(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between February 26th and 28th 2026, was host to the session Treatment Selection, Response Assessment, and Monitoring Across the Spectrum of Advanced Prostate Cancer. Dr. Dana Rathkopf presented New Treatment Options for Patients With Castrate-Resistant Prostate Cancer.
Dr. Rathkopf framed the treatment of mCRPC as “ABC.” A refers to androgen receptor pathway inhibitors, which remain the backbone of therapy and the foundation for most patients. B represents biomarker-driven and bone-targeted strategies, including immune checkpoint inhibition for MSI-H/dMMR disease, PARP inhibitors for HRR-altered tumors, PSMA-targeted radioligand therapy for PSMA-positive disease, and radium-223 for bone-predominant metastases. C stands for chemotherapy, primarily docetaxel and cabazitaxel.
Dr. Rathkopf emphasized that the key principle in mCRPC management is to select the treatment that best fits the patient, not to fit the patient to the treatment. She highlighted how ASCO has operationalized this approach in the ASCO Living Guidelines, which integrate molecular profiling and clinical context to guide therapy selection. The guidelines stratify patients by prior therapies and biomarker status, including HRR alterations, MSI-H/dMMR, and PSMA expression, and align treatment recommendations accordingly across ARPIs, PARP inhibitors, PSMA-targeted radioligand therapy, chemotherapy, and bone-directed agents. This pathway-based framework reinforces a personalized, biology-driven strategy rather than a one-size-fits-all sequencing model.
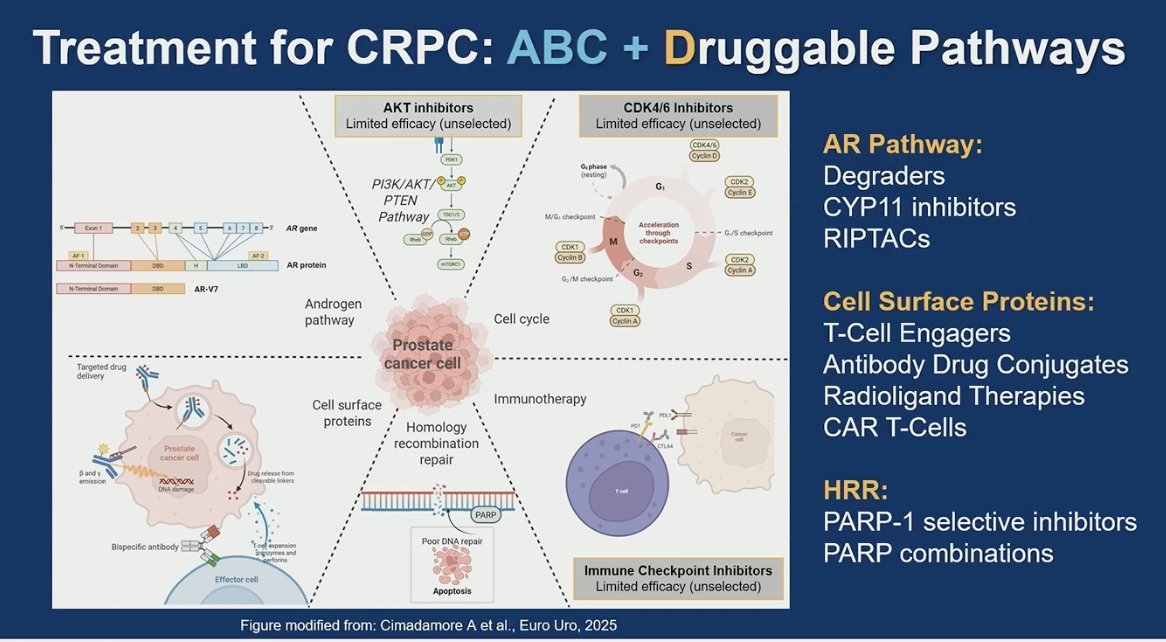
Treatment of CRPC is about to become more complex. Beyond the traditional ABC framework, multiple druggable (D) pathways are emerging, including the androgen receptor pathway with degraders, CYP11 inhibitors, and RIPTACs; cell surface–targeted strategies such as T-cell engagers, antibody–drug conjugates, radioligand therapies, and CAR T cells; and DNA repair–focused approaches including PARP-1–selective inhibitors and PARP-based combinations.
She emphasized that we are not ready to close the door on any of these pathways. While some agents have shown limited efficacy in unselected populations, there remains a clear biologic rationale and ongoing investigation aimed at better patient selection, rational combinations, and optimized sequencing. The field is moving toward increasingly precise targeting of tumor biology, rather than abandoning pathways prematurely based on early-generation results.
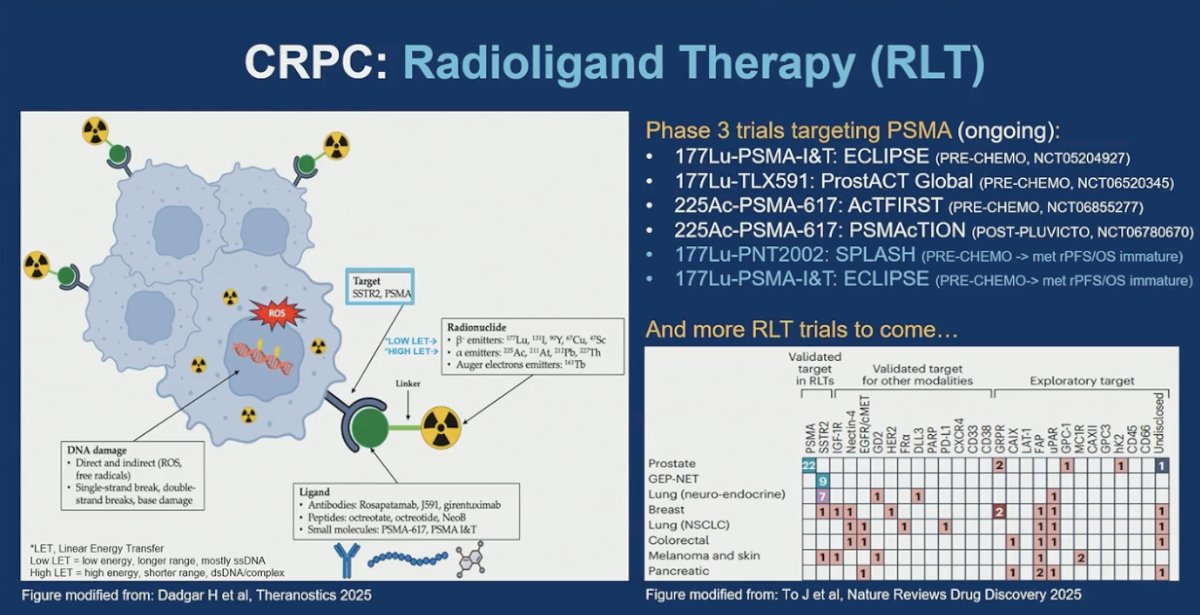
Dr. Rathkopf emphasized that radioligand therapy in CRPC is entering prime time, with two validated targets already approved and multiple phase 3 trials evaluating PSMA-directed agents earlier in the disease course, including pre-chemotherapy settings. She underscored that RLT represents a platform rather than a single agent strategy, with additional targets under active investigation, signaling that this approach is likely to become an increasingly integral component of CRPC management.
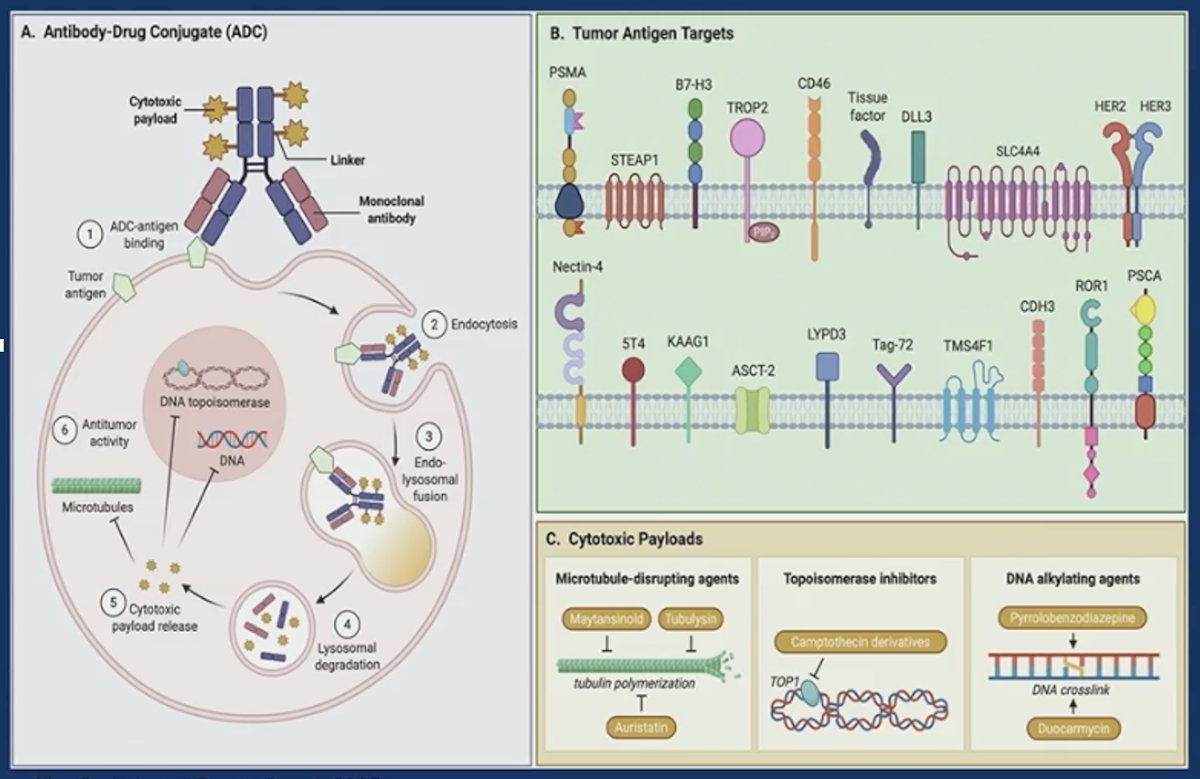
Dr. Rathkopf also discussed antibody–drug conjugates in CRPC, highlighting their mechanism of delivering a potent cytotoxic payload directly into tumor cells through a monoclonal antibody, thereby increasing intratumoral potency while aiming to limit systemic exposure. She noted that several tumor surface antigens are under investigation in prostate cancer, but clinical success depends on sufficient target density and consistent expression. Key considerations include off-target toxicities such as cytopenias, diarrhea, and neuropathy, as well as challenges with penetration into large tumors or dense bone metastases, where strategies such as bystander effect and repeat dosing may be required.
Dr. Rathkopf highlighted the early signal seen with I-DXd, a B7-H3–targeted ADC, noting a confirmed response rate of approximately 25 percent in the overall mCRPC cohort and a particularly notable 33% response rate among patients with liver metastases, a population typically associated with poor prognosis. The most common grade 3 toxicity was anemia, reflecting on-target or off-tumor effects consistent with the payload class. She also pointed out the thoughtful phase 3 trial design, which stratifies patients by site of metastatic disease, including bone-only versus other involvement, acknowledging the biologic and clinical heterogeneity of mCRPC. However, no formal correlative biomarker analyses have yet clearly defined which patients derive the greatest benefit, underscoring the continued need for predictive biomarkers alongside ADC development.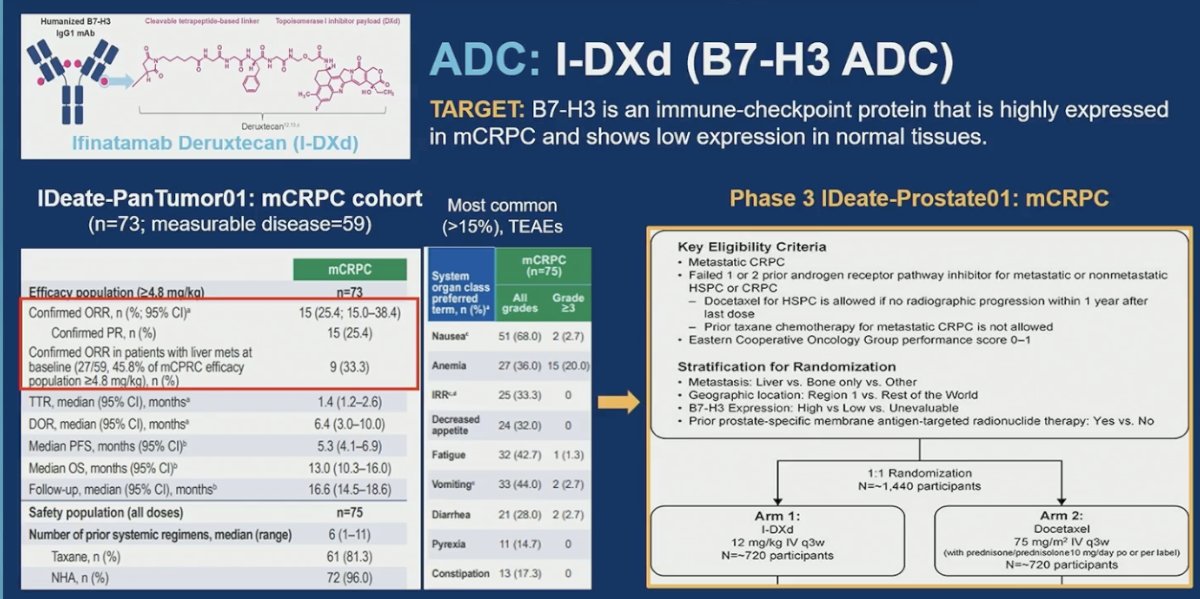
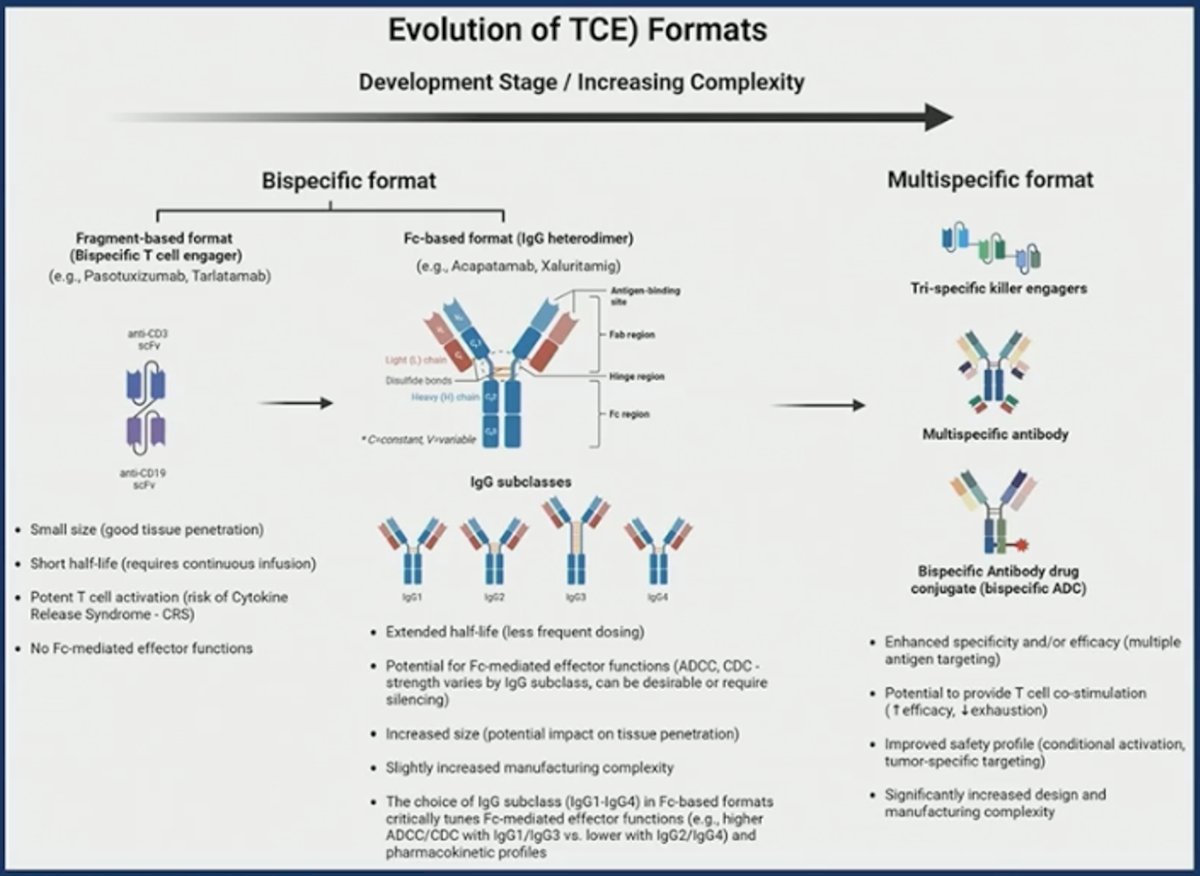
T-cell Engagers (TCE)
The next category discussed was T-cell engagers, a class well established in other malignancies but relatively new to prostate cancer. These agents move beyond passive targeting by actively recruiting T cells to the tumor, triggering immune synapse formation and amplifying cytotoxic activity. In doing so, they hold the potential to convert prostate cancer from a traditionally immune “cold” tumor into a more immune-responsive disease.
At the same time, important clinical considerations remain, including cytokine release syndrome (CRS), immune-related toxicities, antigen escape, and the influence of the tumor microenvironment. With thoughtful development and optimization, T-cell engagers could meaningfully reshape the immunotherapy landscape in advanced prostate cancer.
Among the T-cell engagers in development, STEAP1 × CD3 is one of the leading approaches. Xaluritamig is a bispecific antibody targeting STEAP1, which is highly overexpressed in prostate cancer with limited normal tissue expression, and CD3 to recruit T cells directly to the tumor. In heavily pretreated mCRPC, it demonstrated clear antitumor activity, including a PSA50 rate of 53.1%, PSA90 responses, and objective responses by imaging. Cytokine release syndrome was observed, primarily during cycle 1, as expected for this class, but was manageable with step-up dosing and standard supportive measures. Overall, the activity signal, including ORR, supports continued development in this space.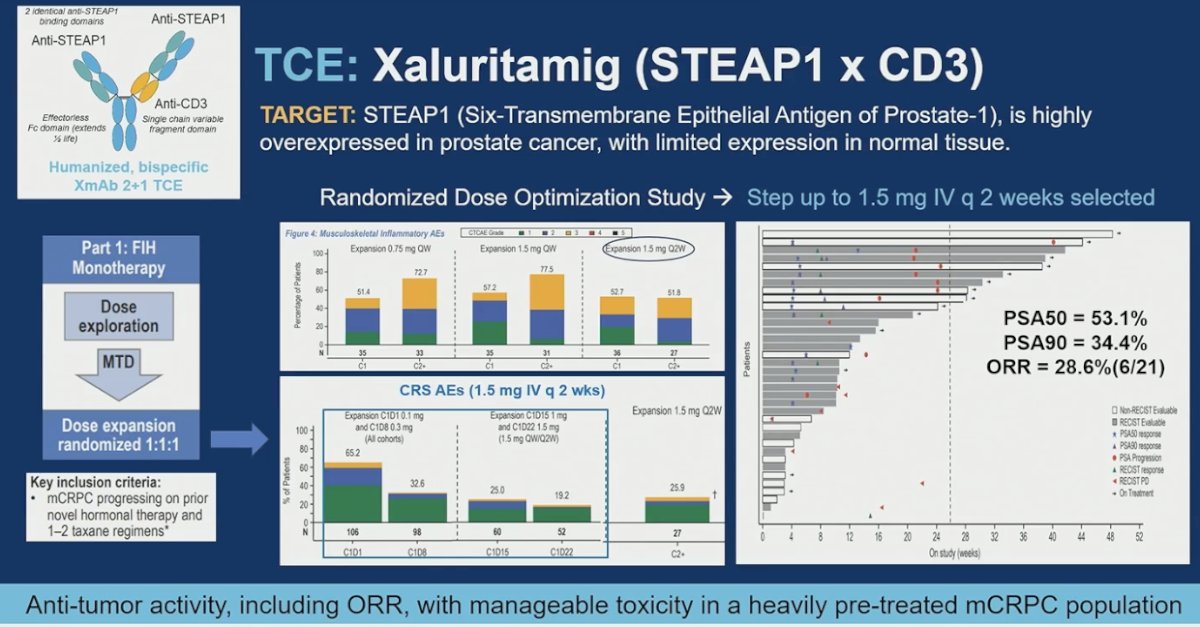
Another T-cell engager in development is pasritamig (KLK2 × CD3), targeting KLK2, a prostate-restricted antigen regulated by AR signaling. In a heavily pretreated mCRPC population, including patients previously exposed to taxanes, pasritamig demonstrated a PSA50 rate of 42.4% and a median rPFS of 7.85 months. Cytokine release syndrome was infrequent and predominantly low grade, supporting a well-tolerated outpatient regimen. Exploratory analyses evaluating dosing intervals suggested that longer intervals may reduce T-cell exhaustion and activation-induced T-cell death, providing a potential strategy to optimize durability of response while maintaining safety.

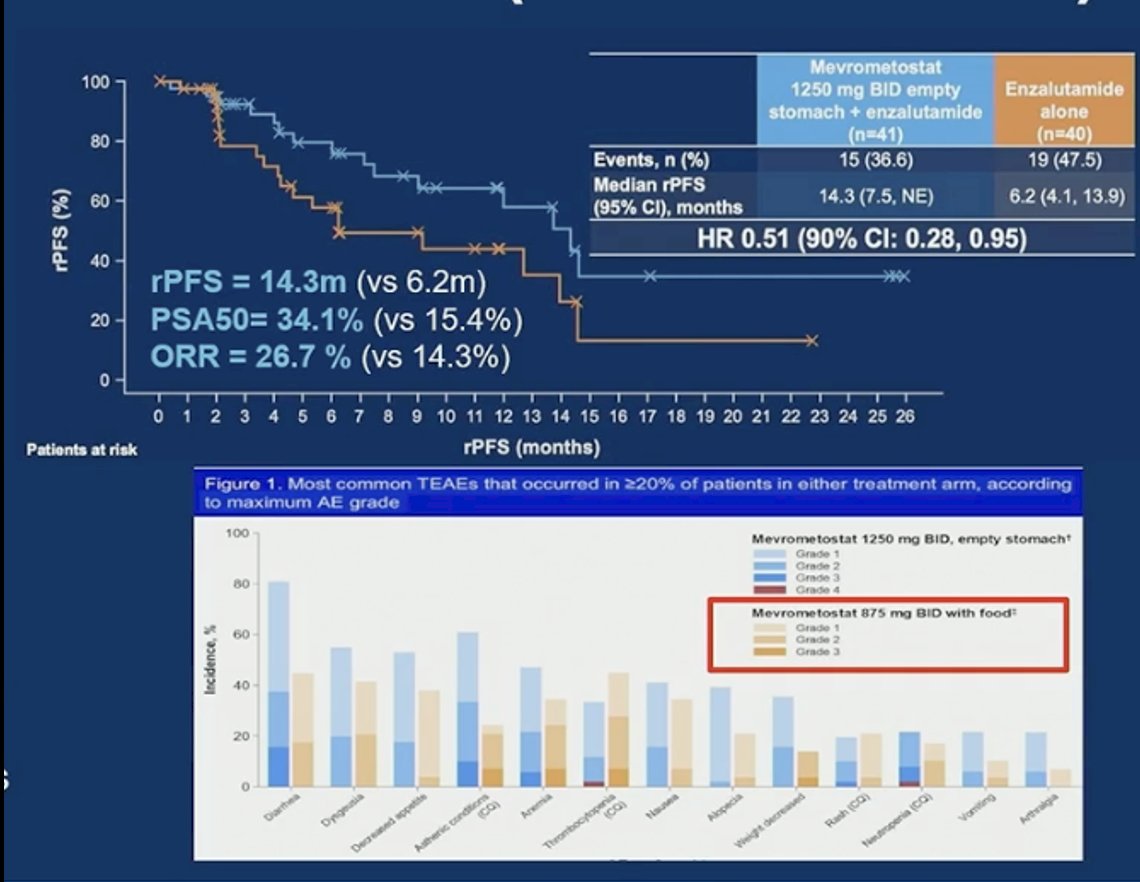
Mevrometostat, an EZH2 inhibitor, was evaluated in combination with enzalutamide and demonstrated antitumor activity at the higher dose administered on an empty stomach. At that dose, median rPFS was 14.3 months, with a PSA50 response rate of 34.1% and an objective response rate of 26.7%, compared with enzalutamide alone. However, increased gastrointestinal toxicity was observed at this schedule, prompting dose adjustment. Administration at a lower dose with food improved tolerability while maintaining similar efficacy signals. Overall, the data support the biologic activity of EZH2 inhibition in combination with AR blockade in mCRPC.
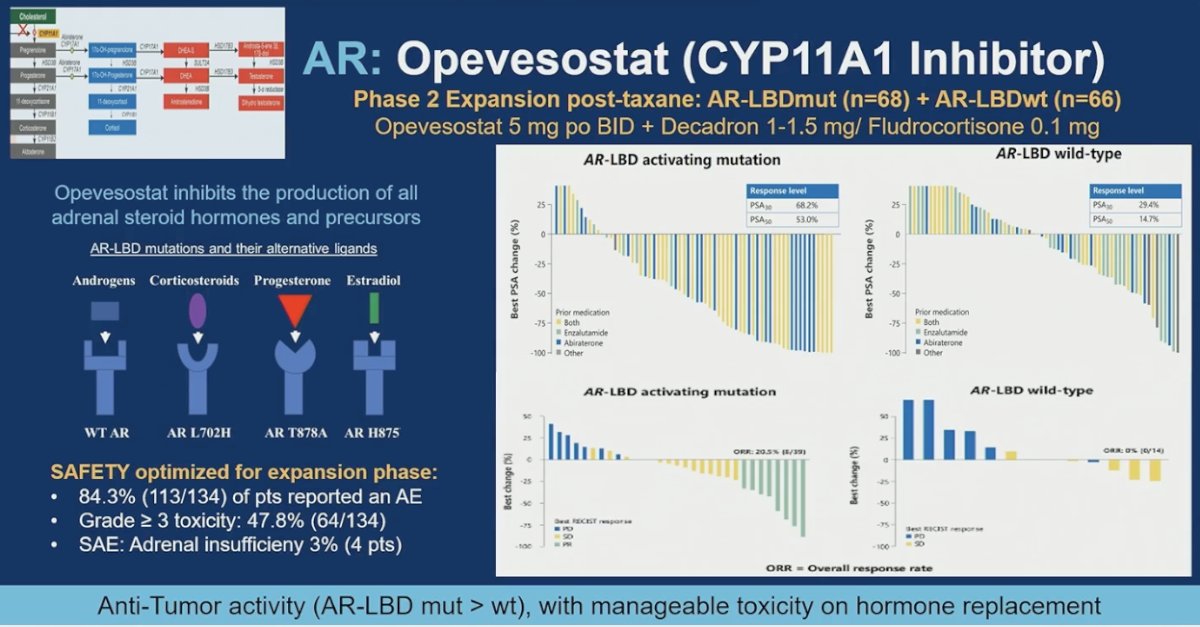
Opevesostat, a CYP11A1 inhibitor, suppresses production of adrenal steroid hormones and precursors and has demonstrated antitumor activity in both AR ligand-binding domain (LBD)–mutant and wild-type mCRPC. In the phase 2 expansion, responses were observed across both molecular subsets, with greater activity in AR-LBD–mutant tumors but meaningful responses also in wild-type disease. In the pre-chemotherapy population, median rPFS was 16.5 months, supporting the population now being evaluated in phase 3. The safety profile was manageable with hormone replacement, and although QTc prolongation was reported, events were controlled with dose modification. Overall, the data support continued development across biomarker-defined and unselected groups.
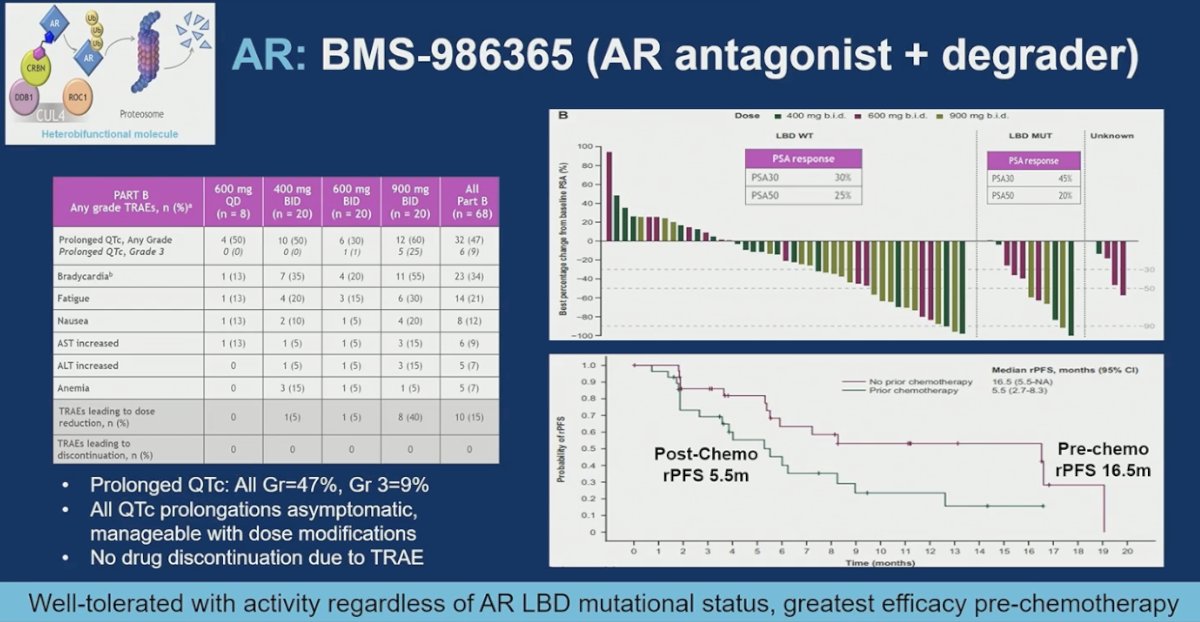
Moreover, BMS-986365 is a dual-function AR antagonist and degrader that has demonstrated activity across AR-LBD–mutant and wild-type mCRPC. Responses were observed in both molecular subsets, supporting the rationale that AR remains a valid target even in the presence of ligand-binding domain alterations. Activity appeared more pronounced in the pre-chemotherapy setting, with a median rPFS of 16.5 months compared with 5.5 months post-chemotherapy. The safety profile was manageable, with QTc prolongation reported in a subset of patients, predominantly low-grade and asymptomatic, and controlled with dose modification. Importantly, no treatment discontinuations occurred due to QTc events. The ongoing phase 3 trial is expected to further clarify efficacy across AR-LBD mutational subgroups.
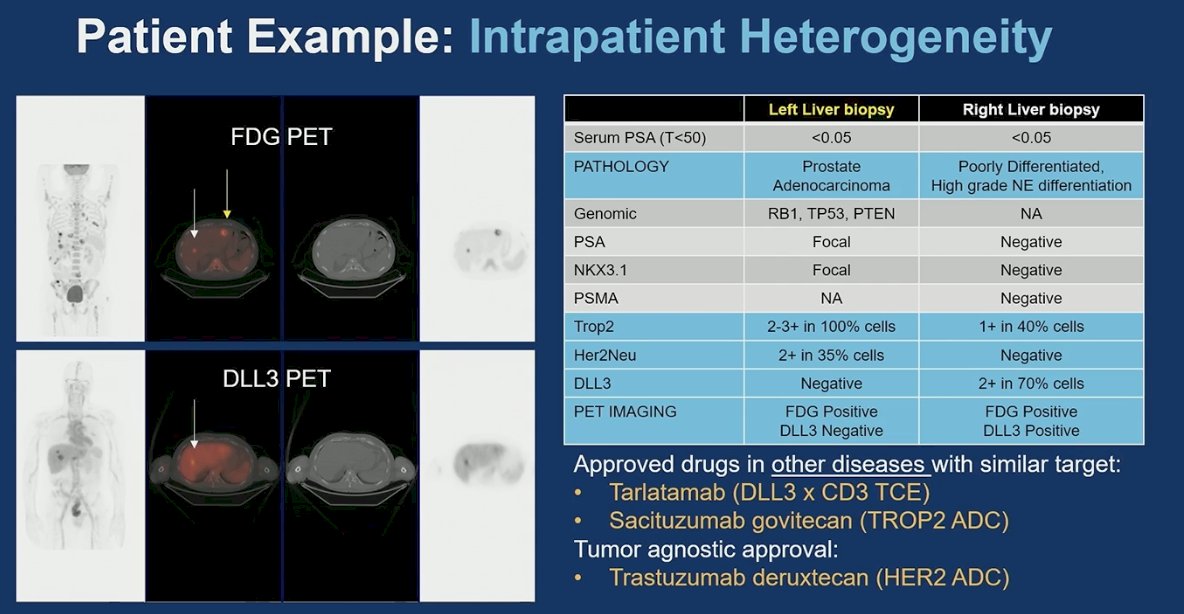
Initially, the importance of lineage plasticity was emphasized. Prostate cancer is not static, and under therapeutic pressure, tumors can evolve into distinct phenotypes within the same patient. The example presented illustrated intrapatient heterogeneity, with one liver lesion consistent with adenocarcinoma and another demonstrating high-grade neuroendocrine differentiation, accompanied by divergent biomarker expression and imaging characteristics. This biologic divergence has direct therapeutic implications, as different lesions may express targets such as DLL3, TROP2, or HER2, opening the door to agents approved in other malignancies. Recognizing lineage plasticity is critical, as it underscores the need for repeat biopsy, molecular reassessment, and adaptive treatment strategies rather than assuming uniform disease biology throughout the course of CRPC.
Dr. Rathkopf concluded her presentation with the following key takeaway points:
- Many promising new therapeutic targets and drug classes are in late-stage (phase 3) development for mCRPC.
- Treatment selection will increasingly require integration of prior therapies, molecular profiling, advanced imaging, resistance mechanisms, toxicity profiles, and overall clinical context.
- Future directions include rational combination strategies and refinement of therapeutic delivery, sequencing, and duration.
- Clinical decision-making must carefully balance efficacy and toxicity to maximize patient benefit while preserving quality of life.
Presented by: Dana E. Rathkopf, MD, Medical Oncologist, Associate Chair, Junior Faculty Development, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY