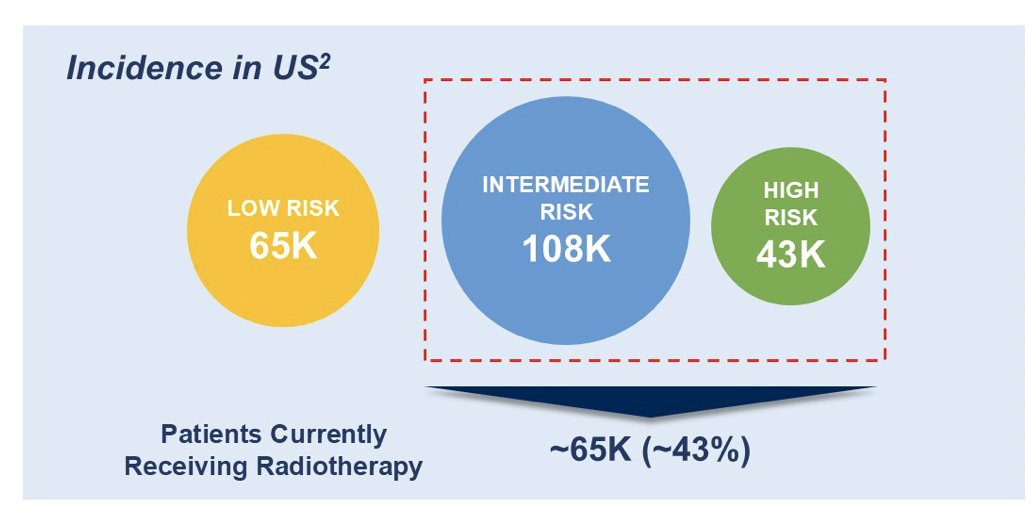
(UroToday.com) The 2025 ASCO annual meeting featured a prostate cancer oral abstract session and a presentation by Dr. Theodore DeWeese discussing a phase 3, randomized, placebo-controlled clinical trial of CAN-2409 + Prodrug in combination with standard of care external beam radiation for newly diagnosed localized prostate cancer. There is currently an unmet need in localized prostate cancer, with approximately 1.4 million new cases of prostate cancer in 2020 globally. The following figure shows the incidence in the United States:
The ultimate goal of curative treatment is prevention of cancer recurrence, while minimizing treatment-related side effects and maintaining quality of life. Standard of care for intermediate to high-risk localized prostate cancer includes surgery or external beam radiation +/- ADT. However, nearly 30% of men undergoing external beam radiation will experience recurrence requiring ADT and salvage therapies that negatively impact quality of life. CAN-2409 is a replication-defective adenovirus encoding the HSV-tk gene that, when combined with valacyclovir (Prodrug), results in immunogenic cell death: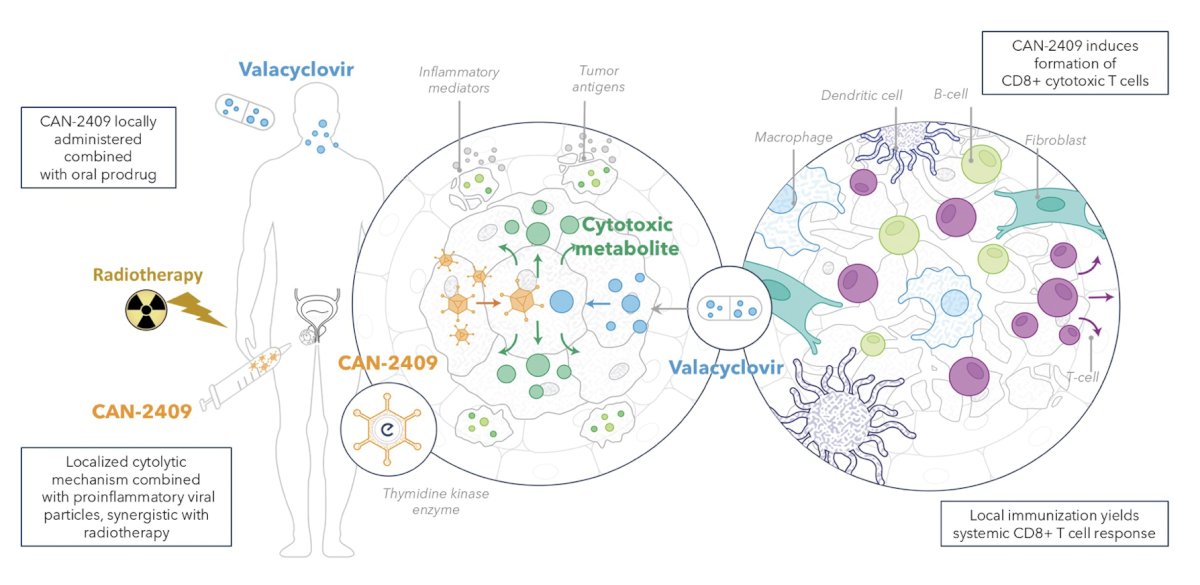
This results in immunization against tumor antigens and long-term tumor control.
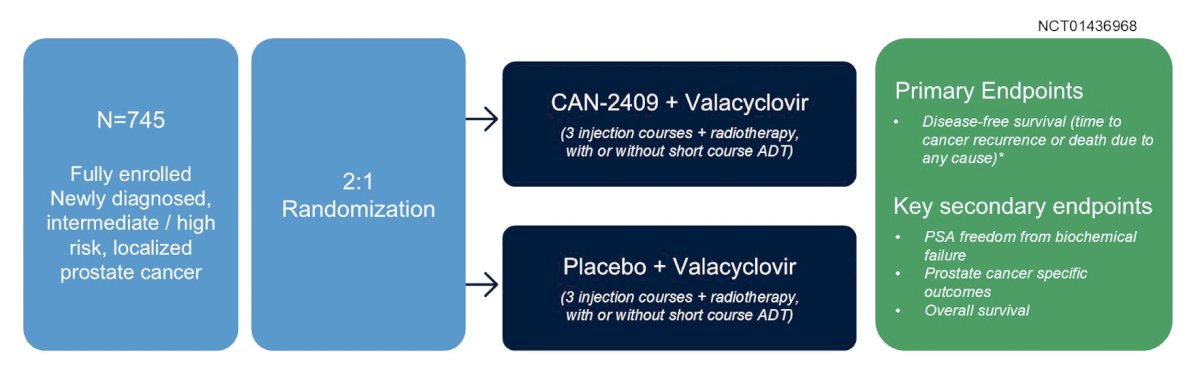
Dr. DeWeese and colleagues conducted a phase 3, multicenter, double-blinded, randomized, placebo-controlled clinical trial in prostate cancer patients planning to receive external beam radiation +/- short course ADT (<6 months) (NCT01436968). There were 745 patients randomized 2:1 (496 in CAN-2409 + Prodrug and 249 in placebo + Prodrug) and stratified by NCCN risk group and ADT use. The trial design is as follows:
Three intraprostatic injections of CAN-2409 (5x10 11v/2mL) or placebo were administered, each followed by 14 days of Prodrug. The following figure shows the standard urologic injection procedure via transrectal or transperineal ultrasound guidance (performed by urologists or radiation oncologists):

Follow-up included a prostate biopsy 2 years after external beam radiation. The primary endpoint was disease free survival, defined as time from randomization to prostate cancer recurrence (local/regional failure or distant metastasis) or death in the intent-to-treat population. Median follow up time was 50.3 months.
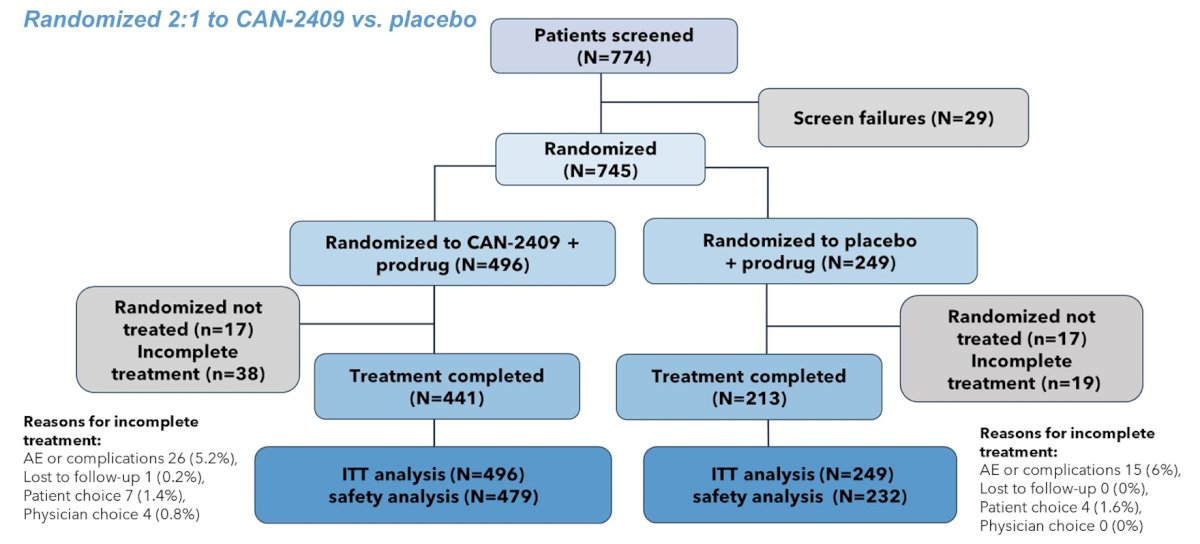
The consort diagram shows that 774 patients were screened for this trial with the following breakdown:
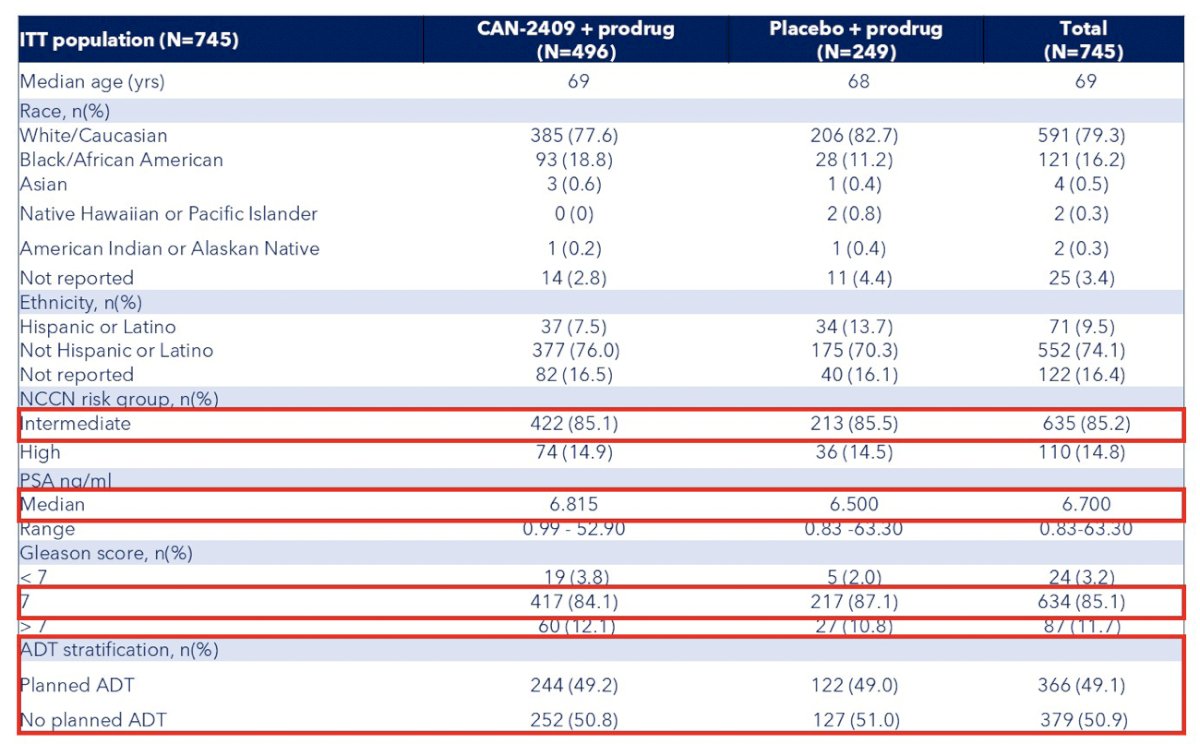
The baseline characteristics of randomized patients were well balanced between the two groups:
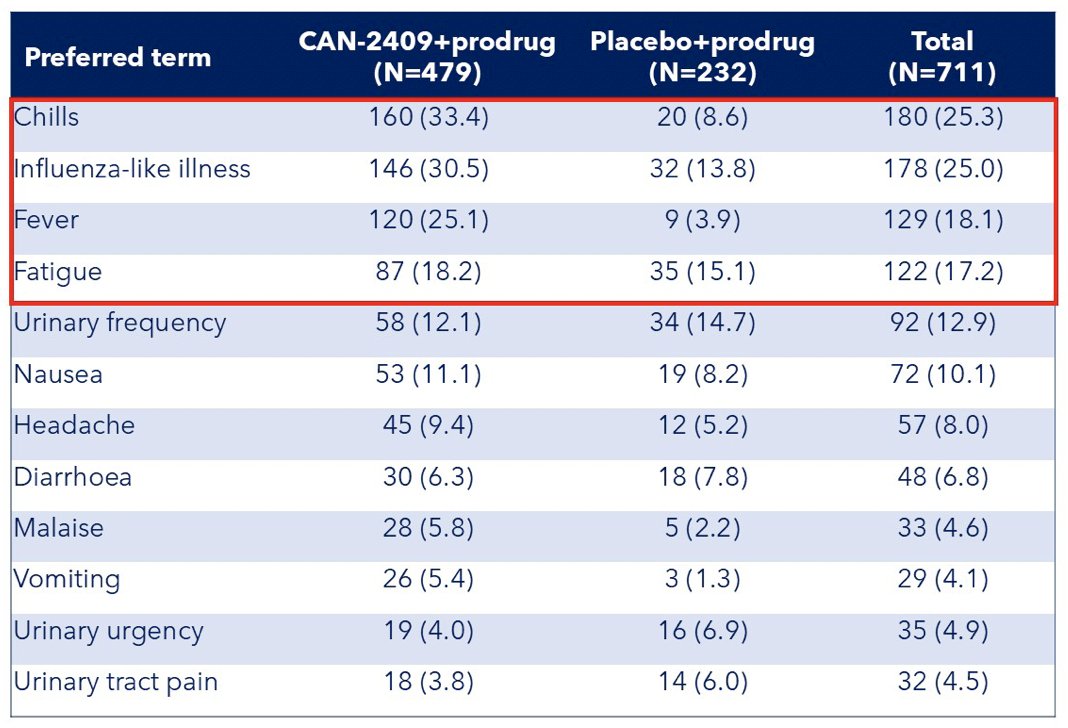
The most common treatment-related adverse events included chills (33.4% versus 8.6%), flu-like symptoms (30.5% versus 13.8%), and fever (25.1% versus 3.9%), mostly grade 1-2 and self-limited. Serious adverse events (5.8% versus 7.3%) and treatment-related serious adverse events (1.7% versus 2.2%) were uncommon across treatment groups:
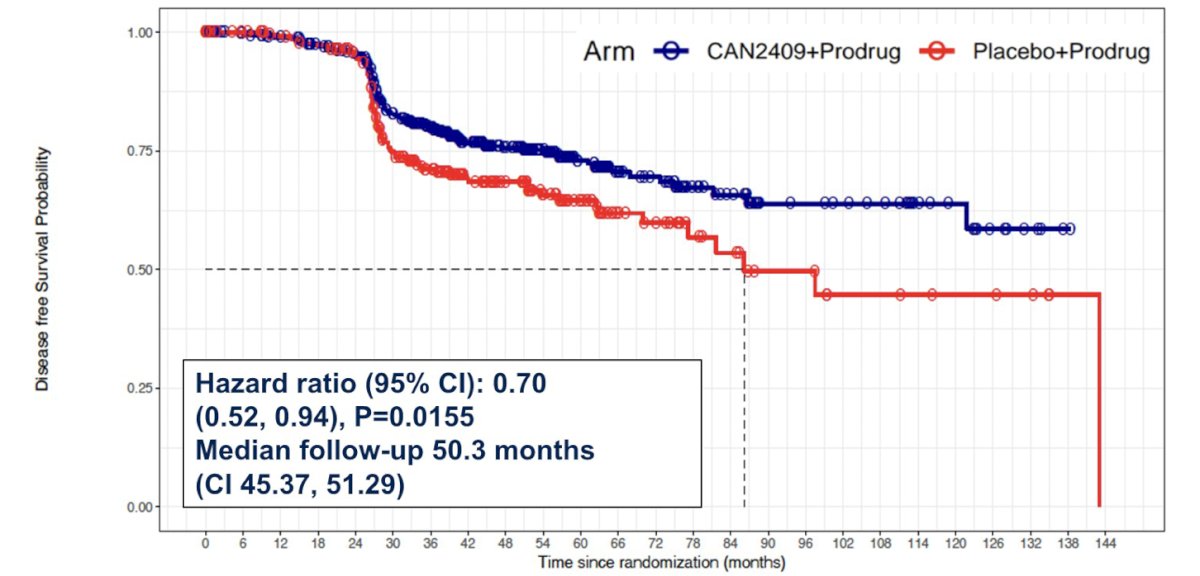
Treatment with CAN-2409 reduced the risk of prostate cancer recurrence or death by 30% (median disease free survival not reached versus 86.1 months, p = 0.0155, HR 0.70, 95% CI 0.52 to 0.94):
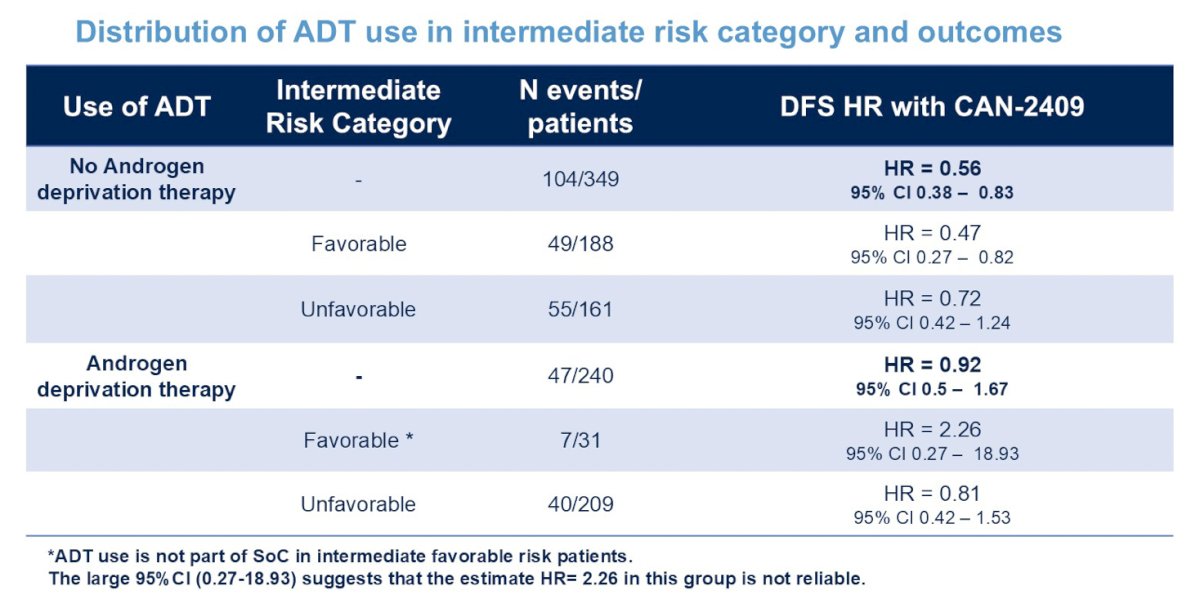
The following shows disease free survival outcomes stratified by use of short-term ADT:
Prostate cancer-specific disease free survival (exclusion of non prostate cancer- related deaths) demonstrated an even greater effect with a 38% decreased risk in the CAN-2409 arm versus placebo (p = 0.0046; HR 0.62, 95% CI 0.44 to 0.87):
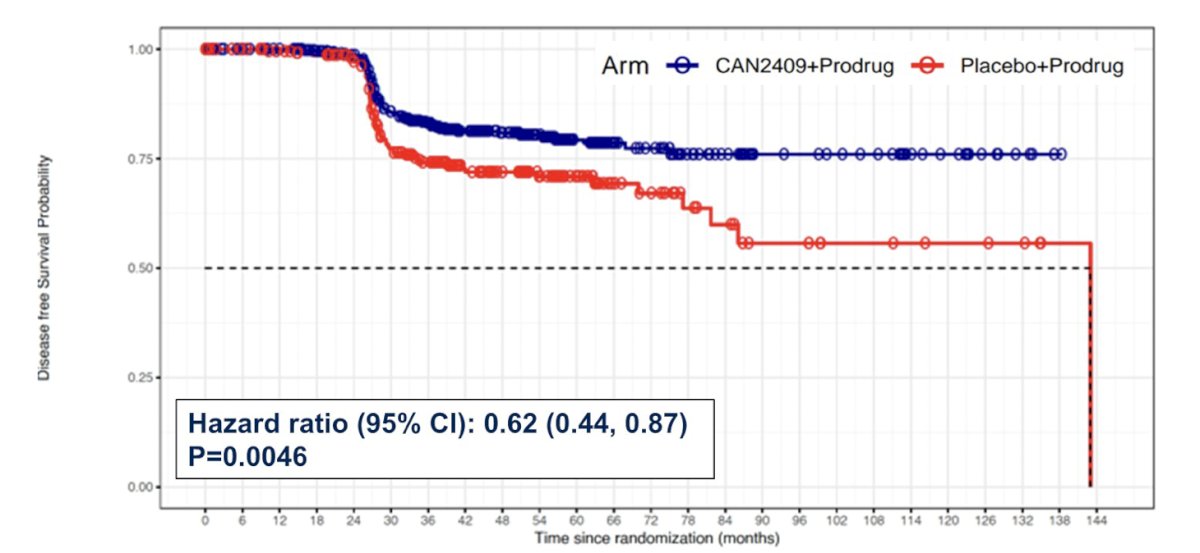
With regards to secondary endpoints, there was an increased percentage of patients achieving PSA nadir (67.1% versus 58.6%, p = 0.0164), and overall survival was similar by treatment arm in this time frame (median follow-up was 50.3 months). There were only 2 deaths due to prostate cancer (one CAN-2409 and one placebo), with 50 patient deaths due to other causes (unrelated to treatment).
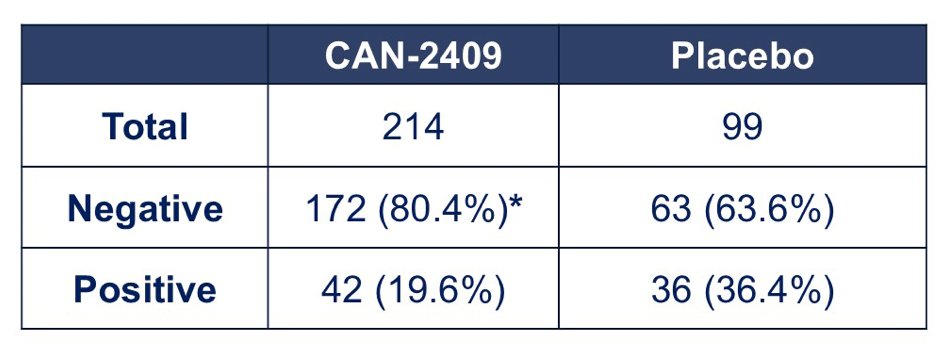
Additionally, CAN-2409 significantly improved pathological complete responses in the 2-year biopsies in the CAN-2409 arm versus placebo (80.4% versus 63.6%, p = 0.0015):
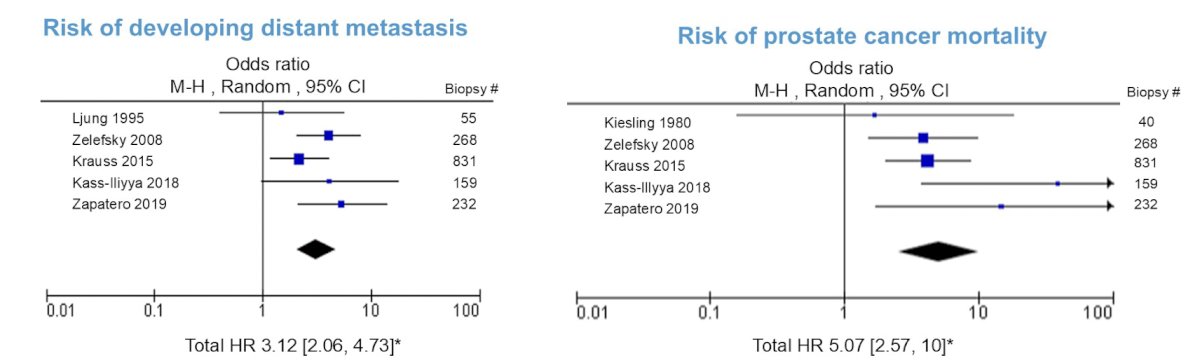
Finally, positive biopsies 2+ years after radiotherapy were predictive of metastases and cancer-related mortality after long-term follow-up. Patients with a positive biopsy had:
- 10-fold higher odds of developing biochemical failure (p < 0.00001)
- 3-fold higher odds of developing distant metastasis (p < 0.00001)
- 5-fold higher odds of dying from their prostate cancer (p < 0.00001)
Dr. DeWeese concluded his presentation discussing a phase 3, randomized, placebo-controlled clinical trial of CAN-2409 + Prodrug in combination with standard of care external beam radiation for newly diagnosed localized prostate cancer with the following take home points:
- Compared with standard of care alone, the addition of CAN-2409:
- Significantly reduced the risk of disease recurrence or death by 30% (HR 0.70, p = 0.0155)
- Significantly reduced the risk of prostate cancer recurrence or prostate cancer-related death by 38% (HR 0.62, p = 0.0046)
- Significantly increased the proportion of patients achieving a PSA nadir <0.2 ng/mL (67.1% versus 58.6%, p = 0.0164)
- Significantly improved the rate of pathological complete response in 2-year biopsies (80.4% versus 63.6%, p = 0.0015)
- CAN-2409 was generally well tolerated
- CAN-2409 immunotherapy could represent the first new therapy for men with localized prostate cancer in over 20 years
Presented by: Theodore L. DeWeese, MD, Johns Hopkins University School of Medicine, Baltimore, MD
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.Related Content: ASCO 2025: Discussion: Better Treatments, Better Selection: Improving Patient Outcomes in Localized Prostate Cancer