(UroToday.com) The 2025 American Society of Clinical Oncology (ASCO) Annual Meeting held in Chicago, IL, was host to the Oral Abstract Session: Genitourinary Cancer—Prostate, Testicular, and Penile. Dr. Angela Jia discussed How Better Treatments and Better Selection Can Improve Patient Outcomes in Localized Prostate Cancer.
Dr. Jia discussed two important abstracts presented during the session:
- Abstract 5000 presented by Dr. DeWeese: A phase 3, randomized, placebo-controlled trial evaluating CAN-2409, an oncolytic viral gene therapy, in combination with a prodrug and standard-of-care external beam radiation therapy (EBRT) for newly diagnosed localized prostate cancer. Dr Jia highlighted that this represents the first completed phase 3 trial of oncolytic viral therapy in localized prostate cancer, demonstrating a 30% relative reduction in recurrence, marking a potential new direction in localized treatment intensification.
- Abstract 5001 presented by Dr. James and focused on a multimodal artificial intelligence (MMAI) model used to identify which high-risk non-metastatic prostate cancer patients benefit most from second-generation androgen receptor pathway inhibitors (ARPIs), such as abiraterone. Derived from the STAMPEDE trial platform, this digital pathology-based biomarker was shown to be prognostic in NCCN very high-risk patients and predictive of metastasis-free survival (MFS) benefit with the addition of abiraterone, highlighting its potential role in personalizing treatment strategies.
Several emerging oncolytic viral therapies are under investigation in prostate cancer, leveraging a patient-specific immune response with a non-patient-specific prodrug. Among the most advanced is CAN-2409, a non-replicating adenoviral vector that delivers the herpes simplex virus thymidine kinase (HSV-tk) gene directly into tumor cells. This approach enables targeted activation of a prodrug within the tumor microenvironment, triggering localized cell death. CAN-2409 has been evaluated across phase I, II, and now phase III trials in localized prostate cancer.

This phase 3 randomized clinical trial enrolled 745 patients with newly diagnosed, localized prostate cancer, including approximately 85% with intermediate-risk and 15% with high-risk disease. Patients were randomized in a 2:1 ratio to receive either CAN-2409 plus valacyclovir or placebo plus valacyclovir, each administered over three intratumoral injection courses. All patients also received standard-of-care external beam radiotherapy, with short-term androgen deprivation therapy (ADT) permitted. The treatment groups were stratified by NCCN risk group and planned short-term ADT use. Valacyclovir was administered over a total of 42 days.
The primary endpoint was disease-free survival (DFS), defined as local, regional, or distant failure or death within two years following treatment. A scheduled prostate biopsy was also performed at the 2-year mark to further assess treatment effect. The study schema is shown below.

At a median follow-up of 50.3 months, treatment with CAN-2409 plus valacyclovir demonstrated a 30% relative improvement in DFS compared to placebo, with a hazard ratio (HR) of 0.70 (95% CI: 0.52–0.94; P=0.0155). This benefit was primarily driven by outcomes from the protocol-specified prostate biopsy performed 24 months post-treatment. Pathologic complete response (pCR) at 2 years was observed in 80.4% of patients in the CAN-2409 arm compared to 63.6% in the placebo group.
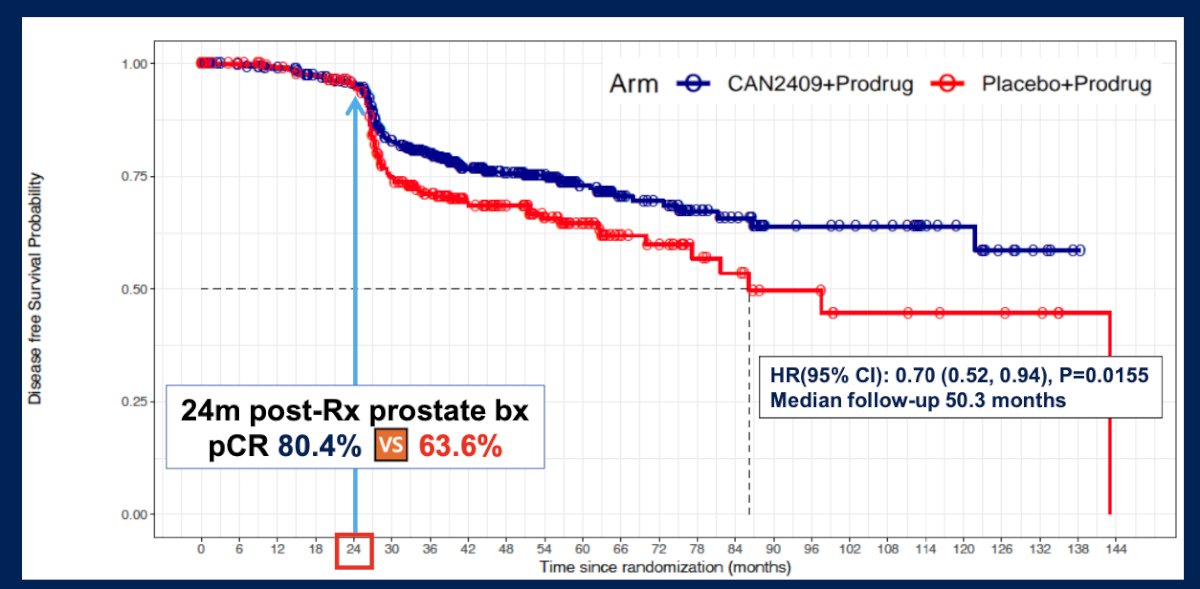
Despite these improvements in local control, overall survival and prostate cancer-specific mortality (PCSM) were not significantly different between groups, with only one PCSM event reported in each arm. Importantly, local persistence or recurrence on 2-year biopsy was significantly lower with CAN-2409 (19.6% vs 36.4%, p=0.0015), suggesting that Local failure is prognostic, but not surrogate for other OS and PCSM.
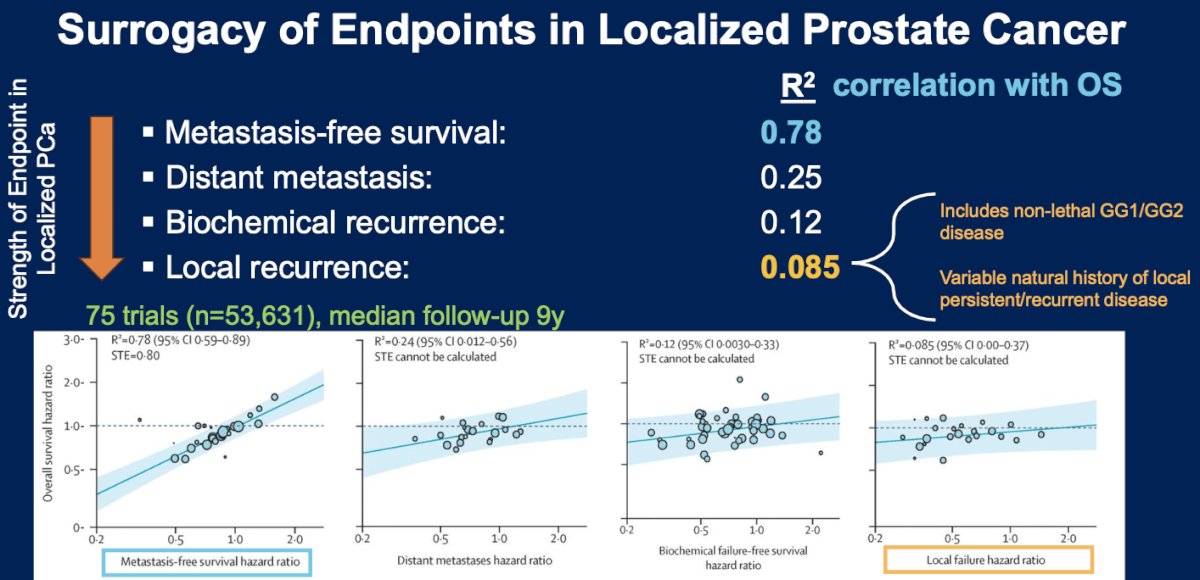
Dr. Jia highlighted findings from a meta-analysis evaluating the surrogacy of commonly used endpoints in localized prostate cancer. The analysis included 75 trials and over 53,000 patients, with a median follow-up of 9.1 years. Results demonstrated that traditional endpoints such as biochemical failure (R² = 0.38), biochemical failure-free survival (R² = 0.12), biochemical and clinical failure combined (R² = 0.28), and local failure (R² = 0.085) all correlated poorly with overall survival. In contrast, progression-free survival showed only a modest correlation with overall survival (R² = 0.46), whereas metastasis-free survival (R² = 0.78) demonstrated a strong correlation, reinforcing its value as a more reliable surrogate endpoint in clinical trials for localized prostate cancer.1
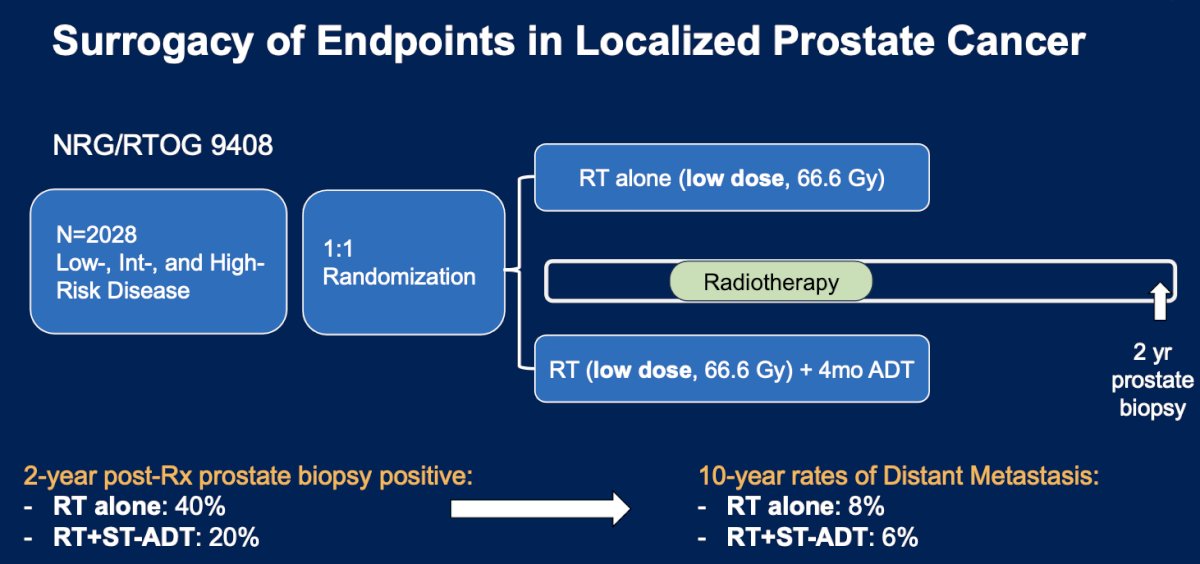
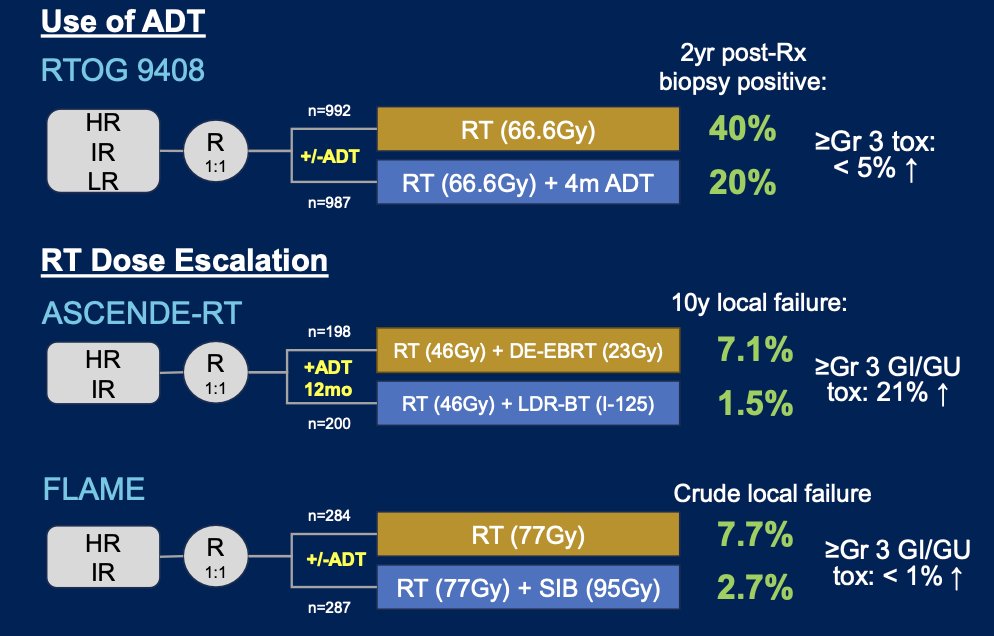
Moreover Dr. Jia highlighted findings from the NRG/RTOG 9408 trial, which enrolled 2,028 patients with low-, intermediate-, and high-risk localized prostate cancer. Patients were randomized 1:1 to receive either low-dose radiotherapy (66.6 Gy) alone or radiotherapy plus 4 months of short-term androgen deprivation therapy (ST-ADT). At the 2-year mark, post-treatment prostate biopsy revealed a significantly lower rate of cancer in the RT + ST-ADT arm (20%) compared to RT alone (40%). This reduction in local persistence was associated with modest improvements in long-term outcomes, with 10-year distant metastasis rates of 6% in the combination arm versus 8% in the RT-alone group, suggesting that early local control may translate into downstream benefits.2
The relevance of older studies like RTOG 9408 must be considered in the context of modern radiotherapy techniques, which have significantly improved local control through dose escalation and precision targeting. Data from trials like ASCENDE-RT and FLAME demonstrate that contemporary approaches, such as brachytherapy boost or focal dose intensification, dramatically reduce local failure rates—often to below 2% compared to the 20–40% positive biopsy rates observed in earlier trials using conventional dose RT. As a result, the incremental benefit of adding short-term ADT seen in historical studies may be less pronounced today, where more effective radiation delivery alone already achieves high rates of tumor ablation.3,4
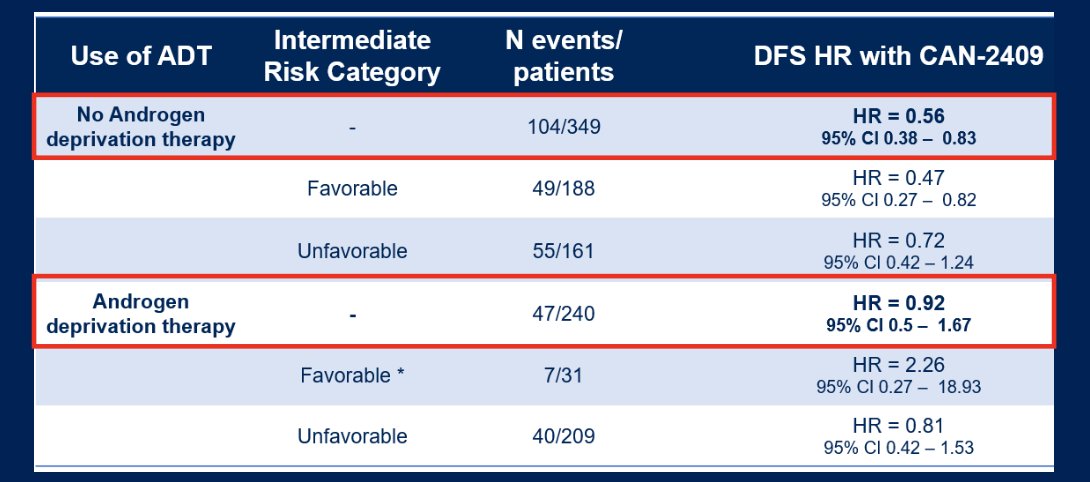
Based on the data presented, the DFS benefit of CAN-2409 remains uncertain in the context of ADT. Among patients not receiving ADT, a significant improvement in DFS was observed (HR 0.56; 95% CI: 0.38–0.83). However, in those who received short-term ADT (ST-ADT), the benefit appeared limited (HR 0.92; 95% CI: 0.50–1.67). Notably, approximately 15% of the cohort were classified as high-risk, and around 12% had Gleason ≥8 disease, yet none of these high-risk patients were planned for long-term ADT (18–36 months), which remains the standard of care in this population. This highlights the need for further evaluation of CAN-2409 in high-risk patients receiving appropriate ADT intensification.
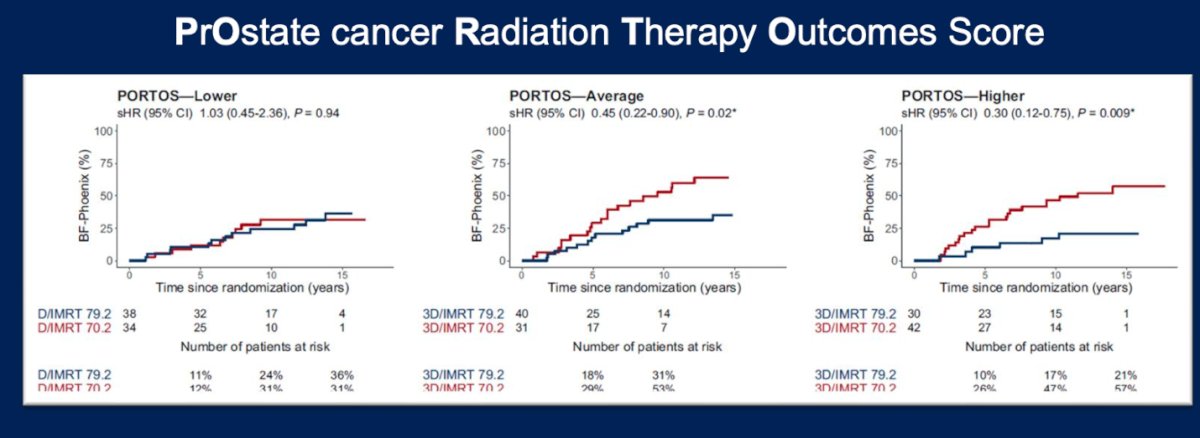
Profiling patients with high Post-Operative Radiation Therapy Outcomes Score (PORTOS) tumors may help identify those most likely to benefit from CAN-2409. The PORTOS gene expression signature has been validated in two randomized controlled trials to predict which patients can be safely treated with lower-dose radiation therapy. Notably, higher PORTOS scores are associated with tumor hypoxia and enhanced immune responses, suggesting a potential for improved therapeutic efficacy when combined with immune-stimulating agents like CAN-2409.5
Dr Jia summarized the discussion of this abstract with the following key points:
- CAN-2409 immunotherapy appears safe, with most adverse events limited to grade 1–2.
- The therapy improved disease-free survival (HR 0.70, p=0.0155), a benefit primarily driven by reduced biopsy positivity at 2 years.
- Preventing local failure remains clinically meaningful, given the added toxicity associated with salvage treatments.
- The weak correlation between local failure and overall survival underscores the importance of longer-term follow-up.
- Key questions moving forward include its integration alongside current standards such as short-term ADT in unfavorable intermediate risk disease, its potential role in PORTOS-high high-risk disease as an alternative to focal RT boost, and whether modern dose intensification strategies, such as optimized injection timing and combination with SBRT could improve outcomes.
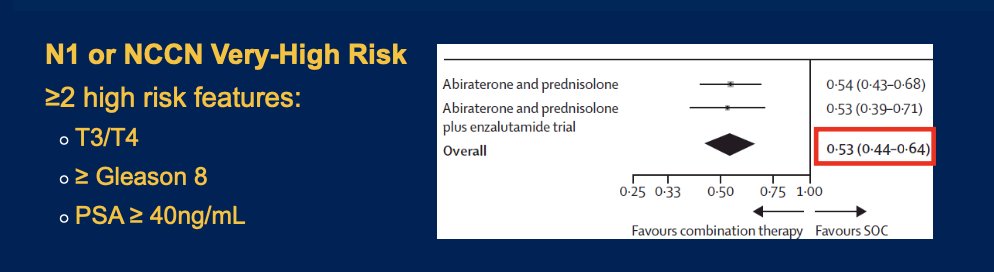
Dr Jia began by highlighting that the current standard of care for clinically high-risk M0 prostate cancer, based on the STAMPEDE platform study, involves two years of androgen deprivation therapy (ADT) combined with abiraterone and radiotherapy. The study enrolled patients with either N1 disease or NCCN-defined very high-risk features, including the presence of at least two of the following: clinical T3/T4 stage, Gleason score ≥8, or PSA ≥40 ng/mL.1 The investigators sought to determine whether a digital pathology-based AI risk score could help guide the selective use of abiraterone for treatment intensification in this patient population.
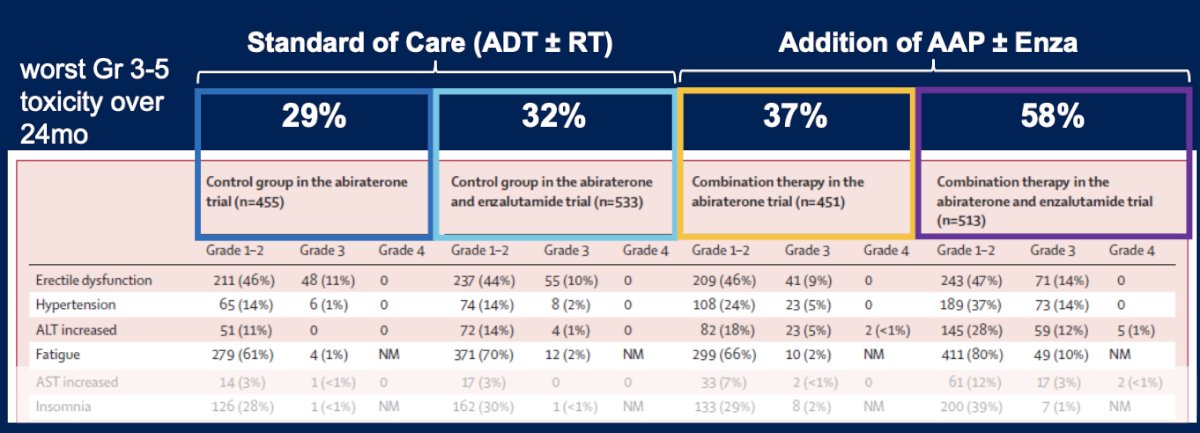
In patients with M0 hormone sensitive prostate cancer (HSPC), the addition of abiraterone or abiraterone plus enzalutamide to standard therapy has been associated with a notable increase in Grade ≥3 toxicity. In the STAMPEDE trial evaluating abiraterone, the worst Grade 3–5 toxicity over 2 years occurred in 29% of patients in the control group versus 37% in the abiraterone group, suggesting manageable toxicity. Moreover, in the trial evaluating the combination of abiraterone and enzalutamide, the toxicity was more pronounced, with Grade ≥3 events reported in 58% of patients in the combination group compared to 32% in the control arm, indicating a ~25% absolute increase in severe toxicity with intensified therapy.1
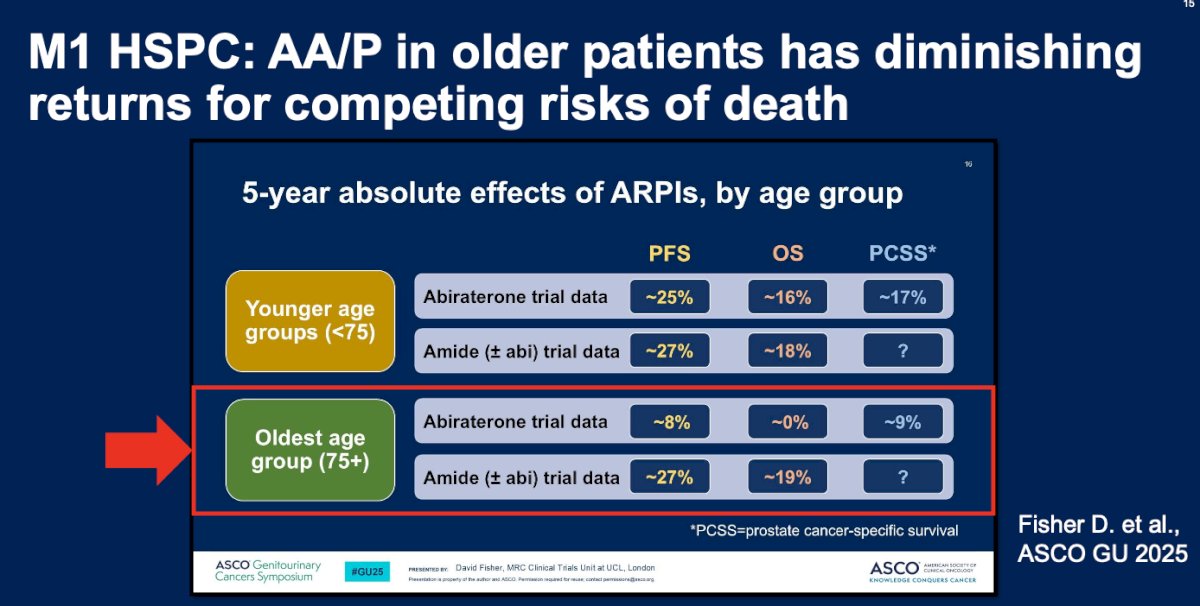
In patients with M1 HSPC, the benefit of abiraterone appears to diminish with increasing age, likely due to competing risks of death. As presented by Dr. Fisher at ASCO GU 2025, older patients (>75 years) demonstrated little to no absolute 5-year overall survival (OS) benefit from abiraterone (0%), in contrast to ~19% absolute OS benefit observed with androgen receptor pathway inhibitors (“amides”).
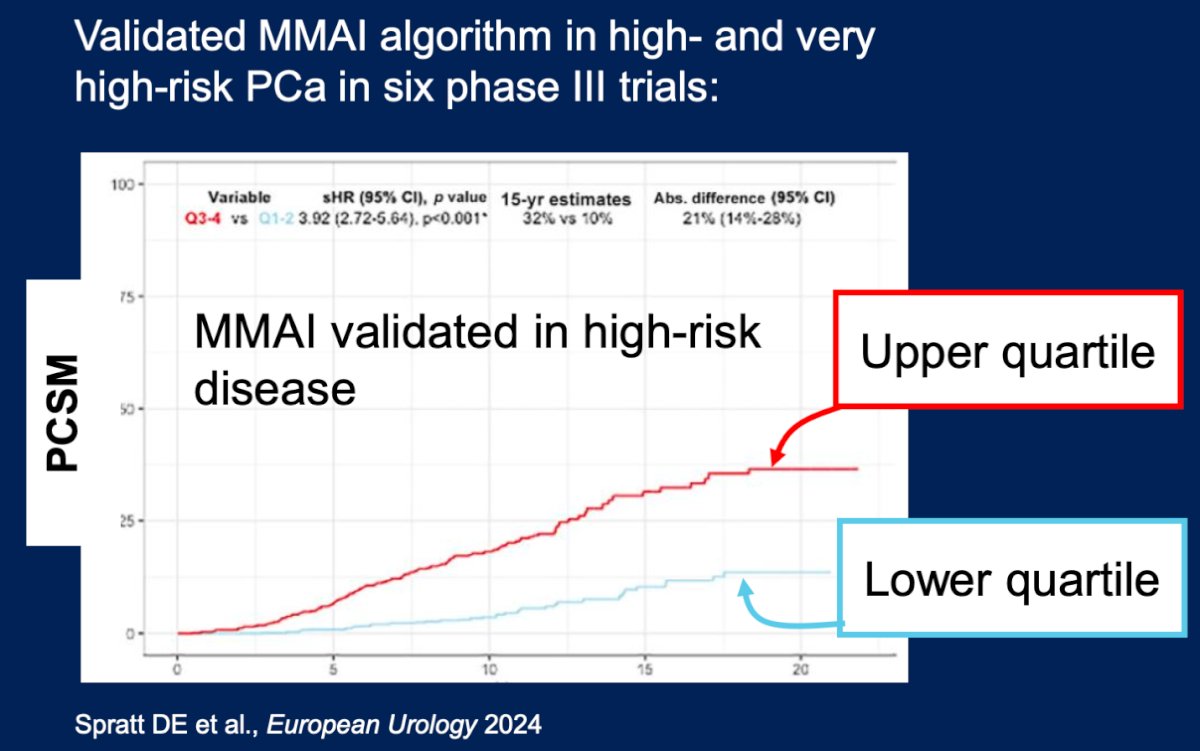
The MMAI algorithm has been validated as a prognostic biomarker in localized prostate cancer across the full risk spectrum. Initially trained and validated using five phase III trials that included patients with low-, intermediate-, and high-risk disease, the algorithm demonstrated robust prognostic capability. Further validation in six additional phase III trials confirmed its prognostic utility specifically in high- and very high-risk prostate cancer, with significant ability to predict prostate cancer–specific mortality (PCSM).7
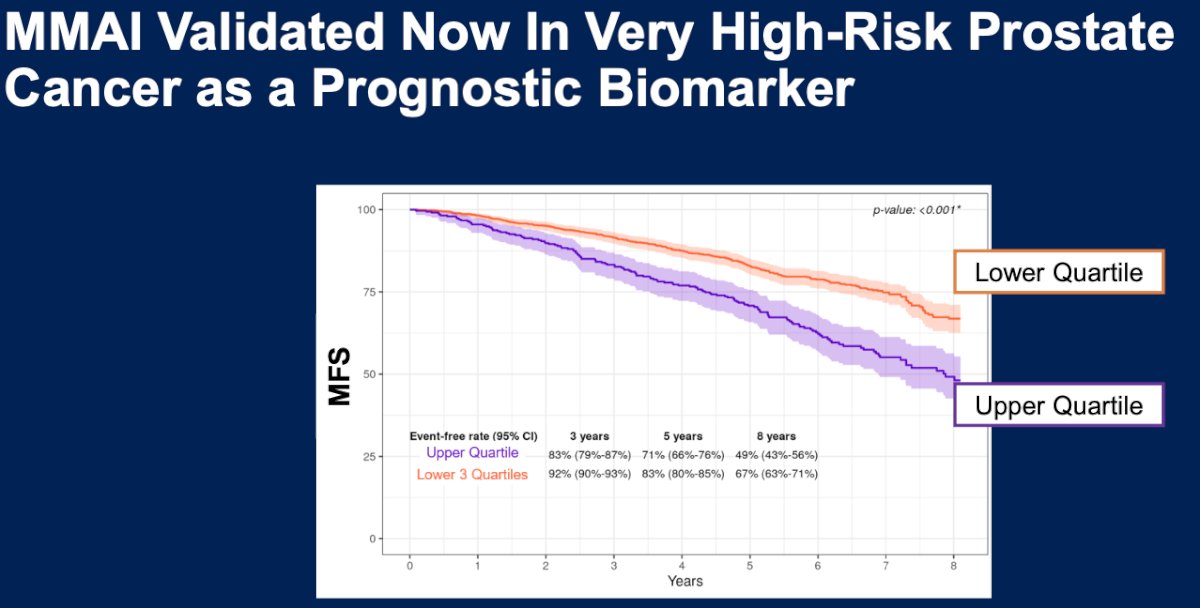
With the data presented by Dr. James, MMAI has now been validated as a prognostic biomarker in very high-risk prostate cancer. Patients in the upper quartile of MMAI-defined risk had significantly worse outcomes, with 8-year MFS of 49% compared to 67% in the lower three quartiles, as illustrated in the curve below.
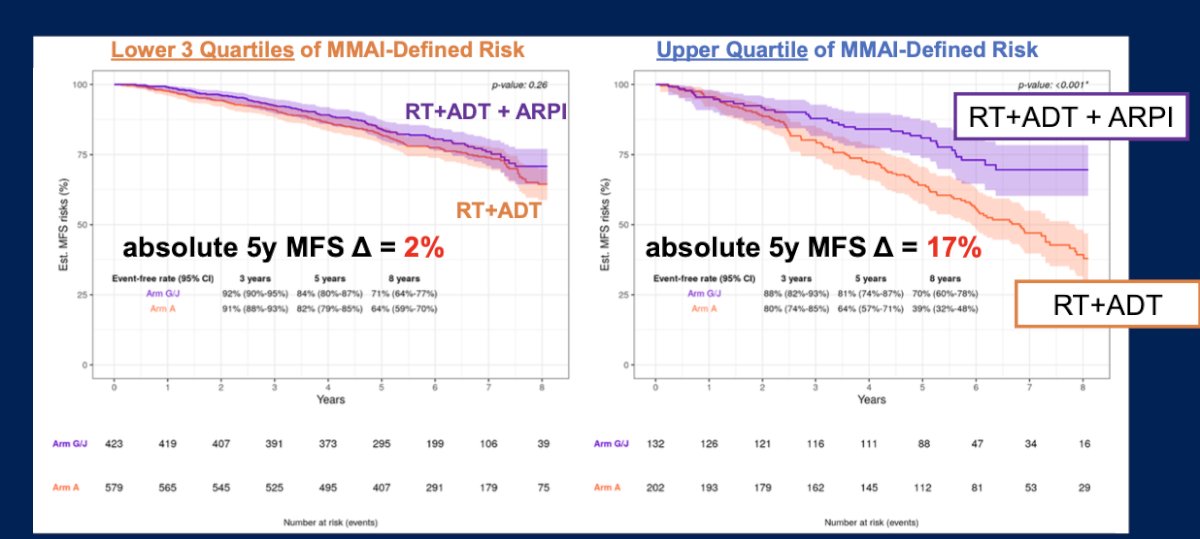
Among these patients, those with MMAI scores in the upper quartile of risk were significantly more likely to benefit from the addition of abiraterone, demonstrating a hazard ratio for metastasis-free survival (MFS) of 0.48 (95% CI: 0.33–0.71; p < 0.001). Notably, the absolute 5-year MFS difference between the RT + ADT + ARPI group and the RT + ADT group was 17% in the upper quartile, compared to only 2% in the lower three quartiles of MMAI-defined risk.
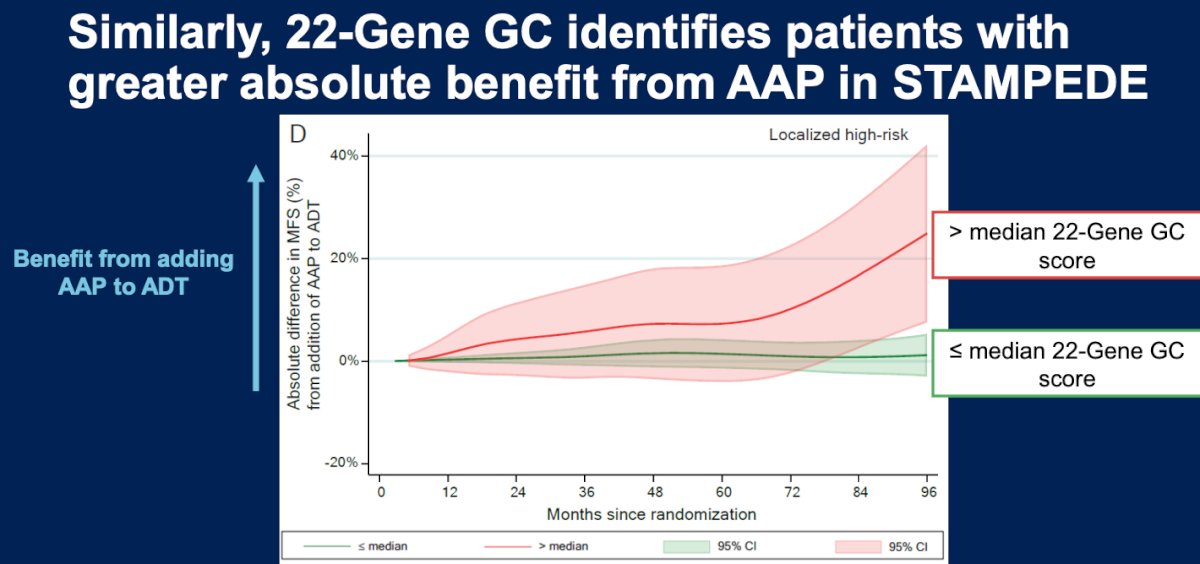
Similarly, the 22-gene genomic classifier (GC) identifies patients with greater absolute benefit from abiraterone in the STAMPEDE trial. Patients with GC scores above the median experienced a more pronounced improvement in metastasis-free survival (MFS) with the addition of abiraterone to ADT, supporting its role in guiding treatment intensification decisions.8
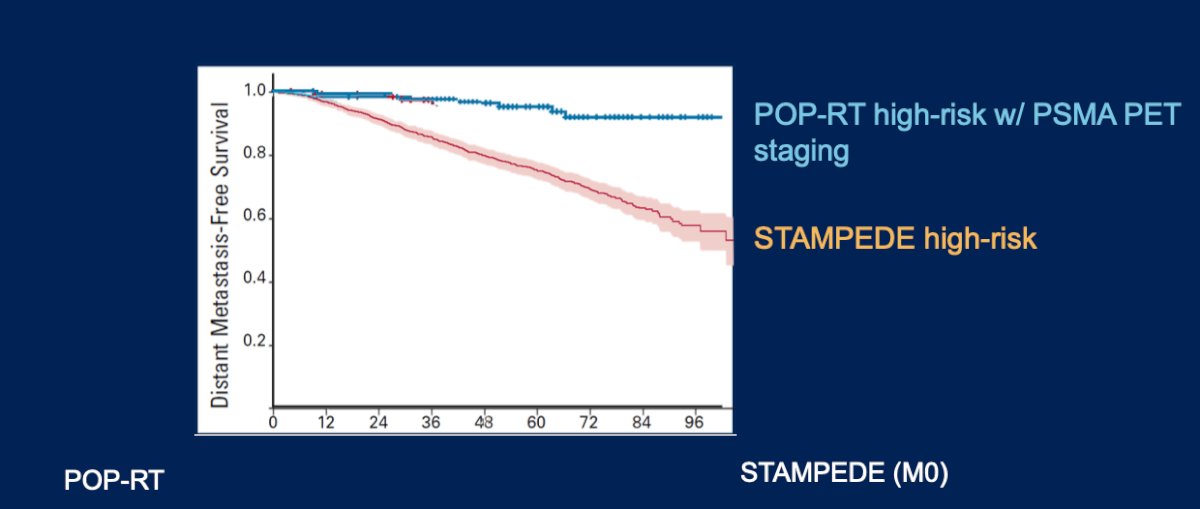
However, Dr. Jia emphasized that the high-risk patients enrolled in the STAMPEDE study may not reflect today’s contemporary high-risk prostate cancer population. Notably, none of the patients in STAMPEDE were staged using PSMA PET/CT, which is now considered standard in many settings. In contrast, more recent trials such as POP-RT have incorporated PSMA PET/CT for staging in up to 80% of patients, highlighting a shift toward more accurate disease characterization and potentially different risk stratification.

The distant metastasis-free survival (DMFS) observed in the STAMPEDE high-risk cohort is considerably lower compared to that reported in the POP-RT trial, where patients were staged with PSMA PET. This disparity underscores the limitations of conventional imaging in accurately identifying disease burden and highlights the critical need for improved staging approaches.
Dr. Jia concluded her discussion of this abstract presentation with the following take-home messages:
- STAMPEDE’s very high-risk patients benefit from the addition of abiraterone, with an associated ~25% absolute increase in grade ≥3 toxicity.
- Only the upper quartile of MMAI risk scores derived clinically meaningful improvements in metastasis-free survival from the addition of abiraterone.
- The cut-point for MMAI score was derived retrospectively.
- Applicability of these findings to contemporary high-risk populations remains unclear due to differences in staging and disease characterization.
- Future prospective trials are warranted to further explore the predictive utility of MMAI in guiding treatment intensification.
Presented by: Angela Y Jia, MD, PhD, Radiation Oncologist at University Hospitals Seidman Cancer Center, Case Western Reserve University, Cleveland, OH.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Reference:
- Gharzai LA, Jiang R, Wallington D, Jones G, Birer S, Jairath N, Jaworski EM, McFarlane MR, Mahal BA, Nguyen PL, Sandler H, Morgan TM, Reichert ZR, Alumkal JJ, Mehra R, Kishan AU, Fizazi K, Halabi S, Schaeffer EM, Feng FY, Elliott D, Dess RT, Jackson WC, Schipper MJ, Spratt DE. Intermediate clinical endpoints for surrogacy in localised prostate cancer: an aggregate meta-analysis. Lancet Oncol. 2021 Mar;22(3):402-410. doi: 10.1016/S1470-2045(20)30730-0. PMID: 33662287; PMCID: PMC10949134.
- Jones CU, Hunt D, McGowan DG, Amin MB, Chetner MP, Bruner DW, Leibenhaut MH, Husain SM, Rotman M, Souhami L, Sandler HM, Shipley WU. Radiotherapy and short-term androgen deprivation for localized prostate cancer. N Engl J Med. 2011 Jul 14;365(2):107-18. doi: 10.1056/NEJMoa1012348. PMID: 21751904.
- Morris WJ, Tyldesley S, Rodda S, Halperin R, Pai HH, McKenzie M, et al. Androgen suppression combined with elective nodal and dose escalated radiation therapy (the ASCENDE-RT trial): an analysis of survival endpoints for a randomized controlled trial. Lancet. 2015;385(9980):1547–1555. doi:10.1016/S0140-6736(14)61969-6
- Kerkmeijer LGW, Groen VH, Pos FJ, Haustermans K, Monninkhof EM, Smeenk RJ, et al. Focal boost to the intraprostatic tumor in external beam radiotherapy for patients with localized prostate cancer: results from the FLAME randomized phase III trial. J Clin Oncol. 2021;39(7):787–796. doi:10.1200/JCO.20.01964
- Zhao SG, Chang SL, Spratt DE, et al. Development and validation of a 24-gene predictor of response to postoperative radiotherapy in prostate cancer: a matched, retrospective analysis. Lancet Oncol. 2016;17(11):1612-1620. doi:10.1016/S1470-2045(16)30357-5
- Attard G, Murphy L, Clarke NW, Cross W, Jones RJ, Parker CC, Gillessen S, Cook A, Brawley C, Amos CL, Atako N, Pugh C, Buckner M, Chowdhury S, Malik Z, Russell JM, Gilson C, Rush H, Bowen J, Lydon A, Pedley I, O'Sullivan JM, Birtle A, Gale J, Srihari N, Thomas C, Tanguay J, Wagstaff J, Das P, Gray E, Alzoueb M, Parikh O, Robinson A, Syndikus I, Wylie J, Zarkar A, Thalmann G, de Bono JS, Dearnaley DP, Mason MD, Gilbert D, Langley RE, Millman R, Matheson D, Sydes MR, Brown LC, Parmar MKB, James ND; Systemic Therapy in Advancing or Metastatic Prostate cancer: Evaluation of Drug Efficacy (STAMPEDE) investigators. Abiraterone acetate and prednisolone with or without enzalutamide for high-risk non-metastatic prostate cancer: a meta-analysis of primary results from two randomised controlled phase 3 trials of the STAMPEDE platform protocol. Lancet. 2022 Jan 29;399(10323):447-460. doi: 10.1016/S0140-6736(21)02437-5. Epub 2021 Dec 23. PMID: 34953525; PMCID: PMC8811484.
- Spratt DE, Liu VYT, Jia AY, Royce TJ, Sandler HM, Pugh SL, Tran PT, Feng FY. Meta-analysis of Individual Patient-level Data for a Multimodal Artificial Intelligence Biomarker in High-risk Prostate Cancer: Results from Six NRG/RTOG Phase 3 Randomized Trials. Eur Urol. 2024 Oct;86(4):369-371. doi: 10.1016/j.eururo.2024.06.019. Epub 2024 Jul 17. PMID: 39025748; PMCID: PMC11480946.
- Parry MA, Grist E, Mendes L, Dutey-Magni P, Sachdeva A, Brawley C, Murphy L, Proudfoot J, Lall S, Liu Y, Friedrich S, Ismail M, Hoyle A, Ali A, Haran A, Wingate A, Zakka L, Wetterskog D, Amos CL, Atako NB, Wang V, Rush HL, Jones RJ, Leung H, Cross WR, Gillessen S, Parker CC, Chowdhury S; STAMPEDE collaborators; Lotan T, Marafioti T, Urbanucci A, Schaeffer EM, Spratt DE, Waugh D, Powles T, Berney DM, Sydes MR, Parmar MKB, Hamid AA, Feng FY, Sweeney CJ, Davicioni E, Clarke NW, James ND, Brown LC, Attard G. Clinical testing of transcriptome-wide expression profiles in high-risk localized and metastatic prostate cancer starting androgen deprivation therapy: an ancillary study of the STAMPEDE abiraterone Phase 3 trial. Res Sq [Preprint]. 2023 Feb 8:rs.3.rs-2488586. doi: 10.21203/rs.3.rs-2488586/v1. PMID: 36798177; PMCID: PMC9934744.
- Murthy V, Maitre P, Kannan S, Panigrahi G, Krishnatry R, Bakshi G, Prakash G, Pal M, Menon S, Phurailatpam R, Mokal S, Chaurasiya D, Popat P, Sable N, Agarwal A, Rangarajan V, Joshi A, Noronha V, Prabhash K, Mahantshetty U. Prostate-Only Versus Whole-Pelvic Radiation Therapy in High-Risk and Very High-Risk Prostate Cancer (POP-RT): Outcomes From Phase III Randomized Controlled Trial. J Clin Oncol. 2021 Apr 10;39(11):1234-1242. doi: 10.1200/JCO.20.03282. Epub 2021 Jan 26. PMID: 33497252.