoints)
- Favezelimab (anti-LAG-3) + pembrolizumab + lenvatinib
- Vibostolimab (anti-TIGIT) + pembrolizumab+ belzutifan
- Quavonlimab (anti-CTLA-4) + pembrolizumab + lenvatinib
- Belzutifan + pembrolizumab + lenvatinib
The primary endpoint was ORR and safety outcomes.
The ORR was highest in the reference arm of pembrolizumab + lenvatinib – 81%. The ORRs in the other four arms were as follows:
- Fave (anti-LAG-3) + pembrolizumab + lenvatinib: 63%
- Vibo (anti-TIGIT) + pembrolizumab + belzutifan: 43%
- Qmab (anti-CTLA-4) + pembrolizumab + lenvatinib: 71%
- Belzutifan (HIF-2α inhibitor) + pembrolizumab + lenvatinib: 78%
- Highest complete response (CR) overall: 13%
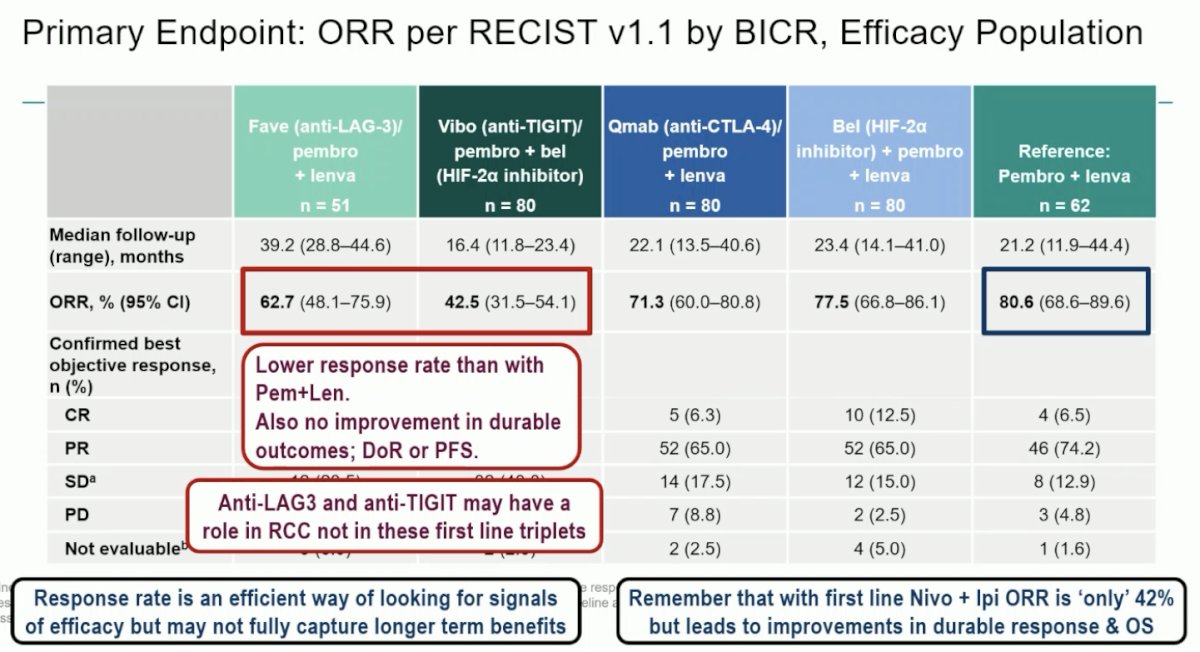
A comparison of efficacy survival outcomes (DOR, PFS, & OS) between the experimental arms including Fave, Vibo, and Qmab and the reference demonstrated no significant differences.
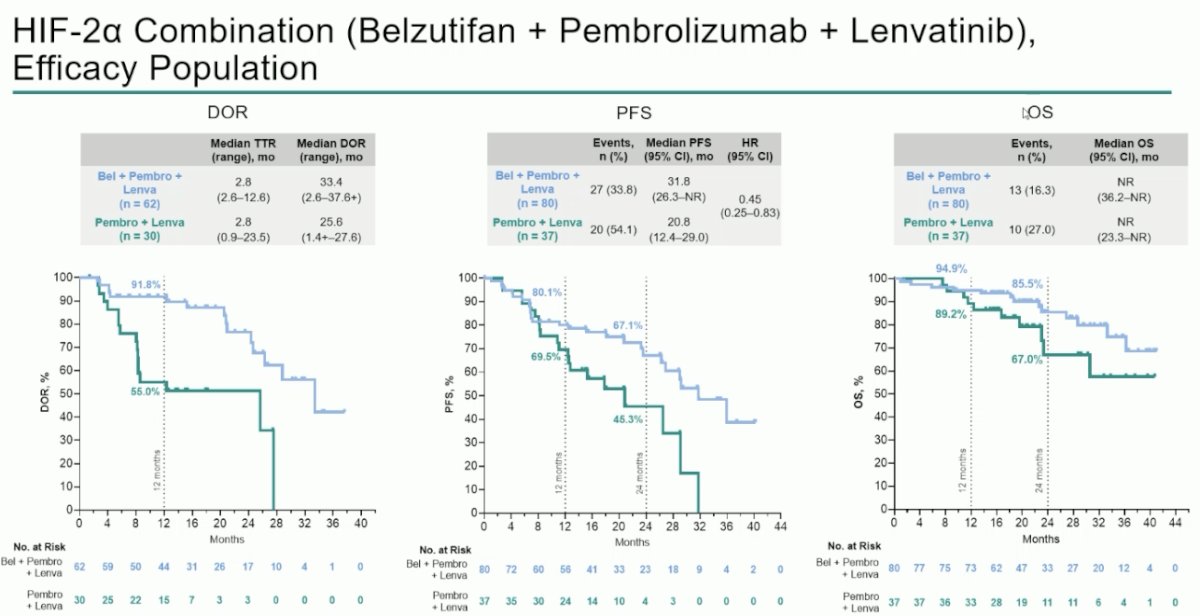
However, in the comparison of the reference arm with the experimental arm of belzutifan + pembrolizumab + lenvatinib, patients in the experimental arm were found to have superior:
- DOR:
- Median: 33.4 vs 25.6 months
- 12 months: 92% vs 55%
- PFS:
- Median: 32 vs 21 months (HR: 0.45, 95% CI: 0.25–0.83)
- 24 months: 67% vs 45%
- OS:
- Median: Not reached in either arm
- 24 months: 86% vs 67%
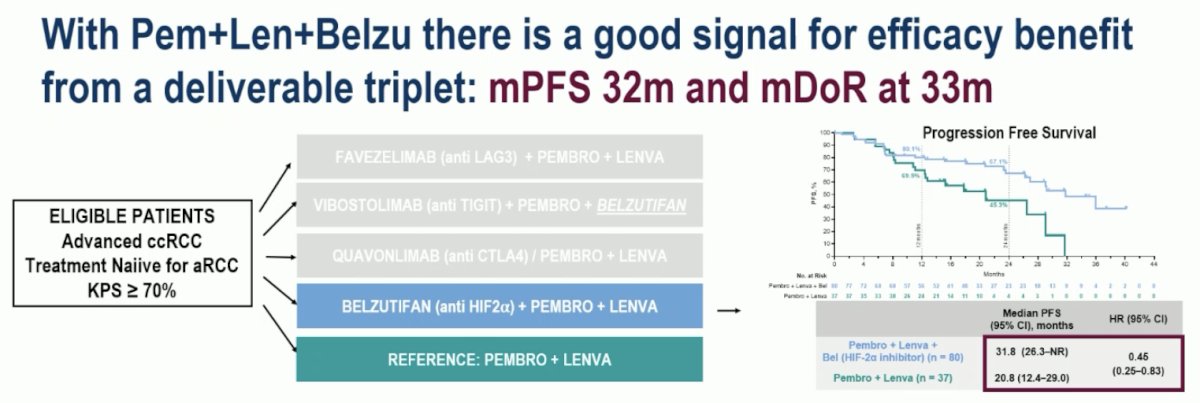
Dr. Pickering commented the following on the combination of belzutifan + pembrolizumab + lenvatinib:
- Her personal thoughts: Encouraging signs for at least an additive benefit
- Hints of durability of response - builds on signals seen with belzutifan in earlier studies
- Deliverable regimen – we do not know yet about dosing intensity. The toxicity looked encouragingly manageable.
- This analysis is exploratory, and we do not yet have mature OS data
- It is not yet time to change to this triplet regimen, but this is encouraging, and we await the results of the phase III LITESPARK012 trial
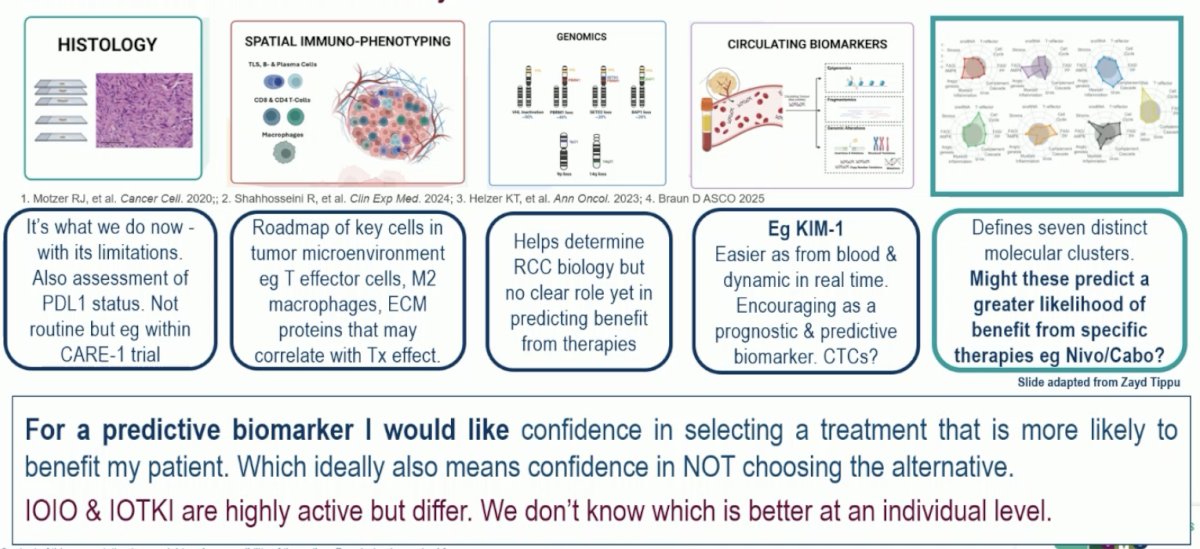
Next, discussing the OPTIC RCC trial, Dr. Pickering noted that the search for reliable biomarkers in RCC has been challenging with inconsistent results.
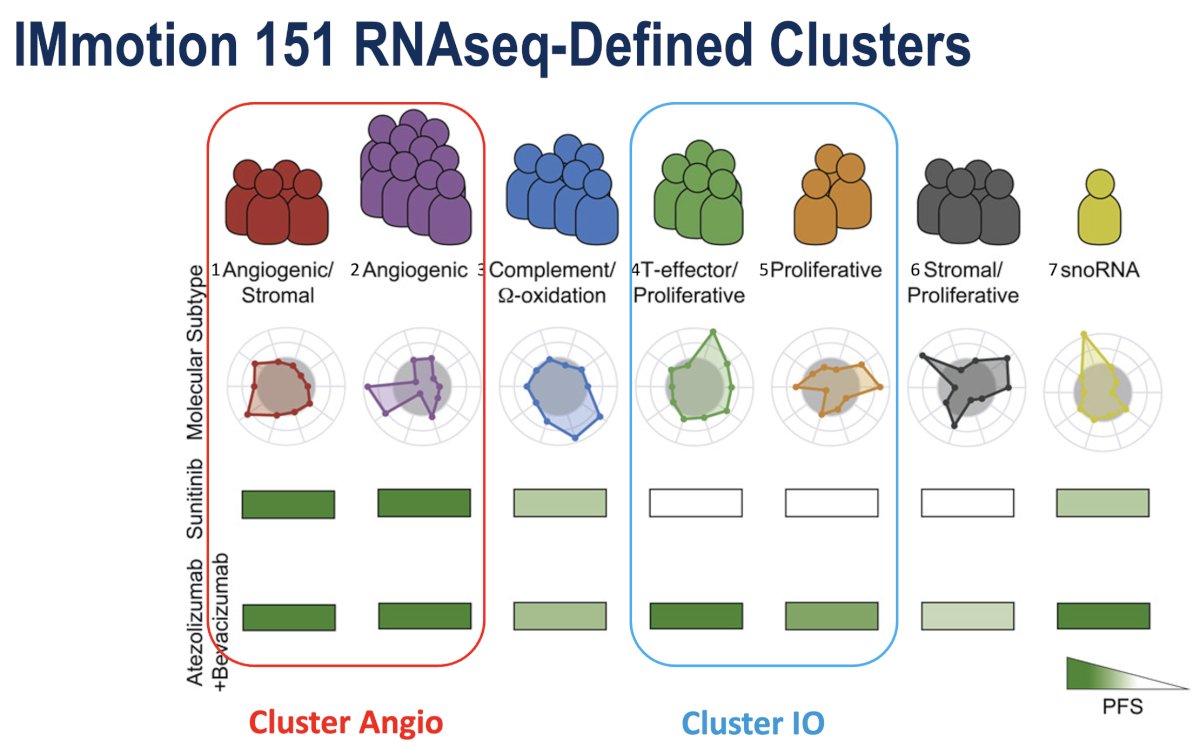
The origins of the OPTIC RCC study can be traced back to the IMmotion 151 study, a randomized phase III clinical trial comparing sunitinib to the combination of atezolizumab plus bevacizumab in previously untreated kidney cancer.3 Unsupervised clustering was performed using the gene expression data, grouping similar tumors into "clusters".
Shown below are the 7 clusters. Two of these clusters exhibited a strong angiogenic gene expression signature. These tumors are referenced as "cluster 1/2 or cluster angio".
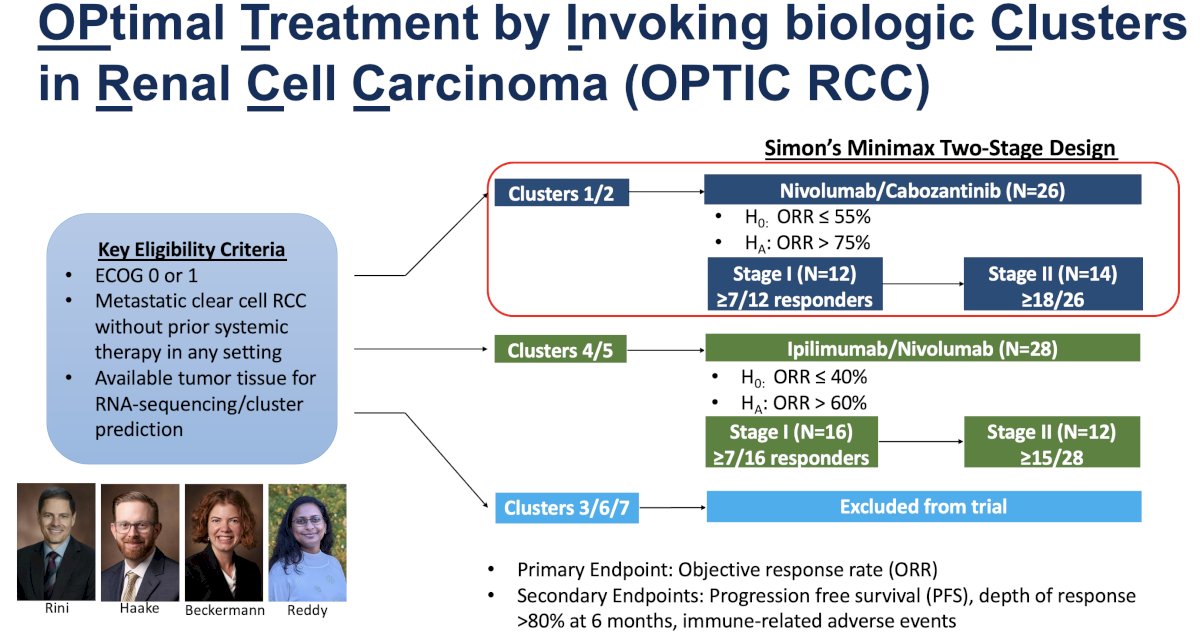
Based on these groups of clusters, the study investigators designed the OPtimal Treatment by Invoking biologic Clusters in Renal Cell Carcinoma (OPTIC) RCC study. The goal was to take these ”tumor clusters” or “gene expression signatures” that retrospectively correlated with drug response and prospectively evaluate their ability to enrich for drug response.
The key eligibility criteria were as follows:
- Metastatic ccRCC without prior systemic therapy in any setting
- Available tumor tissue for RENA sequencing/cluster prediction
- ECOG 0 or 1
Tumors were allocated to treatment arms based on cluster assignment:
- Cluster 1/2 patients were treated with cabozantinib plus nivolumab, a regimen with a potent anti-angiogenic drug (cabozantinib) as well as the anti-PD1 ICI nivolumab.
- The primary endpoint was ORR
- Cluster 4/5 was treated with the dual ICI regimen of ipilimumab plus nivolumab. This arm remains open to accrual.
- Clusters 3, 6, and 7 were excluded from the study.
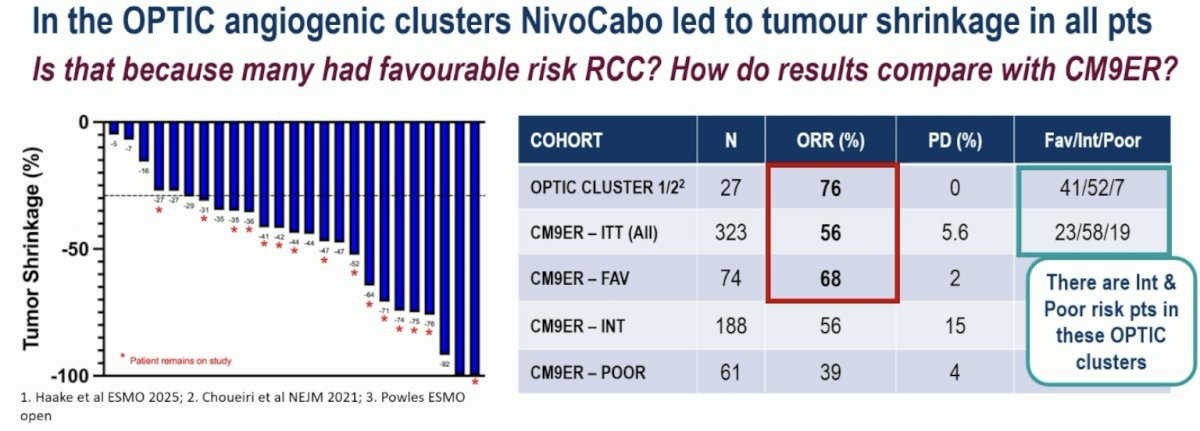
An ORR of 76% was observed in the Cluster 1/2 patients (PR: 68%). All patients exhibited some reduction in tumor burden. But were these results simply observed due to the fact that patients in Clusters 1/2 had favorable prognoses? Firstly, the ORR was higher than that observed in CheckMate-9ER.4 Additionally, all patients with IMDC intermediate and poor risk disease in this trial experienced tumor shrinkage, with no primary progressive disease (PD), which is highly encouraging.
Inevitably there are some limitations to this trial at this stage:
- The proportion of tumors deemed ‘angiogenic’ differed between samples from the renal primary and metastatic sites
- Likely due to ‘spatial and temporal’ heterogeneity and the ‘evolution’ of genetic changes
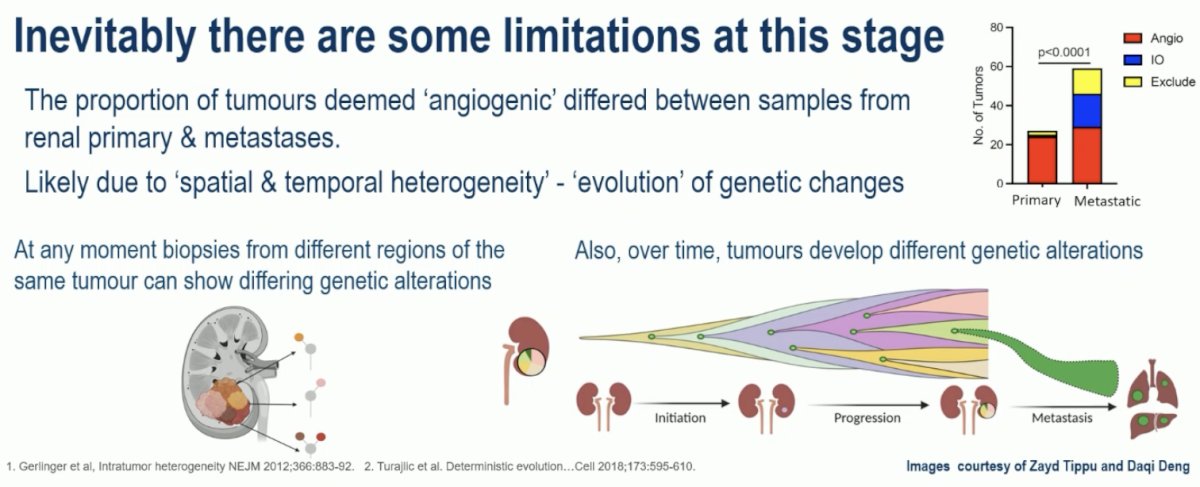
What does this mean from a practical standpoint?
- A biopsy from an archived renal primary is unlikely to represent the dominant driving biology/genetics at the time a patient develops progression
- Taking biopsies from metastatic sites is challenging, but is probably required for this strategy to yield its full potential
Additional limitations to this trial are as follows:
- The data are still early – patient numbers are small, and the efficacy endpoint is response
- It remains to be determined whether this approach enriches for a durable benefit
- Complexities and cost will be relevant for feasibility outside a research environment
In RCC, Dr. Pickering noted that we may need an integrated biomarker strategy, ideally incorporating blood markers. We must strongly encourage prospectively collected samples within clinical trials.
Dr. Pickering’s final thoughts about these trials in the advanced RCC landscape were as follows:
- Our research goals must be guided by what is important to patients
- Chance of eliminating all evidence of disease and response durability
- We have not seen any major new benefits in durable outcomes in advanced RCC that will lead us to radical changes in practice next week
- But often improvement is incremental
- We have seen new information that will guide us about optimal management now and inform better understanding with improved treatment choices in the future
Presented by: Lisa Pickering, MBBS, PhD, FRCP, Consultant, Medical Oncologist, The Royal Marsden, London, UK
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:- Choueiri TK, Powles T, Albiges L, et al. Cabozantinib plus nivolumab and ipilimumab in renal-cell carcinoma. N Engl J Med. 2023;388(18):1767–1778.
- Chahoud J, Liu S, Fellman B, et al. Zanzalintinib + nivolumab ± relatlimab in patients with previously untreated clear-cell renal-cell carcinoma: results from an expansion cohort of the phase 1b STELLAR-002 study. J Clin Oncol. 2025;43(16_suppl):4515 (Abstract).
- Motzer RJ, Powles T, Atkins MB, et al. Final overall survival and molecular analysis in IMmotion151, a phase III trial comparing atezolizumab plus bevacizumab vs sunitinib in patients with previously untreated metastatic renal-cell carcinoma. JAMA Oncol. 2022; 8(2):275-280.
- Motzer RJ, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021; 384(9):829–841.
A Multicenter Randomized Phase II Trial of Lenvatinib plus Everolimus Versus Cabozantinib in Patients with Metastatic Clear Cell RCC That Progressed on PD-1 Immune Checkpoint Inhibition (LenCabo).
ESMO 2025: LenCabo: A Randomized Phase II Multicenter Trial of Lenvatinib plus Everolimus versus Cabozantinib in Patients with Metastatic Clear Cell RCC that Progressed on PD-1 Immune Checkpoint Inhibition
Novel Pembrolizumab-Based Treatments as First-Line Therapy in Advanced Clear Cell Renal Cell Carcinoma: Substudy 03A of the Open-Label, Umbrella Platform, Phase I/II KEYMAKER-U03 Trial.
ESMO 2025: First-line Pembrolizumab-based Regimens for Advanced Clear Cell Renal Cell Carcinoma: KEYMAKER-U03 Substudy 03A
ESMO 2025: Kidney Cancer Discussant: Can we Combine More in Line 1 and Line 2?
Feasibility of Using an RNA-Seq Biomarker to Assign Therapy in the OPTIC RCC Trial - Pedro Barata