Welcome to UroToday’s Center of Excellence on upper tract urothelial carcinoma (UTUC). We share peer-to-peer video conversations, expert reviews, commentaries, and conference updates to help you stay apace with best practices for managing this challenging disease. Here, I provide a brief overview of UTUC and some key updates on recent therapeutic developments.
Brief reviewUTUC, which comprises 5-10% of urothelial carcinomas, is histologically similar to bladder cancer but has distinct clinical and molecular features and management approaches. UTUC is strongly associated with Lynch syndrome and with certain toxic exposures, and has higher frequencies of FGFR3 and HRAS alterations and lower frequencies of RB1 and TP53 alterations compared with bladder cancer. Importantly, it has a worse stage-by-stage prognosis. Renal function is often poor at diagnosis and worsens after surgical management, precluding standard dosing of platinum-based perioperative therapy for many patients. Overall, this is a vulnerable patient population for whom individualized, multidisciplinary care is imperative.
Historically, radical nephroureterectomy (RNU) was the default treatment for UTUC, with nephron-sparing management (endoscopic ablation) reserved for patients with very poor baseline renal reserve, bilateral disease, or comorbidities precluding radical surgery.1 Over the past decade, we have seen a shift toward nephron-sparing approaches for the initial management of low-risk UTUC and (in some cases) high-grade disease with favorable features.2 Factors driving this trend include improved risk stratification, technological advances that improve the accuracy and quality of imaging and biopsy, and a growing evidence base in support of approaches such as lymph node dissection, neoadjuvant and adjuvant chemotherapy, and immunotherapy.1,3
Here are some recent developments of note.
New (2023) AUA/SUO GuidelinesUTUC poses challenges for clinicians due to its relative rarity and a historically scant molecular and clinical evidence base. Many patients were managed using bladder cancer treatment approaches, which often led to inferior oncologic and clinical outcomes. Moreover, there have been marked inconsistencies in management, as well as difficulty appropriately selecting patients for nephron-sparing approaches.
Recently, however, novel molecular studies and an improved understanding of the clinical features of UTUC have spurred therapeutic progress. These advances, together with the known significant impact of UTUC on renal function, have led the EAU to create dedicated guidelines on managing nonmetastatic UTUC,4 followed by joint guidelines from AUA/SUO.2 This is a major step forward for our field.
Published in 2023, the AUA/SUO guidelines include 38 recommendations spanning the full spectrum of UTUC care, from initial diagnosis and evaluation to posttreatment surveillance and survivorship.2 Key focus areas include risk assessment, nephron-sparing management, surgical options (including lymph node dissection), neoadjuvant and adjuvant chemotherapy and immunotherapy, and detailed specifications for post-treatment monitoring, which are stratified by surgical approach and pathology results.
The guidelines emphasize the need to avoid overtreatment, recommending endoscopic tumor ablation as the preferred initial management approach for patients with low-risk favorable UTUC, with additional consideration of this approach for patients with low-risk unfavorable UTUC and a minority of patients with high-risk favorable disease who have low-volume tumors or cannot undergo RNU. The table below is from the AUA/SUO guidelines and specifies how to stratify patients based on pathology and clinical features.
Table 1. Presurgical clinical risk categories from the 2023 AUA/SUO Guidelines on the Diagnosis and Management of Non-Metastatic UTUC2 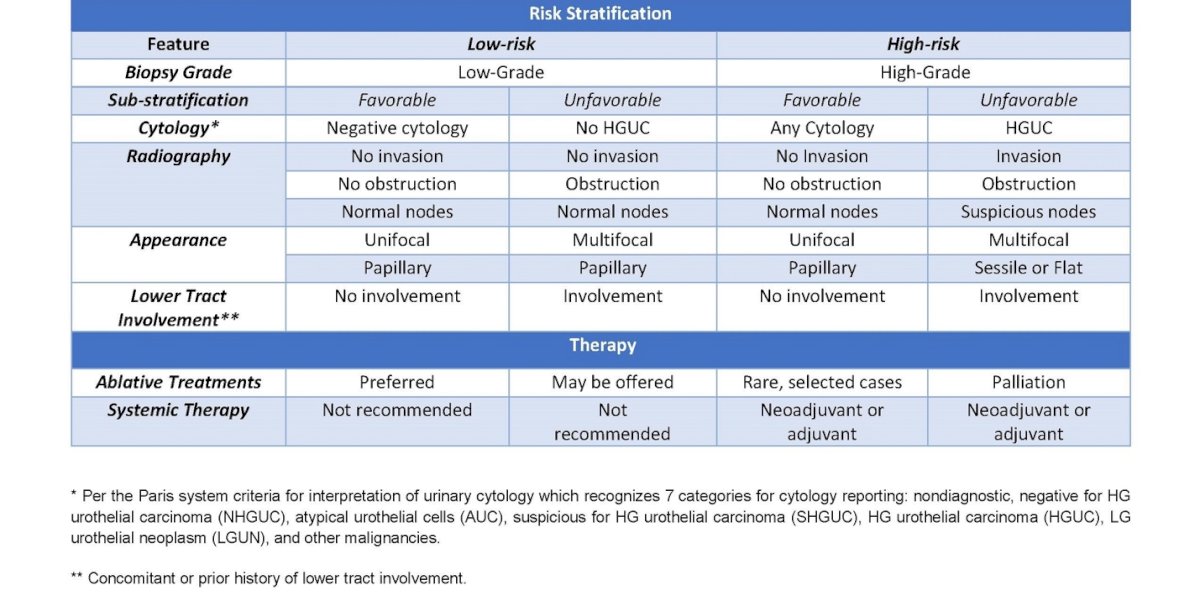
Another key takeaway is to consider neoadjuvant chemotherapy for patients with very high risk UTUC because many will be ineligible for adjuvant chemotherapy after undergoing RNU (see below for discussion of supporting data). In addition, all patients with UTUC should be screened for hereditary Lynch syndrome to guide the consideration of immunotherapy (if tumors show microsatellite instability) and to allow for cascade genetic testing and genetic counseling if desired.
These guidelines represent a step-forward in risk-stratified, adapted management that attempts to account for many factors that other guidelines have not integrated. Academic and residency programs already have begun educating residents with curricula that adapt the guidelines.
UGN-101 (mitomycin gel) shows durability in patients with low-grade UTUCFor patients with low-grade UTUC, endoscopic ablation, typically employing holmium:YAG lasers, has shown noninferior oncologic outcomes compared with RNU and avoids the morbidities of radical surgery.4 Unfortunately, UTUC tends to recur after treatment, so patients require long-term endoscopic surveillance, which increases their cumulative risk of treatment-emergent complications such as stricture, infection, and chronic stent-related symptoms. Paradoxically, some patients who initially receive nephron-sparing ablation for UTUC later develop surveillance-emergent complications and must undergo RNU.
Aqueous topical adjuvant chemotherapy has been explored to prolong disease-free survival and decrease the need for such intensive surveillance, but its efficacy is limited by rapid drug dilution and evacuation due to physiologic urine flow. To overcome this limitation, Jelmyto (UGN-101) employs a reverse thermal technology in which mitomycin is instilled into the upper urinary tract in a chilled liquid form that turns into a gel as it warms to body temperature. This enables the drug to reach hard-to-access areas of the complex upper tract and to remain in place for approximately 4-6 hours before gradually liquefying and being eliminated.
Jelmyto was approved by the FDA in April 2020 for the primary chemoablation of low-grade UTUC based on results from the phase 3, single-arm, open-label OLYMPUS trial of 71 patients with low-grade UTUC from the United States and Israel.5 In all, 41 (58%) had a complete response after six weekly retrograde Jelmyto instillations. Among these complete responders, 56% remained in complete response at 12-month follow-up, for an estimated response durability of 82% based on Kaplan-Meier analysis.
At AUA 2025, we heard a promising update from OLYMPUS: Of 20 surviving study participants who opted for long-term follow-up, 75% remained recurrence-free after a median follow-up time of 53.3 months, and the median durability of response was not estimable due to a low event rate. These data confirm a role for Jelmyto as a minimally invasive, kidney-sparing option for clinically suitable patients with low-grade UTUC.
Patients and caregivers should be advised that Jelmyto can cause ureteral stenosis that requires short or long-term stenting, and that the risk of this adverse event appears to rise as the number of instillations increases. The overall rate of stenosis in OLYMPUS was 44%.5 Thus, patients and caregivers should be cautioned to seek immediate medical attention if fever or flank pain occurs. They also should be educated regarding urinary and systemic symptoms of infection and advised of the need for regular monitoring for bone marrow suppression, although this is a rare side effect.
The ongoing real-world JELMYTO uTRACT registry will provide deeper insights into response rates, durability, and safety of Jelmyto. As of May 2025, this registry had enrolled 274 patients across 22 U.S. sites, with a target enrollment of 400.6 The data from this study will add a substantial body of evidence, given that OLYMPUS was relatively small and had fairly uniform demographics (68% of patients were male, and 87% were White). Although most patients with UTUC are White, the incidence of this disease has recently risen in other racial and ethnic groups,7 and these populations are understudied.
Adjuvant chemotherapy improves survival in high-risk, platinum-eligible patientsIn 2020, investigators reported a significant disease-free survival benefit from adjuvant platinum (cisplatin or carboplatinum)-based chemotherapy after RNU in patients with locally advanced UTUC (either pT2-T4 pN0-N3 M0 or pTany N1-3 M0). This study, called POUT, was an open-label, randomized, two-arm, phase 3 trial of 261 patients from 57 sites in the United Kingdom.8 After a median follow-up of 30.3 months, adjuvant gemcitabine-platinum chemotherapy was associated with an estimated 55% reduction in the risk of disease recurrence or death when compared with postsurgical surveillance alone (hazard ratio, 0.45, 95% CI, 0·30-0·68; P=0.0001). Metastasis-free survival, a secondary endpoint, also favored adjuvant-based chemotherapy, while overall survival data were immature at the time of data cutoff.
The results of POUT were compelling enough for the EAU, AUA, and NCCN to update their management recommendations to include adjuvant platinum-based chemotherapy as a standard of care for patients with high-risk, non-metastatic UTUC who have adverse pathologic features (pT2-T4 or node-positive disease), have not received neoadjuvant chemotherapy, and have adequate renal function. POUT participants had a glomerular filtration rate (GFR) of at least 30 mL/min. Current NCCN and AUA guidelines specify a GFR threshold of >60 mL/min,2,9 while EAU guidelines establish the cutoff as >45 mL/min.4
At ASCO GU 2024, investigators reported final/long-term POUT results. Five-year DFS was 62% with adjuvant platinum-based chemotherapy compared with 45% with surveillance alone, for a 45% reduction in risk of recurrence or death (HR, 0.55) favoring adjuvant treatment. Overall survival, a secondary endpoint, was 66% for adjuvant chemotherapy and 57% for surveillance alone, for an 11-month longer restricted mean survival time (HR 0.68) with adjuvant chemotherapy. Survival benefits were consistent across disease stages and held true regardless of whether patients received cisplatin or carboplatin. Adverse events were in line with what we would expect from platinum-based regimens, while quality-of-life assessments showed no major differences between study arms.
Taken together, these data support a shift toward adjuvant platinum-based chemotherapy after RNU as a standard of care for carefully selected patients with locally advanced or node-positive UTUC. Note that the guidelines correctly underscore the need for careful assessment of renal function and individualized management decisions.
A split-dose neoadjuvant cisplatin regimen shows efficacy in high-risk patientsUnfortunately, many patients with urothelial carcinoma cannot receive standard platinum-based chemotherapy due to impaired renal or cardiac function, neuropathy, or generally poor performance status. For patients with UTUC, nephrotoxicity is of particular concern, given that the prevalence of stage 3 or worse chronic kidney disease is about 40% at UTUC diagnosis and 85% after RNU.10,11 A split-dose cisplatin regimen (which divides the dose over two days) has demonstrated improved safety and maintenance of efficacy in bladder cancer but has not been evaluated in UTUC.
To fill this gap, a recent multicenter, single-arm, phase 2 trial prospectively evaluated a planned four cycles of neoadjuvant gemcitabine and split-dose cisplatin (GC) in patients with high-risk localized UTUC. In all, 57 received the neoadjuvant regimen prior to RNU and lymph node dissection.12 A total of 63% met the primary endpoint of pathologic response (<ypT2N0), and 19% had a complete pathologic response (ypT0N0), which met prespecified criteria for clinical promise. Pathologic responders experienced better long-term oncologic outcomes than non-responders, including two and five-year progression-free survival and overall survival times that exceeded values observed in historical series of patients with high-risk UTUC treated with surgery alone.13-17
Perioperative data such as overall complication rates, length of hospital stay, blood loss, and surgical duration also resembled outcomes observed in historical studies of UTUC patients who did not receive neoadjuvant therapy prior to RNU. Most patients were able to receive at least three cycles of chemotherapy and to proceed to surgery in a timely manner, and none needed dialysis after neoadjuvant treatment. Together, these data suggest that a split-dose approach maintains the efficacy of cisplatin—with observed benefits resembling those seen in bladder cancer—and that splitting the dose may expand patients’ eligibility for neoadjuvant chemotherapy. Given that we have no phase 3 trials of neoadjuvant therapy for high-risk UTUC, this study provides valuable evidence in support of this regimen.
Looking ahead: photodynamic therapyPhotodynamic therapy (PDT) is not (yet) a standard therapy for UTUC, but recent data show significant promise for patients with low-grade disease. In particular, padeliporfin vascular-targeted photodynamic therapy (VTP) combines intravenous padeliporfin (a chlorophyll-derived photosensitizer) with non-thermal laser light therapy delivered by ureteroscopy. After padeliporfin injection, the laser is activated for 10 minutes, triggering production of high levels of radical oxygen species, which selectively destroy the tumor vasculature and induce rapid tumor cell death.18
The largest study of VTP to date is the ongoing single-arm, phase 3 ENLIGHTED trial, which is enrolling patients with new or recurrent low-grade, non-invasive UTUC. who receive a planned three padeliporfin VTP treatments spaced four weeks apart. At ASCO 2025, we heard the most recent interim results, which included data from 37 patients.19 Strikingly, nearly 87% responded to padeliporfin VTP, and 73% had a complete response incorporating endoscopic, cytologic, and histologic criteria. Safety data also were promising—most events were grade 1-2 and resolved within a few days. In all, 9% of patients had serious adverse events; those that were treatment emergent included renal colic and flank pain, which typically resolved within 2 days.
The ENLIGHTED trial aims to enroll 100 patients and is scheduled to end in 2029.20 Thus far, its data have generated substantial interest in the urology community. Note that padeliporfin VTP is an outpatient procedure and less technically challenging than other endoscopic management approaches for UTUC, requiring only basic fiber placement skills. Its minimal invasiveness and the potential to avoid repeated endoscopic resections while sparing the kidney may substantially reduce complications while improving quality of life for appropriately selected patients. Additional trials may clarify the efficacy and durability of padeliporfin VTP and other photodynamic therapies in high-grade disease.
Written by: Sam S. Chang, M.D., M.B.A. Patricia and Rodes Hart Endowed Chair of Urologic Surgery Professor Department of Urology at Vanderbilt University Medical Center
- Metcalf M, Pierorazio PM. Future strategies to enhance kidney preservation in upper urinary tract urothelial carcinoma. Transl Androl Urol. 2020 Aug;9(4):1831-1840.
- Coleman JA, Clark PE, Bixler BR, et al. Diagnosis and management of non-metastatic upper tract urothelial carcinoma: AUA/SUO guideline. J Urol. 2023;209(6):1071-1081.
- Yip W, Jaime-Casas S, Kothari A, et al. Urothelial carcinoma: Perioperative considerations from top to bottom. CA Cancer J Clin. 2025 Jun 6.
- Rouprêt M, Babjuk M, Burger M, et al. European Association of Urology Guidelines on Upper Urinary Tract Urothelial Carcinoma: 2023 Update. Eur Urol. 2023;84(1):49-64..
- Matin SF, Pierorazio PM, Kleinmann N, et al. Durability of response to primary chemoablation of low-grade upper tract urothelial carcinoma using UGN-101, a mitomycin-containing reverse thermal gel: OLYMPUS Trial Final Report. J Urol. 2022 Apr;207(4):779-788.
- Feldman MA.The uTRACT registry: A single-arm, multicenter, prospective, and retrospective registry study to evaluate the real-world use of UGN-101 in participants with upper tract urothelial carcinoma (UTUC) in the United States. J Clin Oncol. 2025;43(16). TPS4629.
- Petros FG. Epidemiology, clinical presentation, and evaluation of upper-tract urothelial carcinoma. Transl Androl Urol. 2020;9(4):1794-1798.
- Birtle AJ, Jones R, Chester J, et al. Improved Disease-Free Survival With Adjuvant Chemotherapy After Nephroureterectomy for Upper Tract Urothelial Cancer: Final Results of the POUT Trial. J Clin Oncol. 2024 1;42(13):1466-1471.
- National Comprehensive Cancer Network (NCCN). NCCN Clinical Practice Guidelines in Oncology: Bladder Cancer. Version 6.2024. Accessed June 20, 2025. https://www.nccn.org/guidelines/guidelines-detail?category=1&id=1417
- Shao IH, Lin YH, Hou CP, et al. Risk factors associated with ineligibility of adjuvant cisplatin-based chemotherapy after nephroureterectomy. Drug Des Devel Ther. 2014;8:1985–1990.
- Raman JD, Lin YK, Kaag M, et al. High rates of advanced disease, complications, and decline of renal function after radical nephroureterectomy. Urol Oncol. 2014;32:47.e9–47.e14.
- Coleman JA, Yip W, Wong NC, et al. Multicenter phase II clinical trial of gemcitabine and cisplatin as neoadjuvant chemotherapy for patients with high-grade upper tract urothelial carcinoma. J Clin Oncol. 2023;41(8):1618-1625.
- Porten S, Siefker-Radtke AO, Xiao L, et al. Neoadjuvant chemotherapy improves survival of patients with upper tract urothelial carcinoma. Cancer. 2014;120:1794-99.
- Martinez-Salamanca JI, Shariat SF, Rodriguez JC, et al. Prognostic role of ECOG performance status in patients with urothelial carcinoma of the upper urinary tract: An international study. BJU Int. 2012;109:1155–61.
- Zeuschner P, Vollmer SG, Linxweiler J, et al. Robot-assisted versus open radical nephroureterectomy for urothelial carcinoma of the upper urinary tract: A retrospective cohort study across ten years. Surg Oncol. 2021;38:101607.
- Krabbe LM, Eminaga O, Shariat SF, et al. Postoperative nomogram for relapse-free survival in patients with high grade upper tract urothelial carcinoma. J Urol. 2017;197:580–589.
- Zennami K, Sumitomo M, Takahara K, et al. Two cycles of neoadjuvant chemotherapy improves survival in patients with high-risk upper tract urothelial carcinoma. BJU Int. 2021;127:332–339.
- Yoshida T, Motoki Y, Rogers CG, et al. Photodynamic diagnosis-guided ureteroscopic laser ablation of upper urinary tract urothelial carcinoma: phase 2, open-label, single-arm trial. Ann Surg Oncol. 2025;32(1):35-38.
- Margulis V, Kaufman RP, Marcq G, et al. ENLIGHTED phase 3 study: Interim results of efficacy and safety of padeliporfin vascular targeted photodynamic therapy (VTP) in the treatment of low-grade upper tract urothelial cancer (LG UTUC). J Clin Oncol. 2025;43(17):LBA4513.
- ClinicalTrials.gov. ENdoluminal LIGHT ActivatED Treatment of Upper Tract Urothelial Cancer (ENLIGHTED) Study (UCM301). Accessed June 23, 2025. https://clinicaltrials.gov/study/NCT04620239