(UroToday.com) The 2026 European Association of Urology (EAU) annual meeting featured a rapid fire debate session on common problems and controversies in bladder cancer moderated by Drs. Ashish Kamat and Arnulf Stenzl, and a presentation by Dr. Antoine van der Heijden discussing radiation toxicity after trimodal therapy for muscle invasive bladder cancer and the role of the urologist in managing the consequences.
To begin this debate, Dr. Paramananthan Mariappan started with a case presentation of a 79 year old male patient with good performance status (golfs 3-4 times per week), ex-smoker (25 years ago), with no significant lower urinary tract symptoms, and an eGFR of 47 who presented with a 3.5 cm mixed appearing tumor on the right lateral wall of the bladder. He underwent a complete TURBT, with pathology showing a high grade, T2 urothelial carcinoma without CIS. Post-TURBT staging of the chest, abdomen, and pelvis showed no residual tumor, no hydronephrosis, and no metastases. After discussion with his treatment team, the patient elected for bladder preservation with chemoradiation for which he received 5-FU + mitomycin C and 55 Gy of radiotherapy in 20 fractions.
One month into the patient’s radiotherapy, he developed a pulmonary embolism and was started on apixaban. A 3 month post radiotherapy cystoscopy showed no cancer recurrence, but his bladder capacity had diminished substantially. A CT scan also showed a thick walled bladder with bilateral hydro-ureteronephrosis, and he was noted to have an acute kidney injury that was initially managed with an indwelling Foley catheter. Unfortunately, there was no improvement in his renal function, so bilateral nephrostomy tubes were inserted with a plan for an ileal conduit 6 months after his pulmonary embolism and anticoagulation. His renal function returned to normal, and bilateral nephrostograms and ureteroscopy were performed to rule out upper tract urothelial carcinoma. Secondary to development of urosepsis and stability of renal function with the bilateral nephrostomy tubes, the patient decided to keep the nephrostomy tubes and declined an ileal conduit. He also developed urge incontinence and intermittent gross hematuria, which was managed with anti-muscarinic medications.
Over subsequent follow-up, the patient had multiple issues with dislodgement of his nephrostomy tubes (with re-insertion), with recurrent sepsis that necessitated prophylactic antibiotics. A follow-up cystoscopy demonstrated no recurrence, and CT imaging still showed no evidence of metastatic disease. Ultimately, the patient decided to stop surveillance cystoscopy, as this had become increasingly painful secondary to his small, shrunken bladder.
Following the case presentation, Dr. van der Heijden started his presentation by noting that the downside of radiotherapy includes:
- Impaired tissue healing
- A latency period of up to 30 years
- Improved cancer survival results and more late side effects
- A major impact on quality of life
- Radiotherapy to the lower abdomen/pelvis leads to gastrointestinal and genitourinary complications
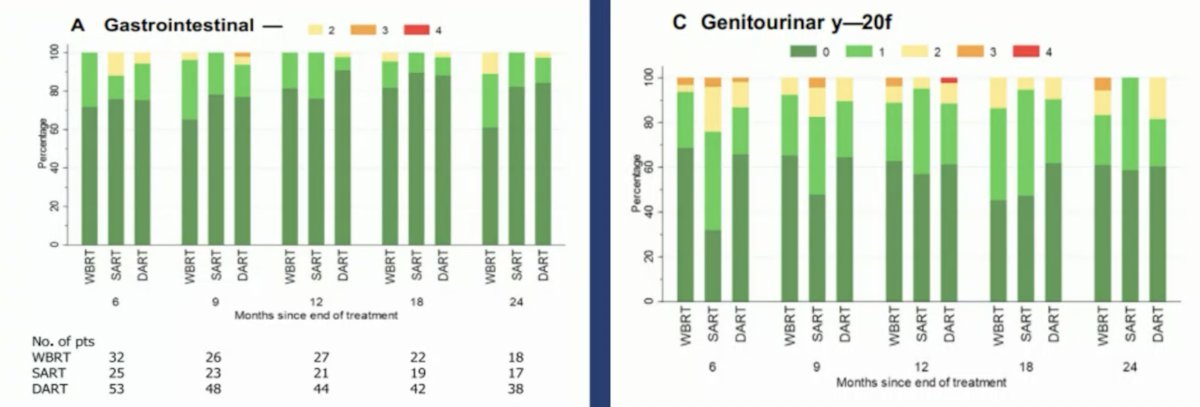
In the phase 2 RAIDER randomized controlled trial assessing dose-escalated adaptive radiotherapy for bladder cancer,1 Huddart and colleagues found that grade 2-3 gastrointestinal adverse events occurred in 5-10% of patients and grade 2-4 genitourinary adverse events occurred in 10-15% of patients in this trial:
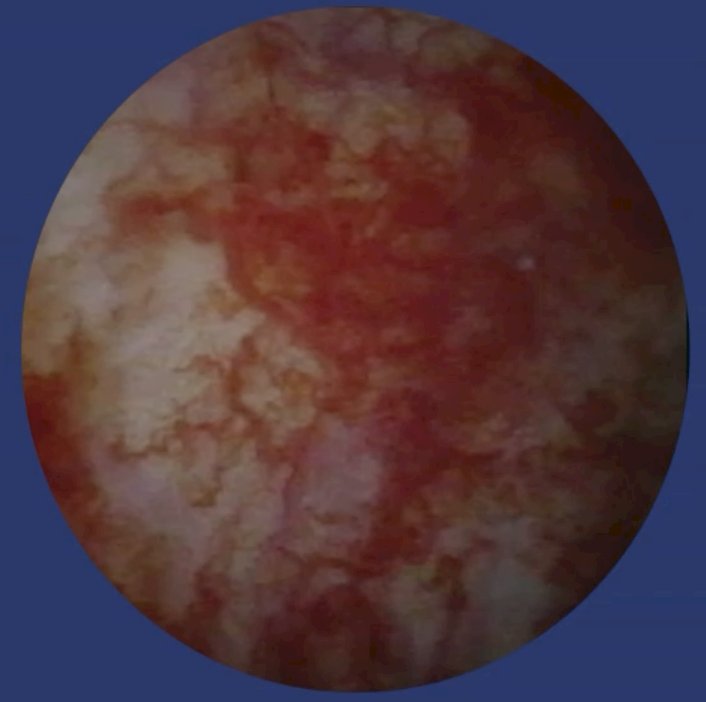
When looking specifically at radiotherapy induced genitourinary complications, the most common are radiation cystitis, strictures, urinary fistulae, and secondary malignancies. Less common complications include erectile dysfunction, lower urinary tract dysfunction, bladder fibrosis, and osteonecrosis. Radiation cystitis occurs in 5-10% of patients after pelvic radiotherapy, with acute radiation cystitis typically being self-limiting for ~3 months, and usually treated with anticholinergics. The main symptom of chronic radiation cystitis is hematuria, and is most often treated by urologists:
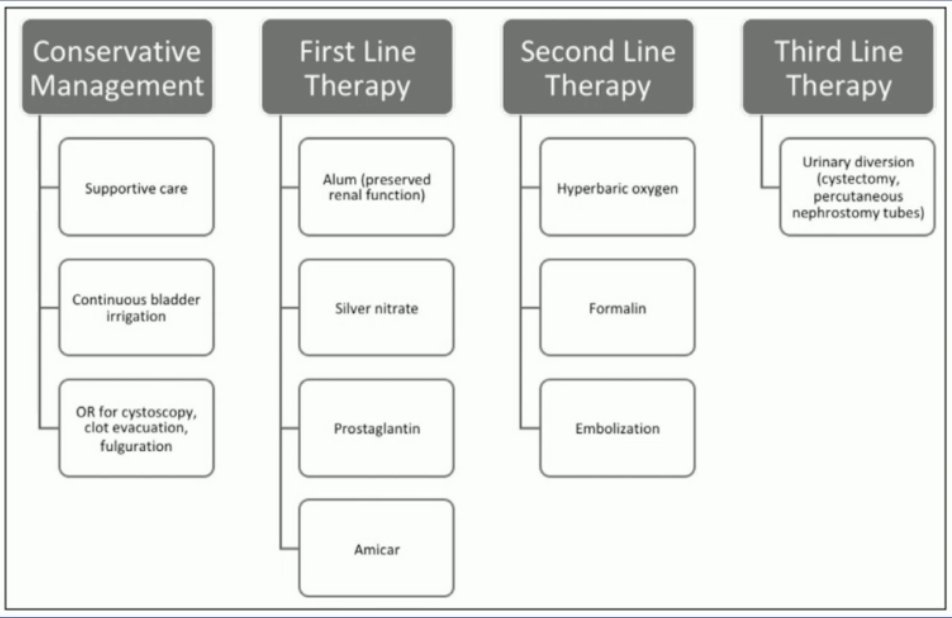
Treatment of chronic radiation cystitis usually starts with conservative management (supportive care, continuous bladder irrigation, or cystoscopy +/- clot evacuation/fulguration), but may also include first, second, and third line therapy options:2
As such, urologists play a central role in both the diagnosis and treatment of these complications.
Bladder fibrosis is a very rare complication after pelvic radiotherapy. The pathophysiology is such that ischemia stimulates progressive fibrosis of the bladder wall, leading to (i) decreased bladder capacity, (ii) ureteral strictures and hydronephrosis, and (iii) urinary incontinence. These sequelae often lead to urinary diversion and/or ureteral stents.
Dr. van der Heijden concluded his presentation discussing radiation toxicity after trimodal therapy for muscle invasive bladder cancer and the role of the urologist in managing the consequences by emphasizing the importance of urologists and radiation oncologists working collaboratively together to best treat these patients.
Moderators:
- Ashish M. Kamat, MD, MBBS, MD Anderson Cancer Center, Houston, TX
- Arnulf Stenzl, MD, University Hospital Tubingen, Tubingen, Germany
Case Presenter: Paramananthan Mariappan, FRCS(Urol), PhD, Edinburgh, Scotland, United Kingdom
Debater: Antoine van der Heijden, MD, PhD, Radboud University Medical Center, Nijmegen, The Netherlands
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2026 European Association of Urology (EAU) Annual Meeting, London, United Kingdom, Fri, Mar 13 – Mon, Mar 16, 2026.
Related content: Managing Radiation Toxicity After Trimodal Therapy for Bladder Cancer - Antoine Van Der Heijden & Neha Vapiwala
References:
- Huddart R, Hafeez S, Griffin C, et al. Dose-escalated adaptive radiotherapy for bladder cancer: Results of the phase 2 RAIDER randomized controlled trial. Eur Urol. 2025 Jan;87(1):60-70.
- D’Amico MJ, Foss H, Uhr A, et al. Hemorrhagic cystitis: A review of the literature and treatment options. Can J Urol. 2022 Oct;29(5):11276-11283.
EAU 2026: TMT for MIBC: Radiation, Responsibility, and Recurrences -- Who Manages the Fallout, and How? Debater 2: Toxicity Happens but Is Manageable -- Radiation Oncologists Can and Should Take Responsibility