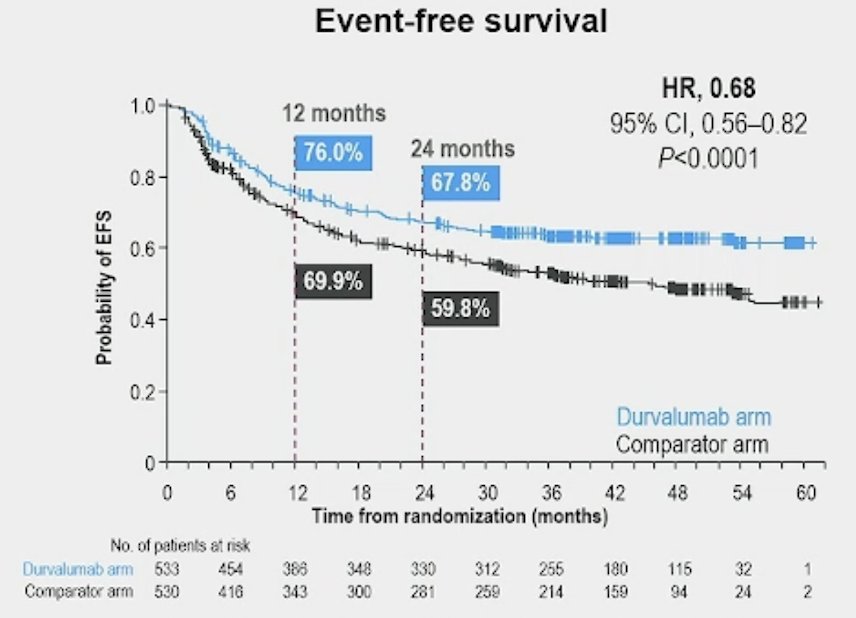
(UroToday.com) The 2025 GU ASCO annual meeting featured a urothelial carcinoma session and a presentation by Dr. Matthew Galsky discussing additional efficacy and safety outcomes and an exploratory analysis of the impact of pathological complete response on long-term outcomes from NIAGARA. In the phase 3 NIAGARA study of patients with muscle-invasive bladder cancer, perioperative durvalumab plus neoadjuvant chemotherapy demonstrated a statistically significant and clinically meaningful improvement in event free survival (HR 0.68, 95% CI 0.56-0.82) and overall survival (HR 0.75, 95% CI 0.59-0.93) compared with neoadjuvant chemotherapy alone, with a manageable safety profile and no detriment to the ability to undergo radical cystectomy1:
Additionally, there was a 10% improvement in pathological complete response rate, no delay to surgery, and no impact on a patient’s ability to undergo/complete surgery. At the GU ASCO 2025 annual meeting Dr. Galsky and colleagues presented additional outcomes and an exploratory analysis from NIAGARA.
NIAGARA enrolled cisplatin-eligible patients with muscle-invasive bladder cancer (cT2-T4aN0/1M0) planned for radical cystectomy. Patients were randomized 1:1 to receive either neoadjuvant durvalumab (1500 mg IV Q3W) and neoadjuvant chemotherapy (cisplatin + gemcitabine IV Q3W) for 4 cycles followed by radical cystectomy, then adjuvant durvalumab monotherapy (1500 mg IV Q4W) for 8 cycles (durvalumab arm), or neoadjuvant chemotherapy followed by radical cystectomy alone (comparator arm):
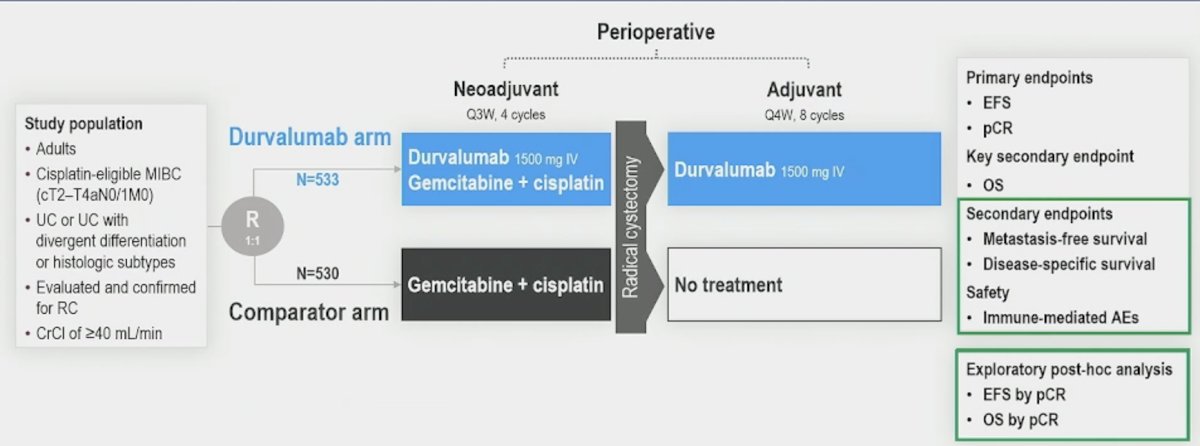
Dual primary endpoints were event-free survival and pathologic complete response and overall survival was a key secondary endpoint, as well as metastasis free survival and disease-specific survival. An exploratory post hoc analysis of event free survival and overall survival in patients with pathologic complete response versus those without pathologic complete response was also performed. Efficacy analyses were conducted in the intent-to-treat population (data cutoff April 2024).
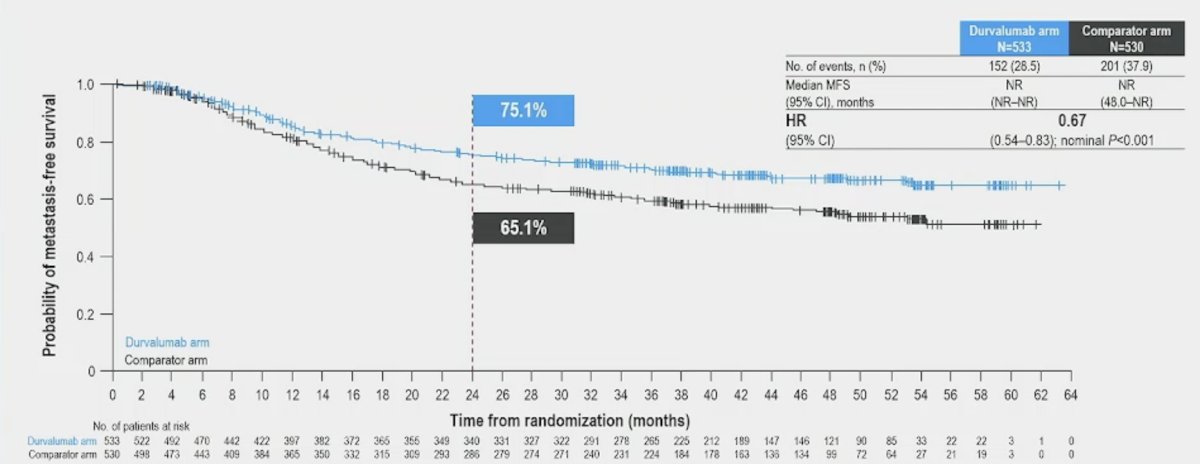
A total of 1,063 patients were randomized (533 durvalumab arm; 530 comparator arm). Patients in the durvalumab arm had a 33% reduction in risk of developing distant metastases or death (HR 0.67; 95% CI 0.54–0.83; nominal p < 0.001):
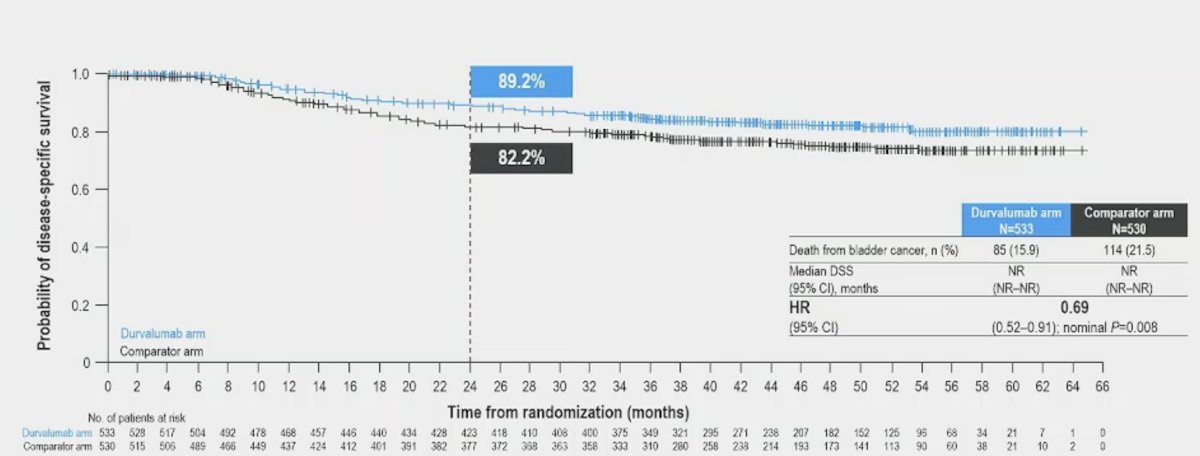
Additionally, the durvalumab arm led to a 31% reduction in risk of death from bladder cancer (HR 0.69; 95% CI 0.52–0.91; nominal p = 0.008) vs patients in the comparator arm:
More patients in the durvalumab versus comparator arm had pathologic complete response at radical cystectomy (37.3% versus 27.5%; OR 1.60, 95% CI 1.23-2.08). The patient characteristics as stratified by pathologic complete response versus non-pathologic complete response are highlighted as follows:

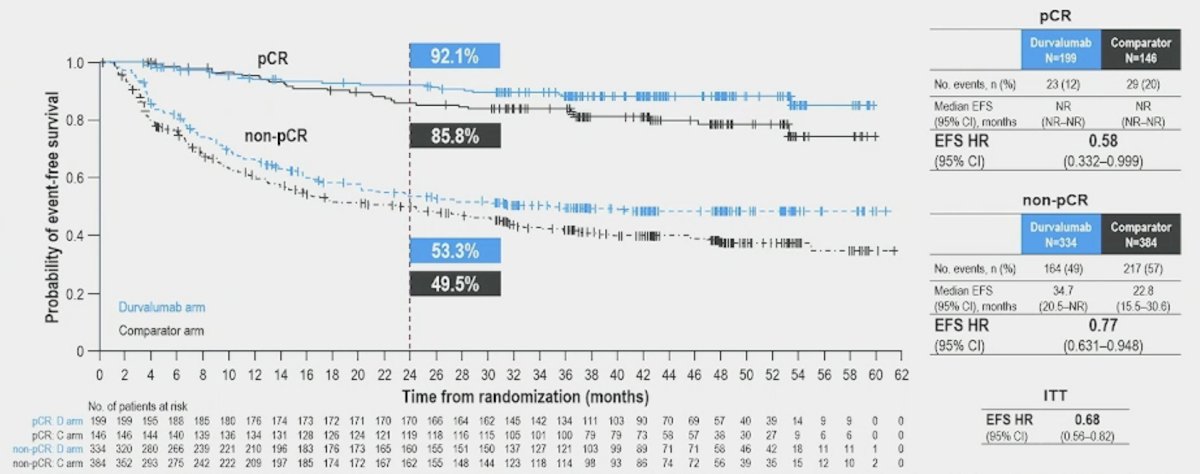
Patients in the durvalumab arm derived greater event-free survival benefit versus the comparator arm in both pathologic complete response (HR 0.58, 95% CI 0.33-0.99) and non-pathologic complete response (HR 0.77, 95% CI 0.63-0.95) groups:
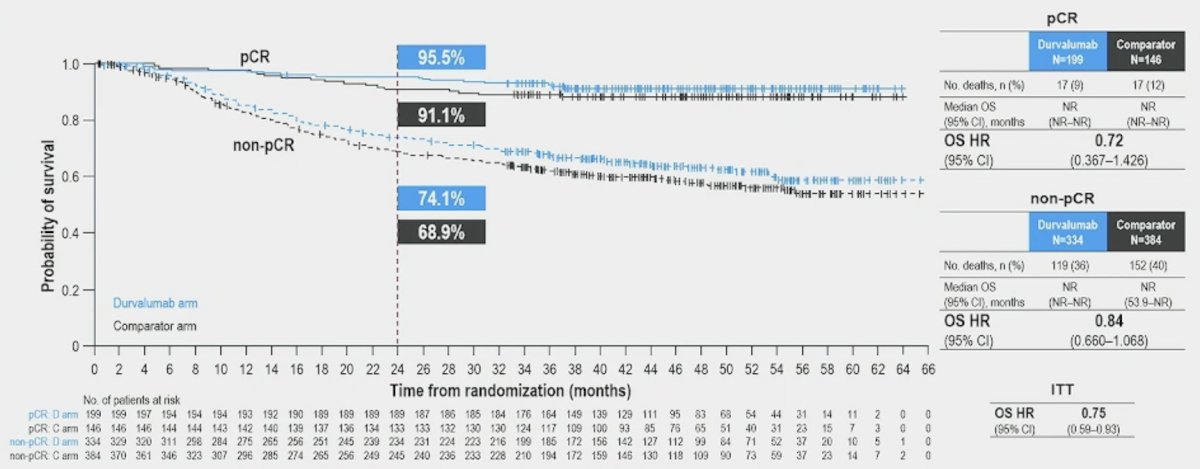
Additionally, patients in the durvalumab arm derived greater overall survival benefit versus the comparator arm in both pathologic complete response (HR 0.72, 95% CI 0.37-1.43) and non-pathologic complete response (HR 0.84, 95% CI 0.66-1.07) groups:
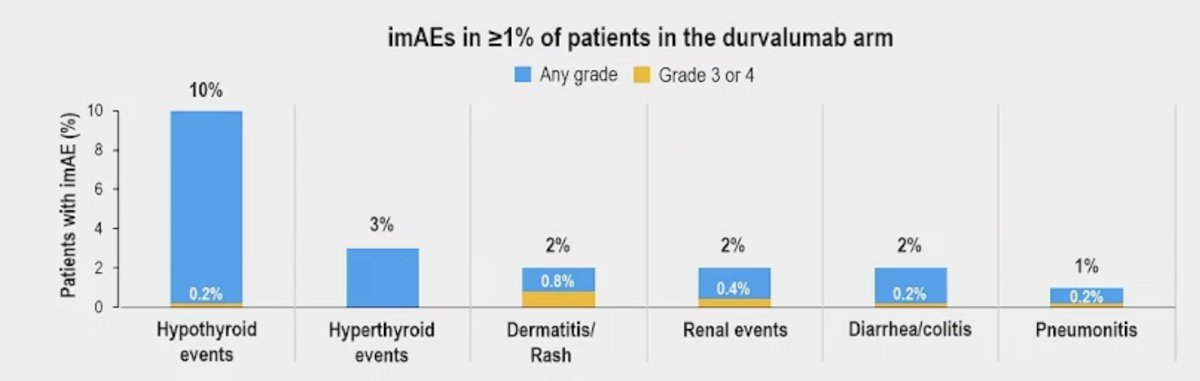
Overall, immune-mediated adverse events were reported in 111/530 (21%) patients in the durvalumab arm (grade 3/4 3%) and 16/526 (3%) in the comparator arm (grade 3/4 0.2%). At data cutoff, all immune-mediated adverse events were resolved for 45/111 (41%) patients (durvalumab arm) and 7/16 (44%) patients (comparator arm). The most common immune-mediated adverse events were hypothyroid events (10% durvalumab arm; 1% comparator arm) and hyperthyroid events (3% durvalumab arm; 0.8% comparator arm):
Dr. Galsky concluded his presentation by discussing additional efficacy and safety outcomes and an exploratory analysis of the impact of pathological complete response on long-term outcomes from NIAGARA with the following take-home points:
- NIAGARA demonstrated a statistically and clinically meaningful improvement in event free survival (HR 0.68, 95% CI 0.56-0.82) and overall survival (HR 0.75, 95% CI 0.59-0.93) with a 10% improvement in pathologic complete response rate
- In the durvalumab arm, the risk of metastasis free survival was reduced by 33% and the risk of a disease specific survival event was reduced by 31%
- Perioperative durvalumab + neoadjuvant chemotherapy improved event free survival and overall survival in both the pathologic complete response and non-pathologic complete response groups in an exploratory analysis
- Immune mediate adverse events were mostly low grade and consistent with the known profile of durvalumab
- This additional NIAGARA data further supports perioperative durvalumab with neoadjuvant chemotherapy as a potential new treatment for patients with cisplatin-eligible muscle invasive bladder cancer
Presented by: Matthew D. Galsky, MD, Icahn School of Medicine at Mount Sinai, New York, NY
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
Related content: The NIAGARA Trial Highlights the Role of Durvalumab in Bladder Cancer Treatment - Matthew Galsky
References: