(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a rapid fire debate session on common problems and controversies in bladder cancer, moderated by Drs. Ashish Kamat and Arnulf Stenzl, and a presentation by Dr. Neha Vapiwala discussing radiation toxicity after trimodal therapy for muscle invasive bladder cancer and that radiation oncologists can and should take responsibility.
To begin this debate, Dr. Paramananthan Mariappan started with a case presentation of a 79 year old male patient with good performance status (golfs 3-4 times per week), ex-smoker (25 years ago), with no significant lower urinary tract symptoms, and an eGFR of 47 who presented with a 3.5 cm mixed appearing tumor on the right lateral wall of the bladder. He underwent a complete TURBT, with pathology showing a high grade, T2 urothelial carcinoma without CIS. Post-TURBT staging of the chest, abdomen, and pelvis showed no residual tumor, no hydronephrosis, and no metastases. After discussion with his treatment team, the patient elected for bladder preservation with chemoradiation for which he received 5-FU + mitomycin C and 55 Gy of radiotherapy in 20 fractions.
One month into the patient’s radiotherapy, he developed a pulmonary embolism and was started on apixaban. A 3 month post radiotherapy cystoscopy showed no cancer recurrence, but his bladder capacity had diminished substantially. A CT scan also showed a thick walled bladder with bilateral hydro-ureteronephrosis, and he was noted to have an acute kidney injury that was initially managed with an indwelling Foley catheter. Unfortunately, there was no improvement in his renal function, so bilateral nephrostomy tubes were inserted with a plan for an ileal conduit 6 months after his pulmonary embolism and anticoagulation. His renal function returned to normal, and bilateral nephrostograms and ureteroscopy were performed to rule out upper tract urothelial carcinoma. Secondary to development of urosepsis and stability of renal function with the bilateral nephrostomy tubes, the patient decided to keep the nephrostomy tubes and declined an ileal conduit. He also developed urge incontinence and intermittent gross hematuria, which was managed with anti-muscarinic medications.
Over subsequent follow-up, the patient had multiple issues with dislodgement of his nephrostomy tubes (with re-insertion), with recurrent sepsis that necessitated prophylactic antibiotics. A follow-up cystoscopy demonstrated no recurrence, and CT imaging still showed no evidence of metastatic disease. Ultimately, the patient decided to stop surveillance cystoscopy, as this had become increasingly painful secondary to his small, shrunken bladder.
Dr. Vapiwala started her portion of the debate by emphasizing that radical cystectomy and bladder preserving therapy, aka trimodality therapy, represent true victories for our bladder cancer patients. However, there are many factors that may impact the choice of trimodality therapy or radical cystectomy for muscle invasive bladder cancer patients:1
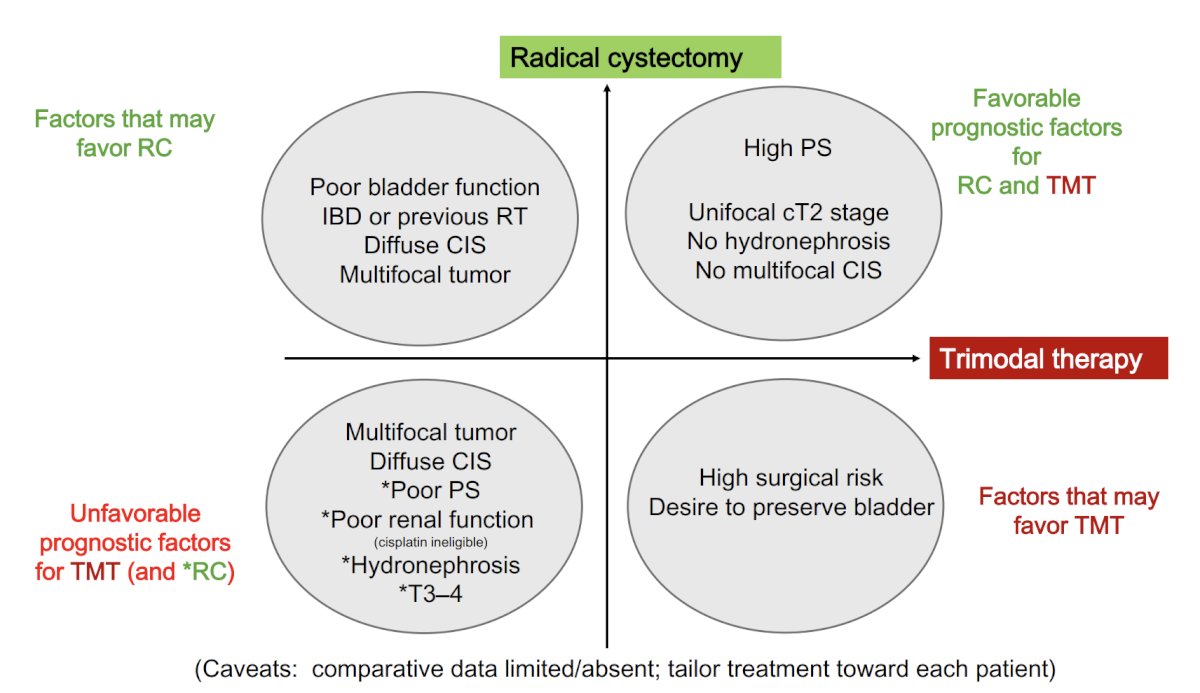
Moreover, for patients who are at high surgical risk but still have a desire to save their bladder, there are now emerging tools to help appropriately select patients, including RNA gene expression signatures, DNA damage and repair gene mutations, and ctDNA testing.
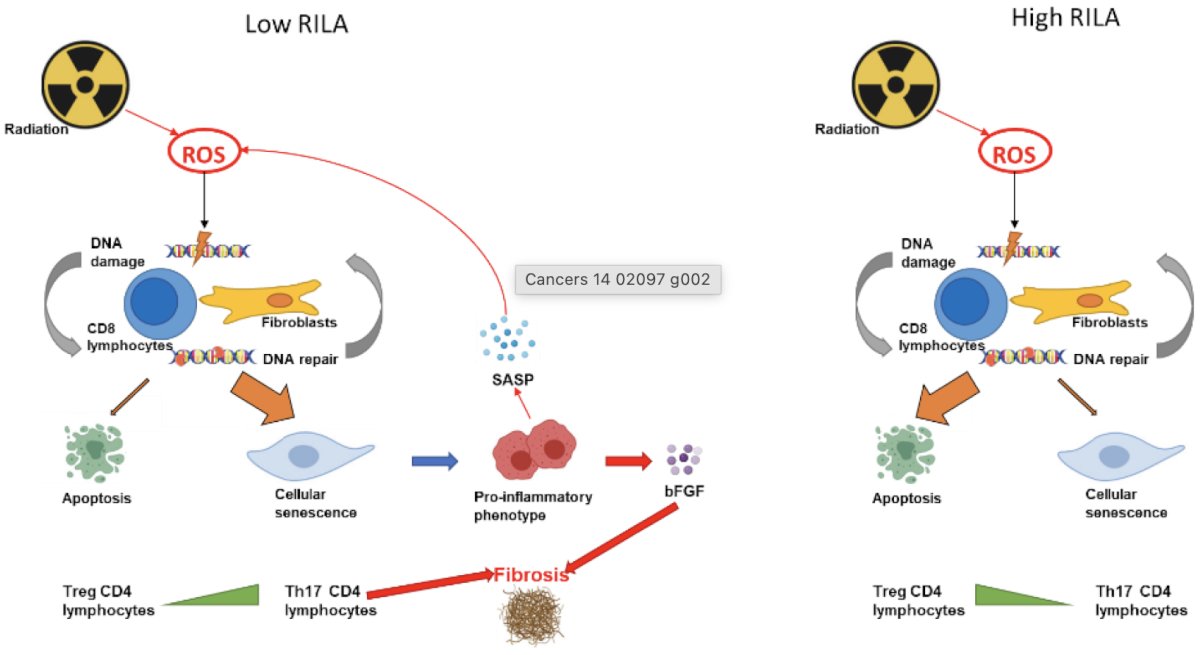
Are disease biology and patient selection predictors of treatment complications? Age and comorbidities for patients considering a radical cystectomy are a much bigger issue than for radiotherapy patients. The pre-test probability of a pulmonary embolism is also difficult to gauge, however there are risk scores (ie. Wells & PE Rule-out Criteria, YEARS algorithm, revised Geneva score, 4PEPS) available to assist. Other factors include the genetic radiotherapy sensitivity, diffuse CIS requiring a photodynamic diagnosis, and “no significant lower urinary tract function” (ie. good bladder function). Dr. Vapiwala notes that there is an inverse correlation of lymphocyte death and increased risk of developing late complications after radiotherapy:2
The Radiotoxicity Bladder Biomarkers prospective observational study assessed the correlation between electronic patient reported outcomes and biological markers of key parameters in acute radiation cystitis among patients with prostate cancer.3 This study included patients with low- or intermediate-risk localized prostate cancer who were eligible for localized radiotherapy. Blood and urinary biomarkers were analyzed before radiotherapy was initiated and at weeks 4 and 12 of radiation therapy. Patients completed questionnaires related to radiation cystitis symptoms and quality of life (IPSS and FACT-P) using a digital remote monitoring platform. The information was then processed by means of an algorithm, which classified patients according to the severity of symptoms and adverse events reported:
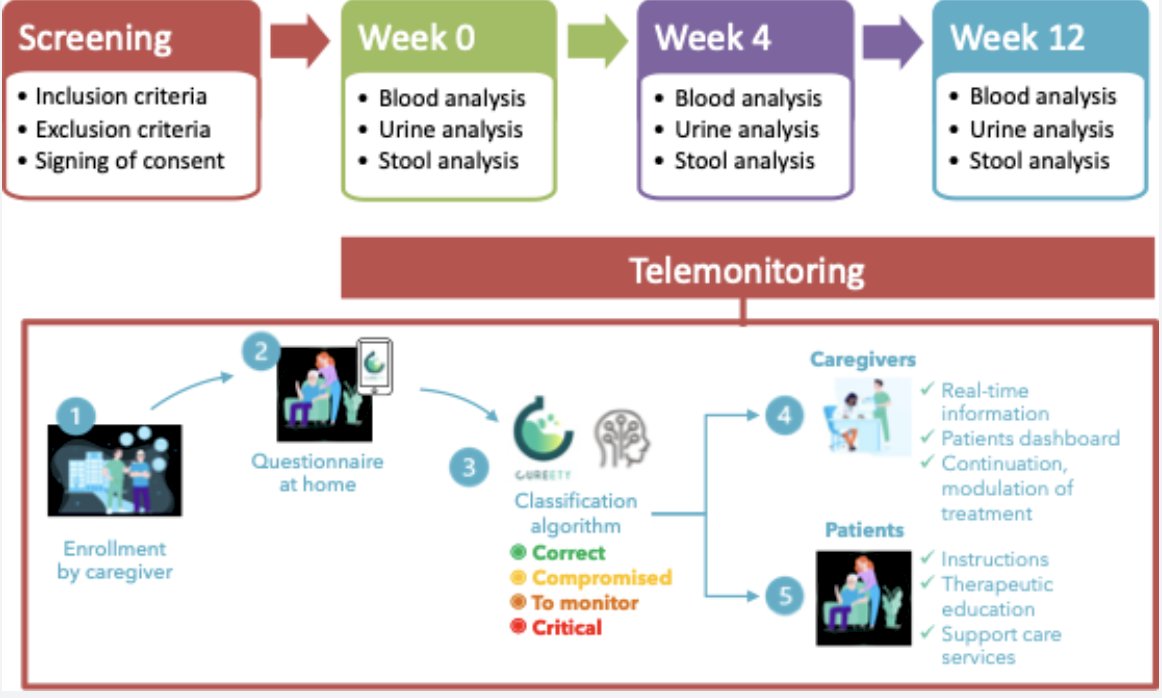
A total of 401 adverse events questionnaires were collected over the duration of this study from 20 patients. The most frequently reported adverse events at week 4 were pollakiuria, constipation, and diarrhea. A significant increase in the proportion of M2 phenotype cells (CD206+, CD163+, CD204+) at week 12 compared to week 0 was observed. Additionally, an increase in serum and urine levels of M-CSF, hepatocyte growth factor, and macrophagic inflammatory protein was observed at week 12 compared to baseline levels. Baseline serum and urine M-CSF concentrations showed a significant negative correlation with FACT-P scores at weeks 4 and 12 (r = -0.65, p = 0.04, and r = -0.76, p = 0.02, respectively). As such, the results of this study may help to develop mitigation strategies in order to limit radiation damage to the bladder.
It is important that we engage the entire care team to help patients prepare for and get through treatment, which includes a prehabilitative and rehabilitative focus on exercise, nutrition, cardiovascular health, and psychological support. Post-procedure, there are fairly similar post trimodality therapy guideline recommendations and standard institutional protocols. These include a personalized, risk based approach based on clinical factors, patient reported outcomes, non-invasive imaging surveillance, and predictive biomarkers. Additionally, Dr. Vapiwala advocates for a multi-disciplinary pelvic radiotherapy symptom management clinic.
Dr. Vapiwala concluded her presentation discussing radiation toxicity after trimodal therapy for muscle invasive bladder cancer, and that radiation oncologists can and should take responsibility with the following take-home points:
- Radiation oncologists continue to improve the therapeutic index, with (sometimes more than) a little help from urologic friends
- We must understand the biology of complications and refine patient selection
- If we predict who may be at risk, we can modify our plan and perhaps improve treatment tolerability
- We need to follow patients more closely
- Communication, collaboration, and leveraging our respective expertise is key
- Ashish M. Kamat, MD, MBBS, MD Anderson Cancer Center, Houston, TX
- Arnulf Stenzl, MD, University Hospital Tubingen, Tubingen, Germany
Case Presenter: Paramananthan Mariappan, FRCS(Urol), PhD, Edinburgh, Scotland, United Kingdom
Debater: Neha Vapiwala, MD, FASTRO, Perelman School of Medicine, University of Pennsylvania, Philadelphia, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Related content: Managing Radiation Toxicity After Trimodal Therapy for Bladder Cancer - Antoine Van Der Heijden & Neha Vapiwala
References:
- Gupta S, Hensley PJ, Li R, et al. Bladder preservation strategies in muscle-invasive bladder cancer: Recommendations from the International Bladder Cancer Group. Eur Urol. 2026 Jan;89(1):18-28.
- Lapierre A, Bourillon L, Larroque M, et al. Improving patients’ life quality after radiotherapy treatment by predicting late toxicities. Cancers (Basel). 2022 Apr 22;14(9):2097.
- Helissey C, Cavallero S, Guitard N, et al. Correlation between electronic patient-reported outcomes and biological markers of key parameters in acute radiation cystitis among patients with prostate cancer (RABBIO): Prospective observational study. JMIR Cancer. 2024 Dec 12:10:e48225.
EAU 2026: TMT for MIBC: Radiation, Responsibility, and Recurrences -- Who Manages the Fallout, and How? Debater 1: Radiation Toxicity Is Real and Its Urologists Who Manage the Consequences