(UroToday.com) The 2025 GU ASCO annual meeting featured a prostate cancer session and a discussant presentation by Dr. Edwin Posadas discussing two abstracts: “Radical prostatectomy versus radiotherapy in high-risk prostate cancer: Emulated randomized comparison with individual patient data from two phase III randomized trials” by Dr. Soumyajit Roy and “Gene signature predictor of dose-response to prostate radiation: Validation of PORTOS in phase III trials” by Dr. Shuang Zhao. Starting with Dr. Roy’s presentation, Dr. Posadas states that he agrees with the two trials selected for this analysis, namely that the CALGB 90203 (PUNCH) trial and NRG/RTOG 0521 trials were:
- Prospective, cooperative group studies used to avoid bias and confounding from registries and retrospective institutional studies
- Distant metastasis was used as a point of comparison
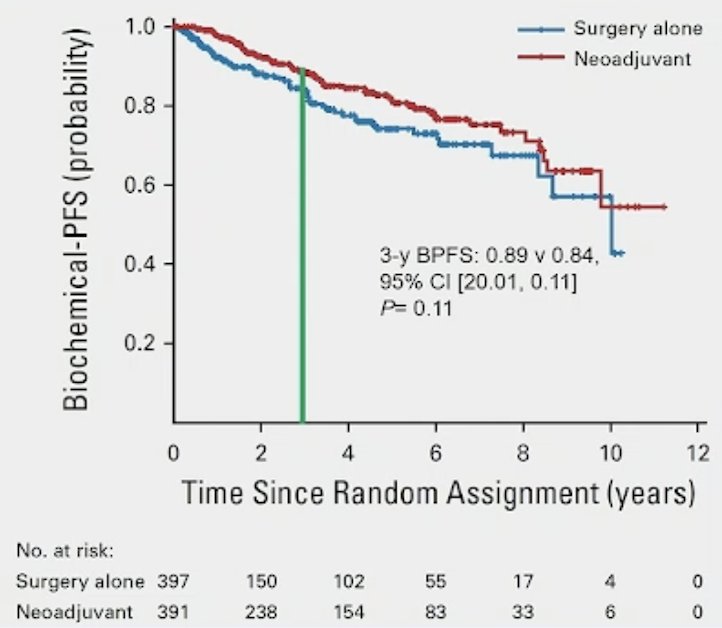
The CALGB 90203 (PUNCH) trial1 assessed men with clinically localized, high-risk prostate cancer, defined as clinical stage T1-3a with serum PSA levels less than or equal to 100 ng/mL within 6 weeks of prostate biopsy, without evidence of radiographic metastatic disease on bone scan and axial imaging (CT or MRI). After enrollment, patients were randomly assigned in a 1:1 fashion to receive either radical prostatectomy alone or ADT plus docetaxel followed by radical prostatectomy. The primary study endpoint was biochemical progression free survival (BPFS) at 3-years, defined as a serum PSA level > 0.2 ng/mL that increased on two consecutive occasions that were at least three months apart. Secondarily, the authors considered BPFS at 5-years, BPFS overall as a time to event outcome, local recurrence, metastasis-free survival, prostate cancer-specific mortality, and overall survival. A total of 788 men were randomly assigned of whom 738 (391 in the neoadjuvant therapy arm and 397 in the surgery alone arm) actually underwent radical prostatectomy. Over a median follow-up of 6.1 years, the authors found no significant difference in 3-year BPFS (89% vs 84%; difference 5%, 95% CI for difference -1% to 11%; p = 0.11) or 5-year BPFS (81% vs 74%; difference 7%, 95% CI for difference -1% to 16%):
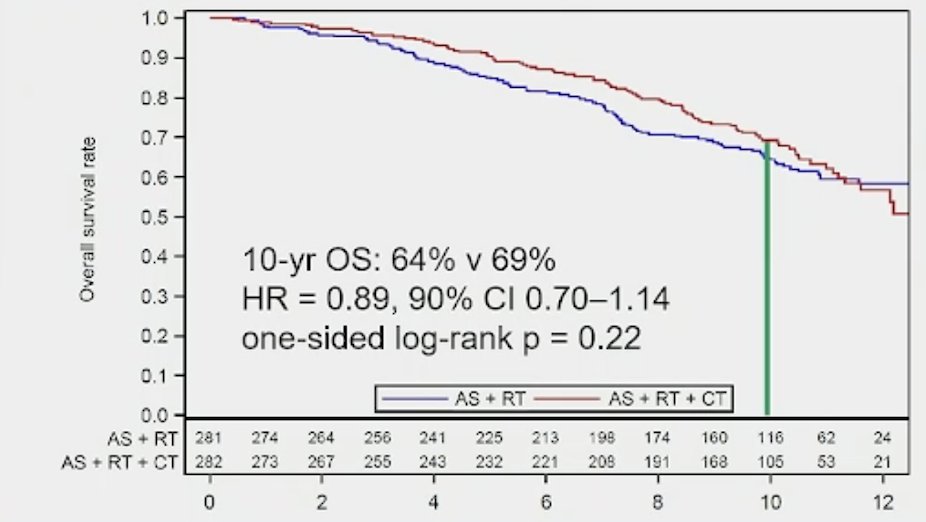
The NRG/RTOG 0521 randomized trial enrolled patients with high-risk nonmetastatic disease between 2005 and 2009. Patients (n = 563) were randomly assigned to receive standard long-term ADT plus radiotherapy with or without adjuvant chemotherapy. Median PSA level in the cohort was 15.1 ng/ml, with 53% of patients having Gleason Score 9-10 disease, and 27% having cT3-4 disease. Over a median follow-up of 5.7 years, the 4-year overall survival rate was 89% (95% CI: 84% -92%) for ADT and radiotherapy, compared to 93% (95% CI: 90% - 96%) for ADT and radiotherapy plus chemotherapy (HR: 0.69, 90%: CI 0.49-0.97).2 However, with additional long term follow-up, the 10 year overall survival rate was 64% versus 69% (HR 0.89, 90% CI 0.70-1.14):3
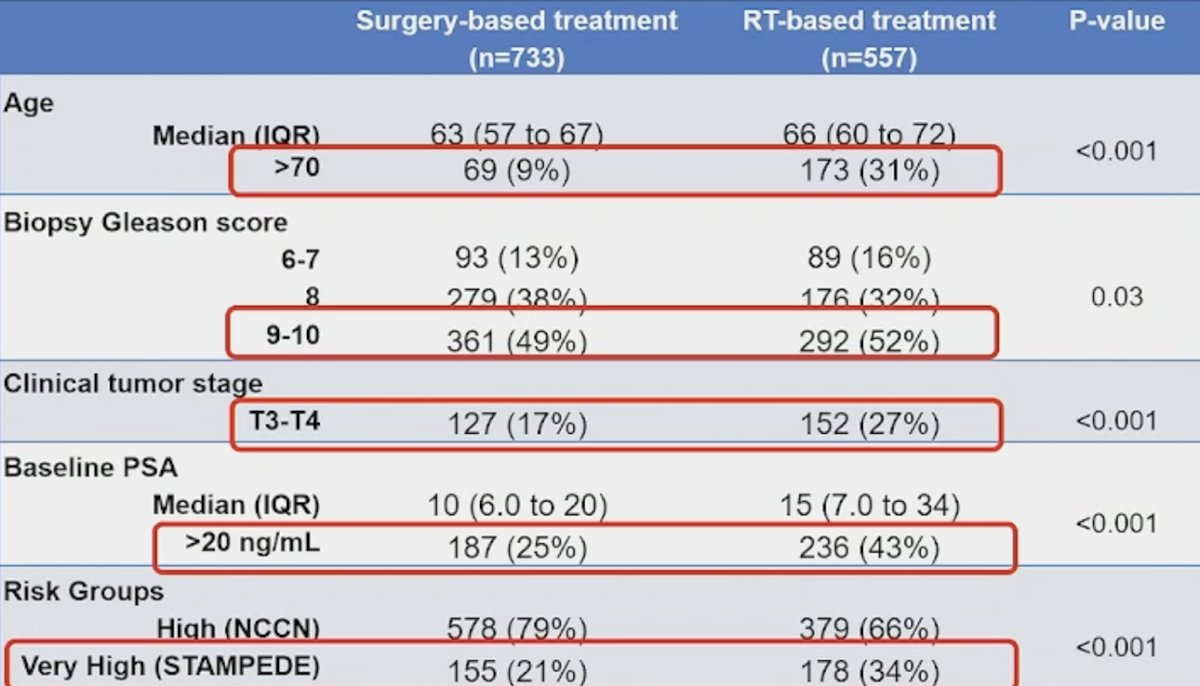
In Dr. Roy’s study presented at GU ASCO 2025, 1,290 patients (radiation therapy n = 557, radical prostatectomy n = 733) were included, with similar median follow-up of 6.4 years. Prior to IPTW, radical prostatectomy patients were significantly younger with lower baseline PSA compared to radiation therapy patients:
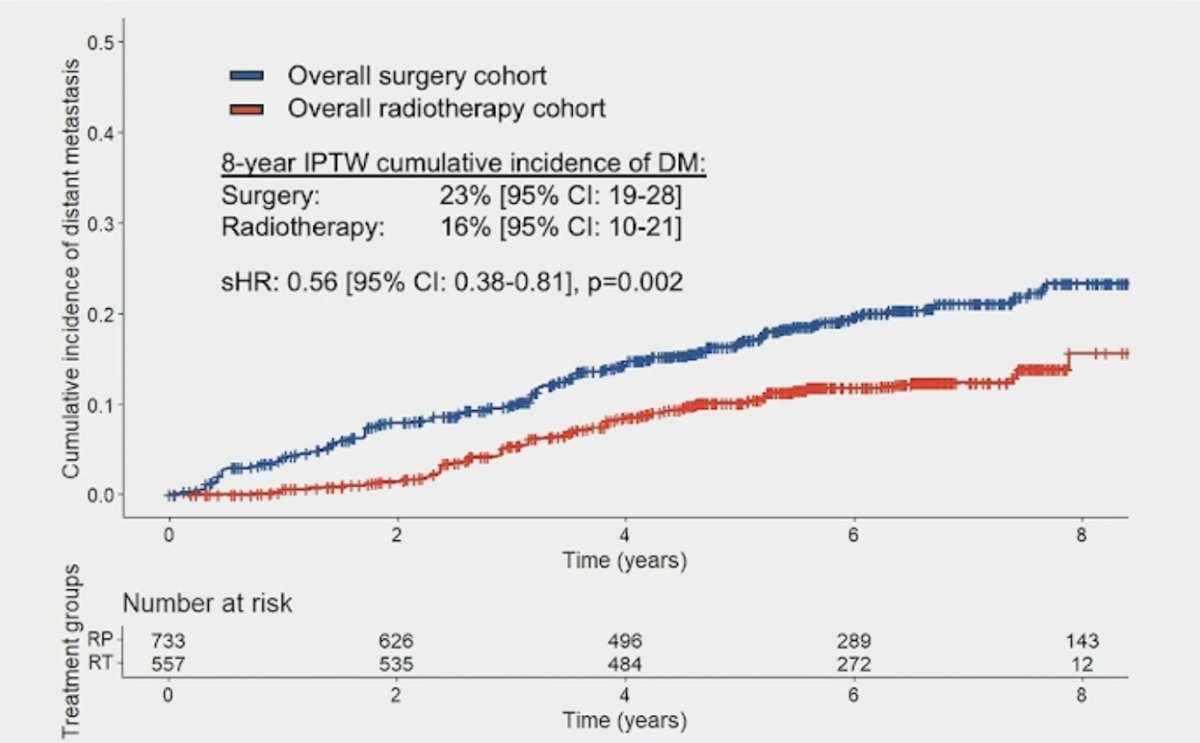
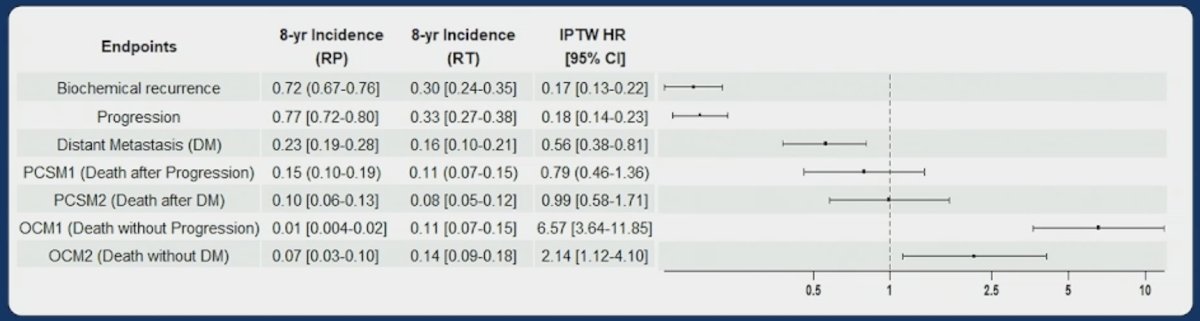
The primary endpoint of this study was distant metastasis. Cumulative incidence of distant metastasis was significantly lower in patients who underwent radiation therapy compared to radical prostatectomy (8-year IPTW cumulative incidence of distant metastasis: 16% vs 23%; subdistribution HR 0.56, 95% CI 0.38-0.81, p = 0.002):
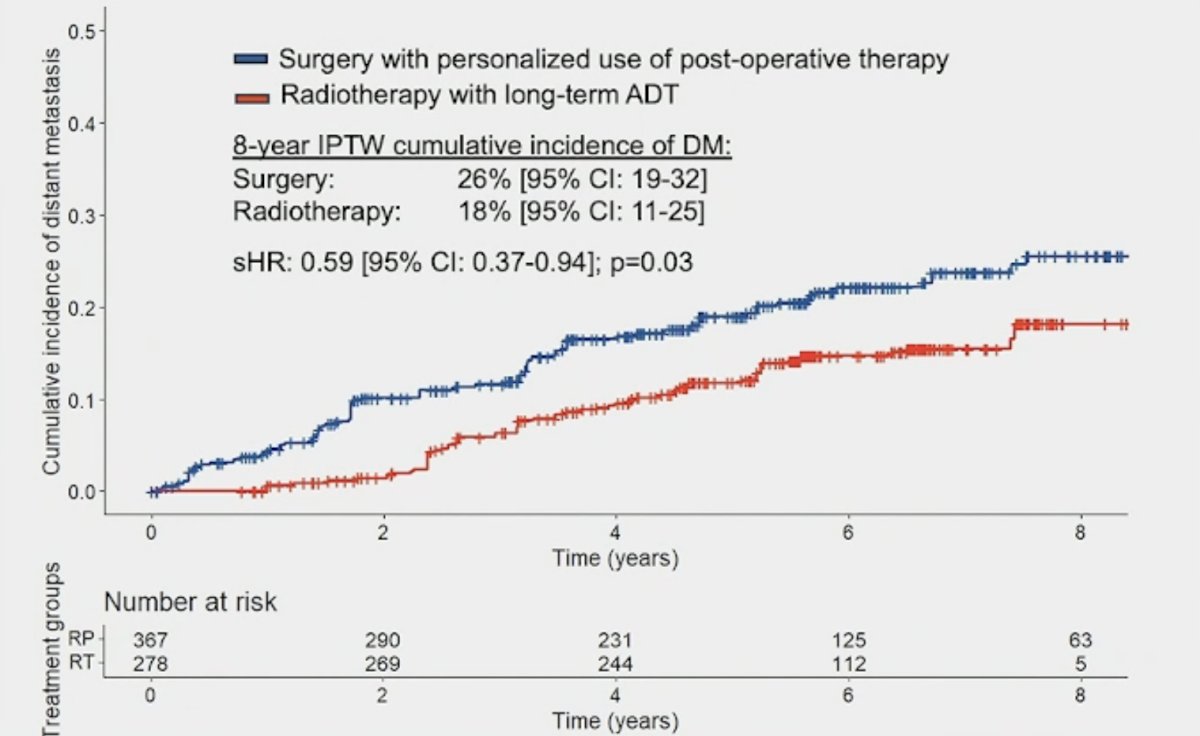
Looking at a standard of care assessment of radiation therapy + long-term ADT versus radical prostatectomy + personalized post-operative therapy also showed higher cumulative incidence of distant metastasis for the surgical cohort (8-year IPTW cumulative incidence of distant metastasis: 16% vs 26%; subdistribution HR 0.59, 95% CI 0.37-0.94, p = 0.03):
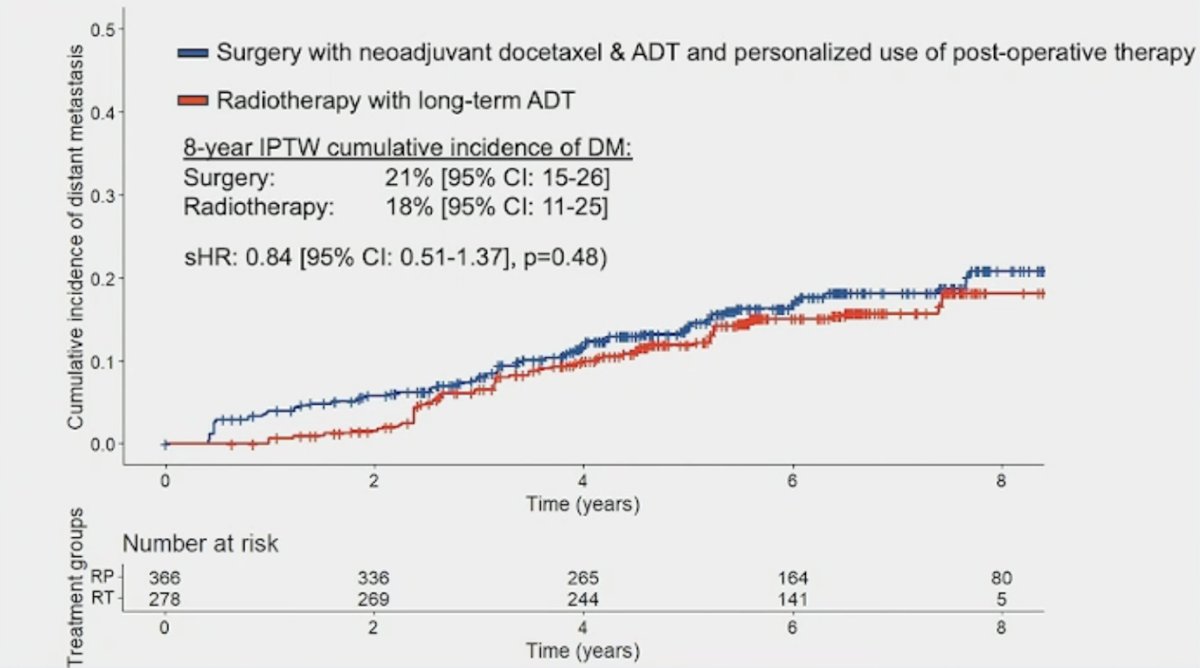
On a cross-arm comparison, 8-year cumulative incidence of distant metastasis when comparing standard of care radiation therapy + long-term ADT group versus the docetaxel + ADT + radical prostatectomy group was 18% vs 21%, respectively (subdistribution HR 0.84, 95% CI 0.51-1.37], p = 0.48):
Dr. Posadas notes that the secondary endpoints are clinically relevant and help to drive the shared decision making discussion with the patient in the clinic:
Dr. Posadas emphasized that he agrees with Dr. Roy’s robust list of limitations, highlighted as follows:
- Residual unmeasured confounding and selection bias (seen by early and large differences in overall cause mortality, as anticipated)
- Intermediate follow-up of 6.4 years, with limited prostate cancer specific mortality events
- Contemporary practice implications (PSMA PET imaging, abiraterone acetate + prednisone is now standard of care with radiotherapy in very high risk patients). He also added another limitation, notably that treatment of mHSPC has advanced significantly since these trials were enrolling patients
Dr. Roy’s conclusions to his oral abstract presentation were as follows:
- Radiotherapy-based treatment regimen appears to result in a lower incidence of distant metastasis than a surgery-based regimen for patients enrolled in phase III RCTs. Dr. Posadas states that for these studies, this appears to be true, but variations in the populations make this more of an interesting hypothesis. Secondly, he notes that although distant metastasis is important, prostate cancer specific mortality is a priority to patients and is not different.
- Approximately 80% of men with high risk prostate cancer treated with surgery will receive further treatment or experience recurrence. Adjuvant and early salvage radiotherapy remains critical for this population. Dr. Posadas agrees.
- Use of triple or quadruplet therapy of neoadjuvant chemotherapy + ADT, radical prostatectomy, and personalized post-operative radiotherapy + ADT may mitigate these differences when compared to a doublet of radiotherapy + long-term ADT. However, toxicity and cost implications require further study. Dr. Posadas agrees, given that subsequent therapy appears to impact outcomes downstream of initial treatment and its impacts need to be considered especially with more active agents now available.
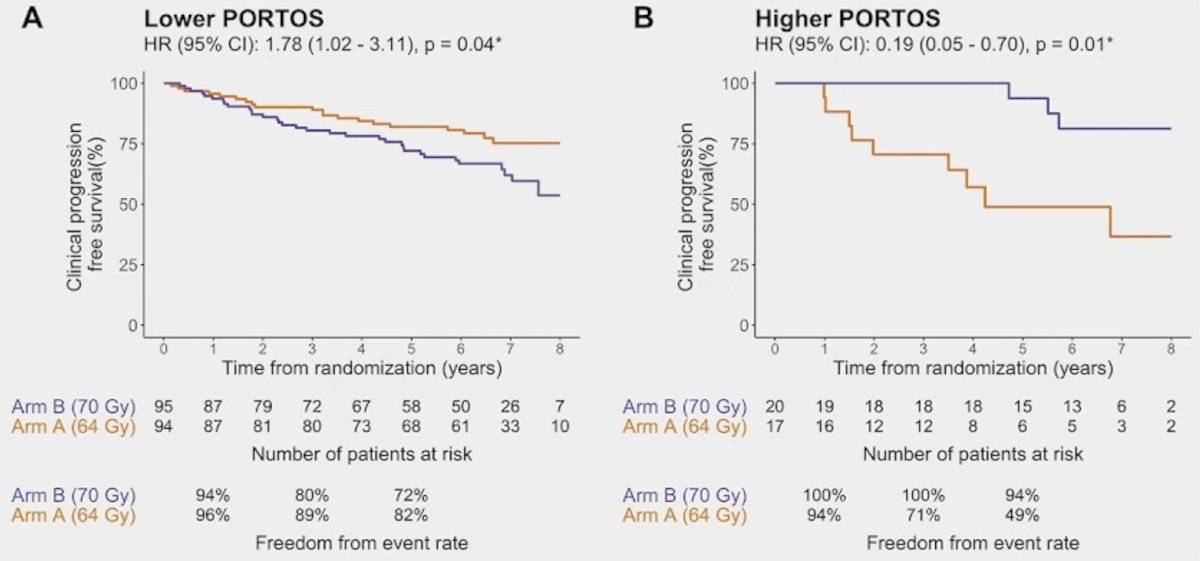
Dr. Posadas then discussed Dr. Zhao’s PORTOS validation study, noting that dose escalation in radiation therapy has been extensively studied and that it generally improves outcomes, but also increases the potential for toxicity. PORTOS appears to identify a group of patients that benefits from higher dosing. Dr. Posadas notes that Dr. Zhao’s work validates PORTOS in SAKK 09/10. In this post-op trial, only patients in the higher PORTOS score group benefited from radiation therapy dose escalation (clinical progression free survival HR 0.19, 95% CI 0.05-0.70; p = 0.01), with a significant biomarker-treatment interaction between lower versus higher PORTOS and treatment arm (p = 0.003):
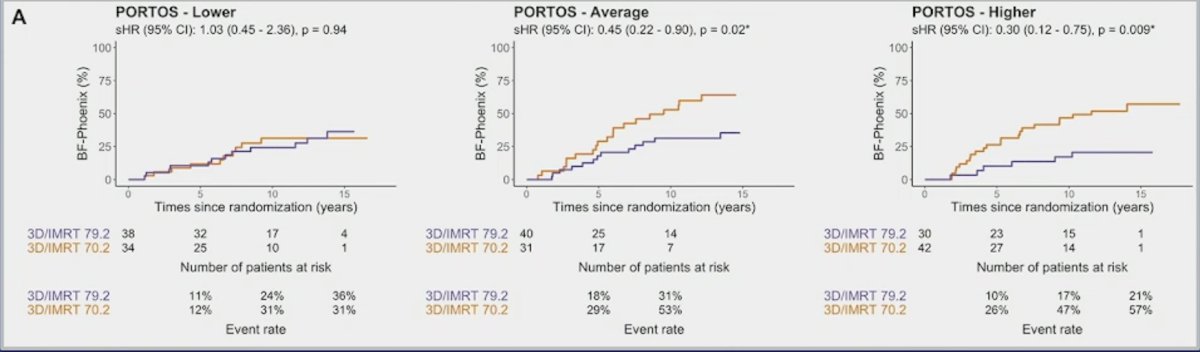
Moreover, in RTOG 0126, in patients with lower tertile PORTOS scores, there was no difference in Phoenix biochemical failure (subdistribution HR 1.03, 95% CI 0.45-2.36, p = 0.94). However, for patients in the middle and higher tertile PORTOS score range, there was a significant benefit for radiation therapy dose escalation for Phoenix biochemical failure:
- Middle PORTOS: subdistribution HR 0.45, 95% CI 0.22-0.90, p = 0.02
- Higher PORTOS: subdistribution HR 0.30, 95% CI 0.12-0.75, p = 0.009
PORTOS was not consistently associated with clinicopathologic variables in either trial or in the large real-world biopsy or prostatectomy datasets. Biologically, in the real-world datasets, PORTOS was modestly associated with hypoxia signatures consistent with its role in radio-resistance, and strongly associated with immune signatures and molecular subtypes.
Dr. Zhao’s conclusions to his oral abstract presentation were as follows:
- PORTOS predicts salvage dose response in SAKK 09/10 and predicts definitive dose response in NRG/RTOG 0126. Dr. Posadas agrees.
- PORTOS is also associated with hypoxia and immune response. Dr. Posadas agrees and notes that this opens a venue into optimizing therapeutic combinations.
- PORTOS could be used to help guide radiation dose escalation and de-escalation. Dr. Posadas thinks this may be possible, but there are also important patient variables and disease biology to consider. Further, de-escalation remains an important question for those with vulnerable disease biology.
Dr. Posadas provided the following thoughts and take away points from this discussant presentation:
- Optimizing care for patients with high risk disease that can and must be cured remains a priority in our field
- There are clear variations in outcome between surgery and radiation-based treatment but prostate cancer specific survival remains similar
- Emerging biomarkers may help to better empower decision making in the near future
- Multimodal care for these patients strongly impacts outcomes
- Molecular information is becoming more and more important in delivering optimal care to patients with prostate cancer, even with early disease
- Emerging biomarkers such as PORTOS may help optimize selection and dosing for patients
- Patient factors are still present that impact toxicity outcomes and must be considered
- It will be important to see how PORTOS interacts with systemic treatments
- Additional strategies are underway in this space and require support for patients and investigators
Presented by: Edwin M. Posadas, MD, Cedars-Sinai Medical Center, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:
- Eastham JA, Heller G, Halabi S, et al. Cancer and Leukemia Group B 90203 (Alliance): Radical Prostatectomy With or Without Neoadjuvant Chemohormonal Therapy in Localized, High-Risk Prostate Cancer. J Clin Oncol. 2020 Sep 10;38(26)3042-3050.
- Rosenthal SA, Rodrigues GB, Sartor O, et al. Effect of chemotherapy with docetaxel with androgen suppression and radiotherapy for localized high-risk prostate cancer: The Randomized Phase III NRG Oncology RTOG 0521 Trial. J Clin Oncol. 2019 May 10;37(14):1159-168.
- Sartor O, Karrison TG, Sandler HM, et al. Androgen deprivation and radiotherapy with or without docetaxel for localized high-risk prostate cancer: Long-term follow-up from the randomized NRG Oncology RTOG 0521 Trial. Eur Urol. 2023 Aug;84(2):156-163.
Related Content:
ASCO GU 2025: Gene Signature Predictor of Dose-response to Prostate Radiation: Validation of PORTOS in Phase III Trials
ASCO GU 2025: Radical Prostatectomy Versus Radiotherapy in High-Risk Prostate Cancer: Emulated Randomized Comparison with Individual Patient Data from Two Phase III Randomized Trials.
Radiation Therapy vs Surgery Outcomes in High-Risk Localized Prostate Cancer Patients - Soumyajit Roy