(UroToday.com) The 2025 GU ASCO annual meeting featured a urothelial carcinoma session and a discussant presentation by Dr. Elizabeth Plimack discussing two abstracts: “Adjuvant nivolumab vs placebo for high-risk muscle-invasive urothelial carcinoma: Additional efficacy outcomes including overall survival in patients with muscle-invasive bladder cancer from CheckMate 274” by Dr. Matthew Milowsky, and “Additional efficacy and safety outcomes and an exploratory analysis of the impact of pathological complete response on long-term outcomes from NIAGARA” by Dr. Matthew Galsky.
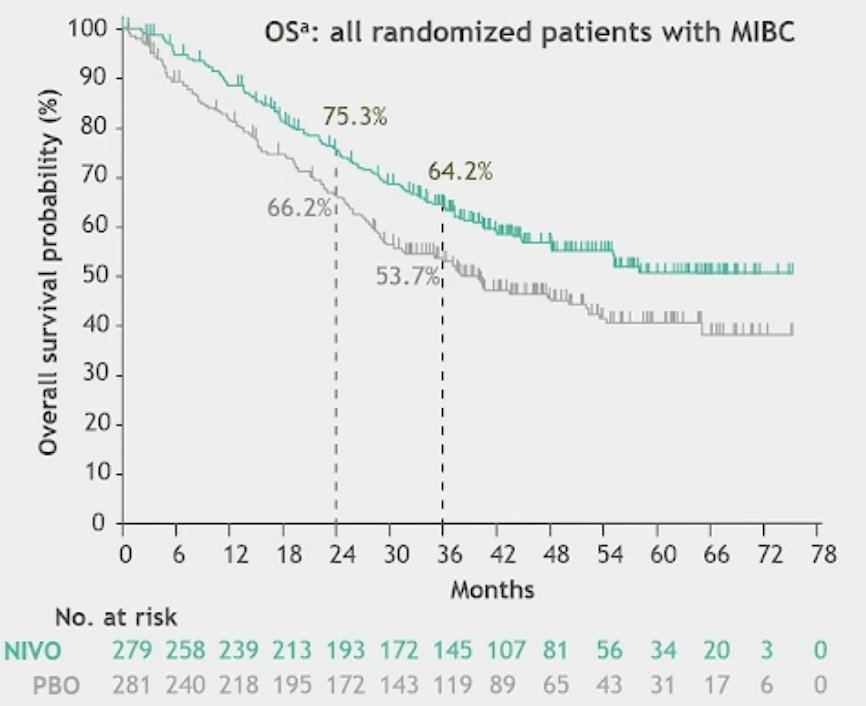
Dr. Plimack started her discussion by emphasizing that in the most recent update of Checkmate 274 we now know that there is a clear overall survival benefit with nivolumab versus placebo, with an absolute event free survival benefit at 3 years of 15% and an absolute overall survival benefit at 3 years of 11% in patients with muscle invasive bladder cancer:
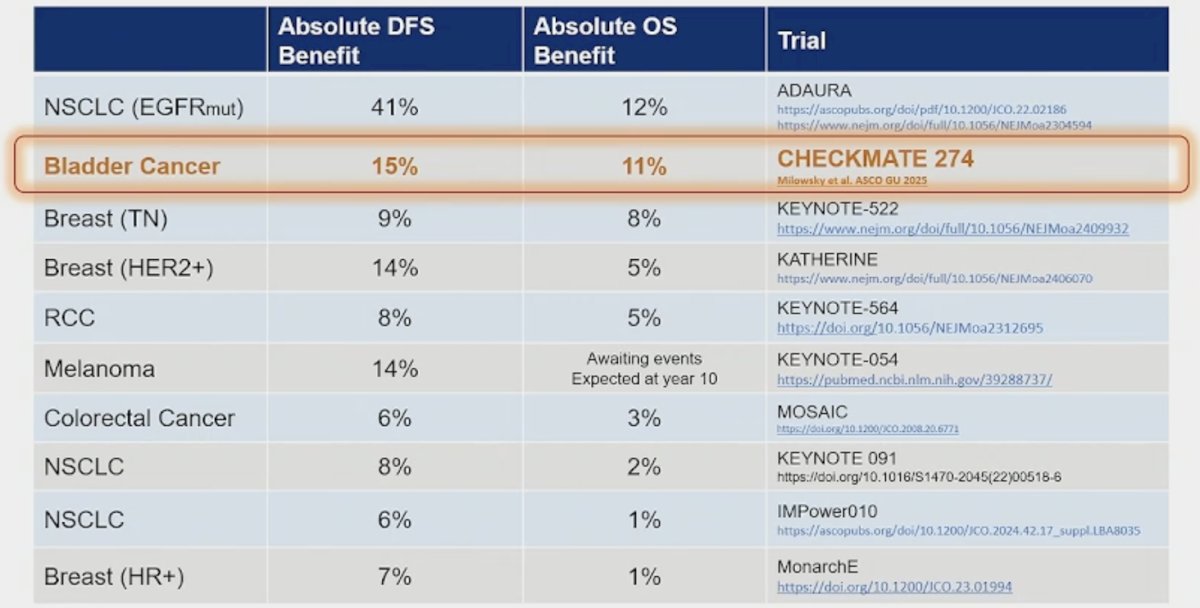
Moreover, when we compare adjuvant regimens in cancer (intention to treat versus placebo), nivolumab in muscle invasive bladder cancer compares favorably:
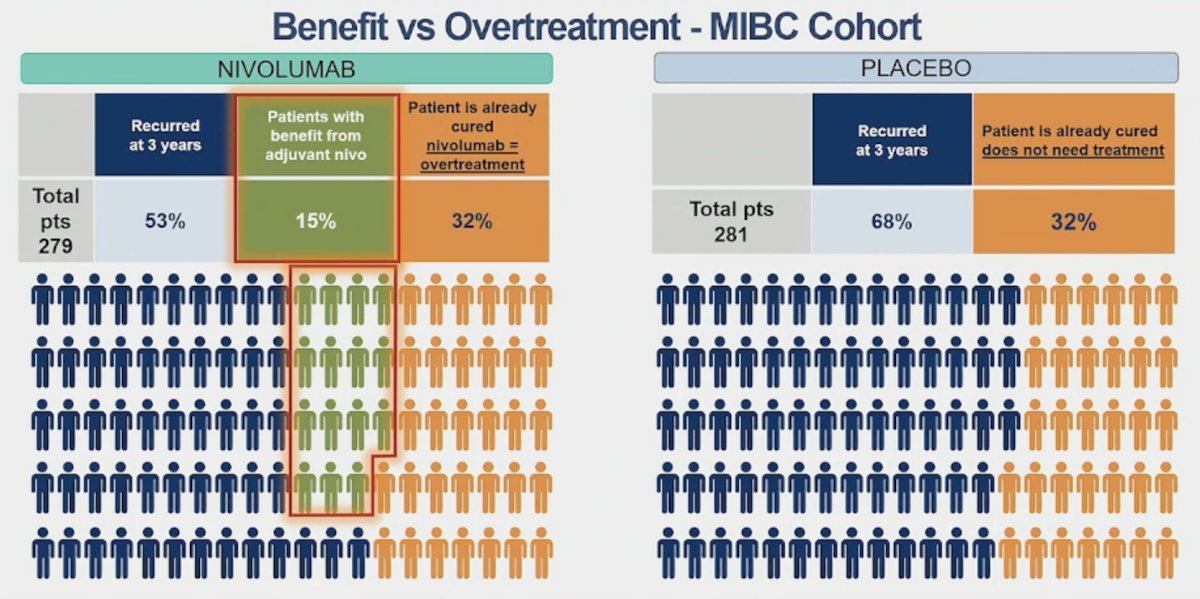
However, like for any adjuvant therapy, it is always important to assess risk of overtreatment for those already cured of disease, and risk of under-treatment of those that should have further treatment intensification, and ultimately identify those who are most likely to benefit from adjuvant nivolumab:
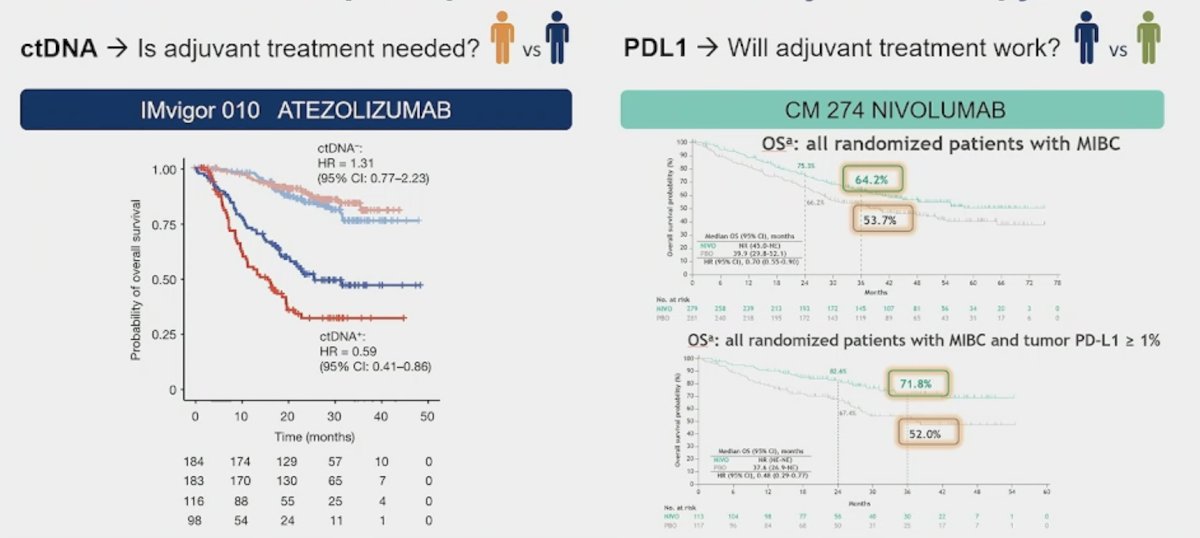
Can biomarkers improve patient selection for adjuvant therapy? From the negative IMvigor 010 trial of adjuvant atezolizumab [1] we know that ctDNA can tell us whether adjuvant treatment is needed, and from the CheckMate 274 trial [2-3], we know that PD-L1 status can tell us whether adjuvant treatment will work:
Dr. Plimack highlighted the risk adapted adjuvant therapy trial MODERN, which is seeking to answer whether dose escalation (adding relatilimab) can improve overall survival if ctDNA is positive? And, does nivolumab provide any disease free survival benefit in ctDNA negative patients? To date, this trial has accrued 93 of 1,190 patients:

The setting of overall survival with adjuvant nivolumab in CheckMate 274 in the context of subsequent therapy is an important question. In this trial, only 8.8% of patients in the nivolumab arm received a subsequent immunotherapy, whereas 26.1% did so in the placebo arm. Given this data, it important to understand that few, if any, patients in CheckMate 274 who progressed after nivolumab would have access to enfortumab vedotin + pembrolizumab as first line standard of care therapy for metastatic urothelial carcinoma.4
Adjuvant nivolumab improved overall survival for patients with muscle invasive bladder cancer with (HR 0.74, 95% CI 0.53-1.03) and without prior neoadjuvant chemotherapy (HR 0.67, 95% CI 0.47-0.95):

However, Dr. Plimack questions why half of enrolled patients did not get neoadjuvant chemotherapy as standard of care therapy? General reasons for not receiving neoadjuvant chemotherapy include (i) the patient is unfit for cisplatin, (ii) the patient is understaged as T1 and upstaged at surgery, and (iii) neoadjuvant chemotherapy was not offered (which is not standard of care).
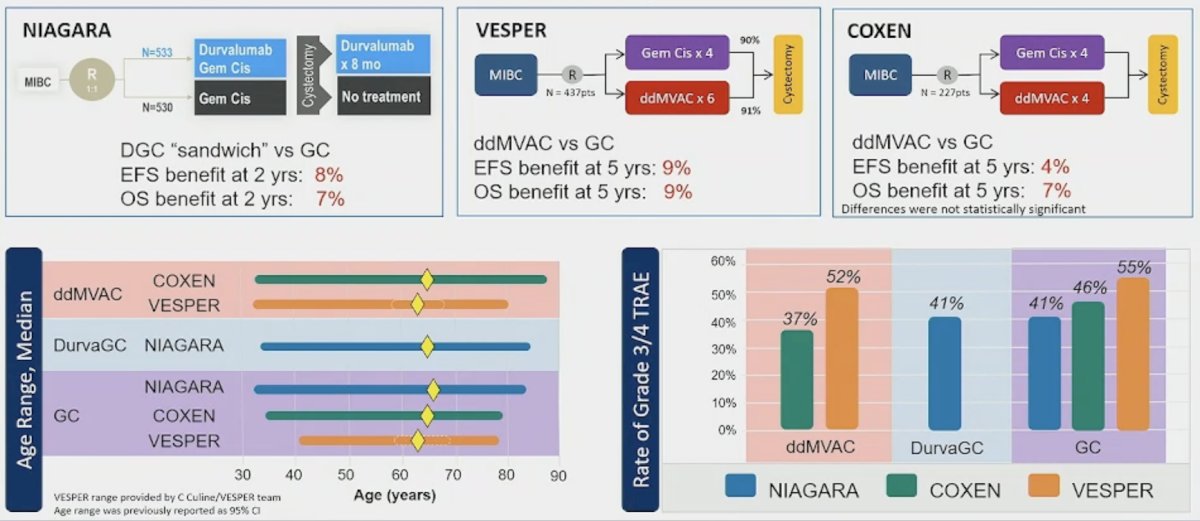
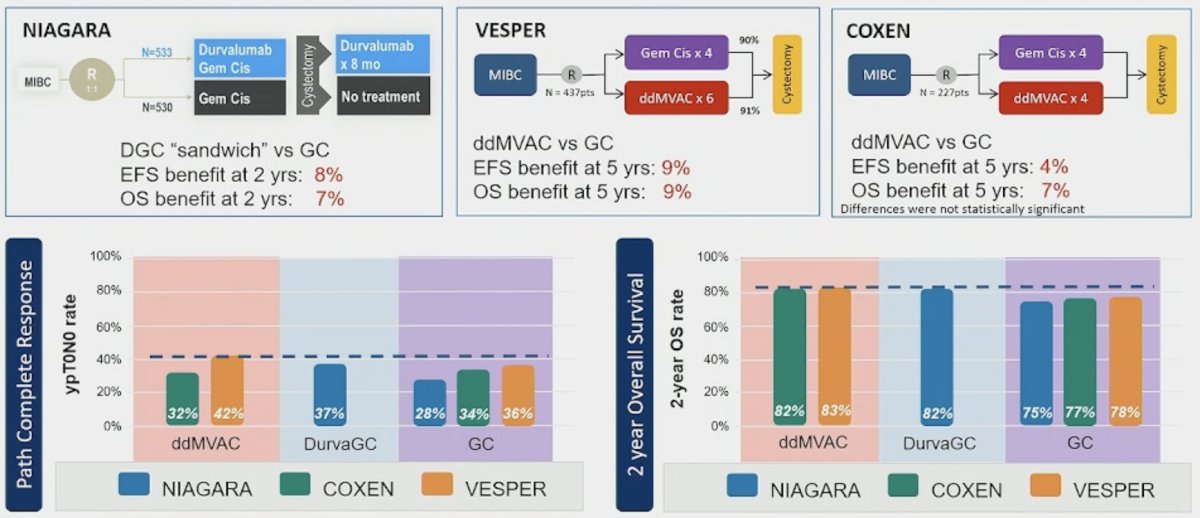
Dr. Plimack then discussed the NIAGARA updated analysis, the approach which she calls “sandwich” perioperative chemoimmunotherapy for muscle invasive bladder cancer. She notes that it is important to understand that for checkpoint inhibitors, persistent PD1 receptor occupancy suggests that the effects of neoadjuvant chemotherapy extend into the adjuvant period even without adjuvant dosing. Moreover, the NIAGARA control arm does not reflect the current standard of care. Few patients in the control arm would have had access to adjuvant nivolumab, which became standard of care in 2021. Additionally, VESPER [5] and COXEN [6] overall survival data were published in 2023, after NIAGARA fully accrued. The following two figures place NIAGARA in the context of currently available treatment options:
In NIAGARA, patients in the durvalumab arm derived greater overall survival benefit versus the comparator arm in both pathologic complete response (HR 0.72, 95% CI 0.37-1.43) and non-pathologic complete response (HR 0.84, 95% CI 0.66-1.07) groups:
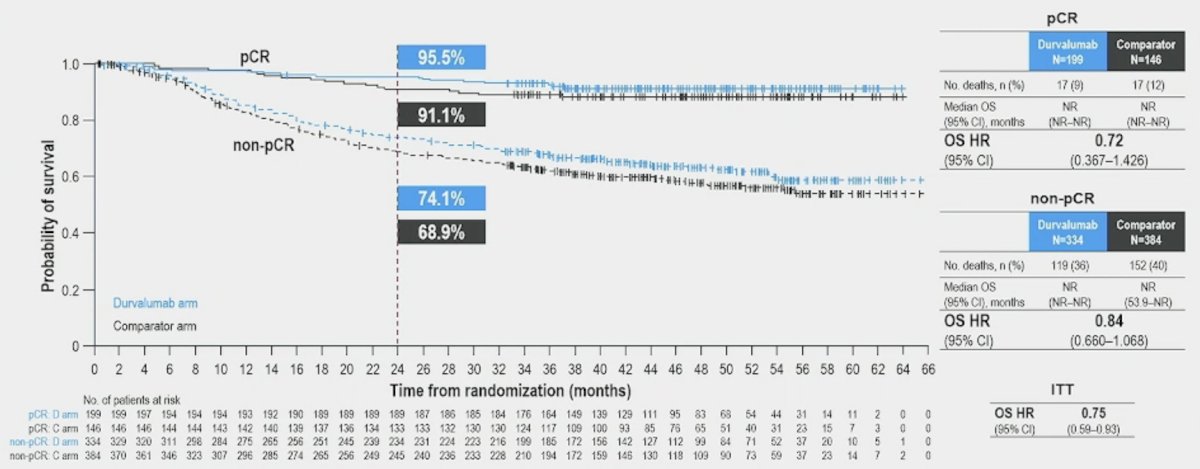
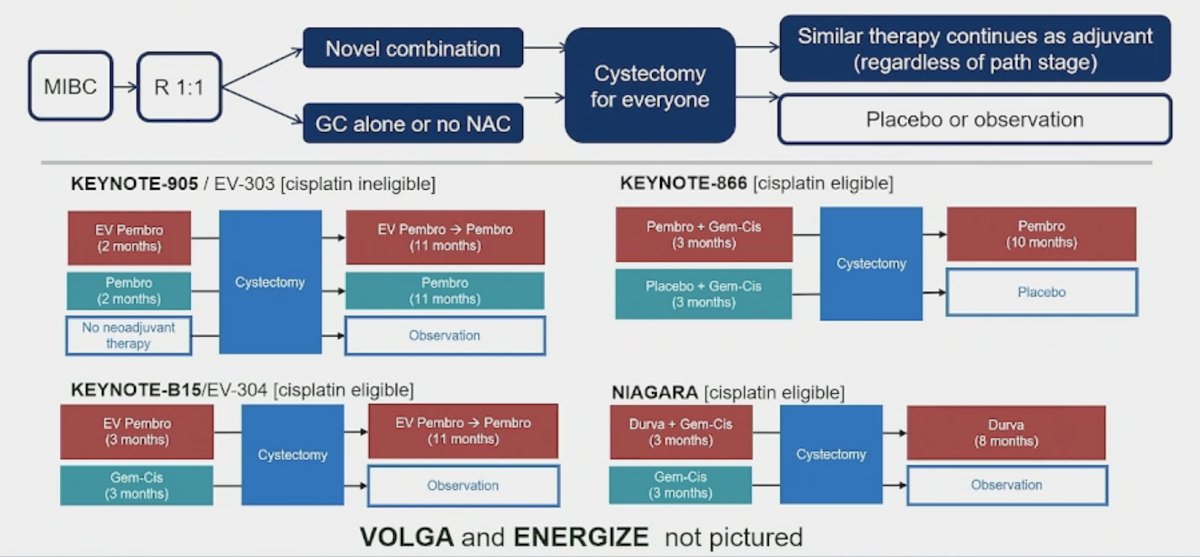
This corresponds to an absolute 2 year overall survival benefit in the pathologic complete response group of 4%, and as such should not be extrapolated to support the contribution of the adjuvant component. This benefit may all be from durable receptor occupancy, or more durable IO response to the neoadjuvant component compared with gemcitabine + cisplatin alone. Given the sandwich trial design, the adjuvant phase may add financial toxicity, time toxicity, and side effect toxicity and must be justified by showing added benefit. Currently, there are 6 ongoing phase III muscle invasive bladder cancer trials using the sandwich approach, of which we will be unsure of the contribution from the neoadjuvant and adjuvant components of treatment:
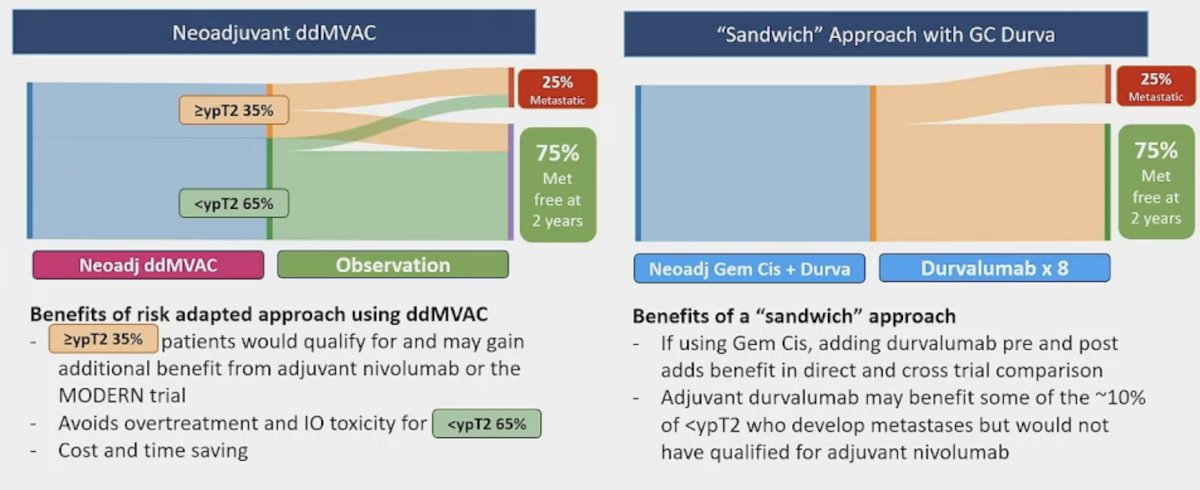
Dr. Plimack notes that there are two options to take with us to the clinic on Monday: the neoadjuvant dose dense MVAC approach or the “sandwich” approach with gemcitabine + cisplatin and durvalumab:
Dr. Plimack concluded her discussant presentation with the following take-home points:
- Adjuvant nivolumab for high risk muscle invasive bladder cancer demonstrates a significant overall survival and event free survival benefit and is standard of care in this disease space
- Biomarkers (ctDNA and PD1) may help us select who needs adjuvant immunotherapy, and of those who need it, who is likely to benefit
- Neoadjuvant therapy is still standard of care, with or without immunotherapy, and uptake needs to improve
- “Sandwich” immunochemotherapy is effective per NIAGARA, but may be over treatment, as a sandwich study design does not clarify the contribution of neoadjuvant and adjuvant components
- Neoadjuvant chemotherapy with risk adapted adjuvant immunotherapy can achieve similar efficacy to a sandwich approach, with less overtreatment
Presented by: Elizabeth R. Plimack, MD, Fox Chase Cancer Center, Temple Health, Philadelphia, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:
- Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021 Jl;595(7867):432-437.
- Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021 Jun 3;384(22):2102-2114.
- Galsky MD, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab in high-risk muscle-invasive urothelial carcinoma: Expanded efficacy from CheckMate 274. J Clin Oncol. 2025 Jan;43(1):15-21.
- Powles T, Valderrama BP, Gupta S, et al. Enfortumab Vedotin and Pembrolizumab in Untreated Advanced Urothelial Cancer. N Engl J Med. 2024 Mar 7;390(10)875-888.
- Pfister C, Gravis G, Flechon A, et al. Perioperative dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin in muscle-invasive bladder cancer (VESPER): Survival endpoints at 5 years in an open-label, randomized, phase 3 trial. Lancet Oncol. 2024 Feb;25(2):255-264.
- Flaig TW, Tangen CM, Daneshmand S, et al. Long-term outcomes from a phase 2 study of neoadjuvant chemotherapy for muscle-invasive bladder cancer (SWOG S1314; NCT02177695). Eur Urol. 2023 Sep;84(3):341-347.
Related Content:
ASCO GU 2025: Additional Efficacy and Safety Outcomes and an Exploratory Analysis of the Impact of Pathological Complete Response on Long-Term Outcomes from NIAGARA
ASCO GU 2025: Adjuvant Nivolumab vs Placebo for High-Risk Muscle-Invasive Urothelial Carcinoma: Additional Efficacy Outcomes Including Overall Survival in Patients with MIBC from CheckMate 274