(UroToday.com) The 2025 SNMMI annual meeting featured a prostate cancer and molecular imaging session and a presentation by Dr. Madeleine Karpinski discussing the three-tier risk stratification of prostate cancer by PSMA-PET PROMISE (PPP2).
Previously, these investigators established two prognostic nomograms of PSMA-PET standardized by the Prostate Cancer Molecular Imaging Standardized Evaluation (PROMISE) criteria for stratification into low versus high risk in a large single-center cohort. At the 2025 SNMMI annual meeting, Dr. Karpinski and colleagues updated both PPP2 nomograms with three-tier risk stratification in a large international multi-center registry study.
Patients included in the analysis had histologically proven prostate cancer and underwent PSMA-PET at 20 hospitals in Germany, Italy, Sweden, the Netherlands, Belgium, Slovakia, Austria, the United States, and Australia between 2014 and 2021. PSMA-PET was standardized by PROMISE version 2. The investigators obtained total lesion count, total tumor volume, PSMA expression score, and overall survival follow-up. Considering site characteristics, they split the investigator sites 2:1 into development and validation cohorts. PPP predictors were assessed and created version 2 for visual and quantitative PPP2 nomograms based on Cox regression models with least absolute shrinkage and selection operator penalty for overall survival using the development cohort. The visual and quantitative PSMA PET metrics are highlighted as follows: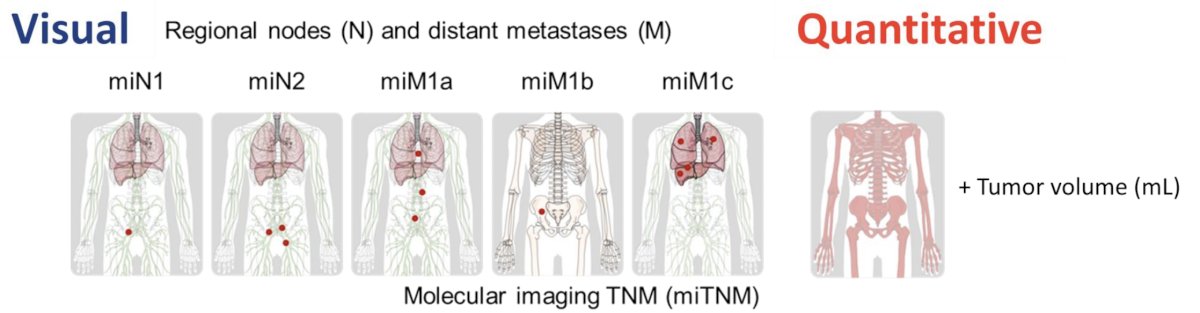
There were 6,128 male patients (4,044 development and 2,084 validation cohorts) included across all disease stages with a median follow-up of 4.8 years (IQR 3.4-6.4). Over this follow-up time, 1,915 (31.2%) deaths were reported. Predictors in the visual PPP2 nomogram were the presence of distant metastases (extrapelvic nodal metastases [M1a], bone metastases [M1b; oligometastatic, disseminated or diffuse marrow involvement], and visceral metastases [M1c]), PSMA expression score, and total lesion count:![There were 6,128 male patients (4,044 development and 2,084 validation cohorts) included across all disease stages with median follow-up of 4.8 years (IQR 3.4-6.4). Over this follow-up time, 1,915 (31.2%) deaths were reported. Predictors in the visual PPP2 nomogram were presence of distant metastases (extrapelvic nodal metastases [M1a], bone metastases [M1b; oligometastatic, disseminated or diffuse marrow involvement], and visceral metastases [M1c]), PSMA expression score, and total lesion count:](/images/com-doc-importer/221-snmmi-2025/snmmi-2025-three-tier-risk-stratification-of-prostate-cancer-by-psma-pet-promise-ppp2-results-from-an-international-multi-center-registry-study/image-1.jpg)
Predictors in the reassessed quantitative PPP2 nomogram were distant metastases (M1a, M1b, and M1c), total tumor volume, and PSMA expression score: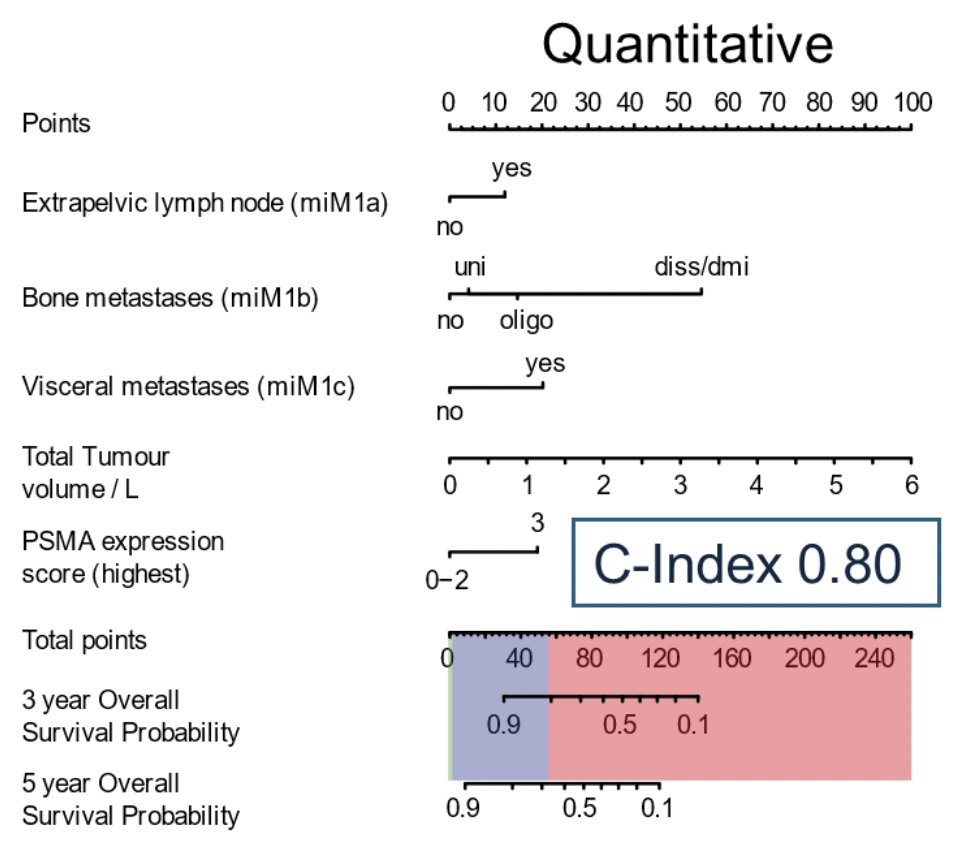
C-indices in the validation cohort were 0.80 (95% CI 0.78-0.82) for the visual and 0.80 (95% CI 0.79-0.82) for the quantitative nomogram, respectively. Accuracy of both PPP2 nomograms for three-tier stratification (high, intermediate, low risk) in the validation cohort was superior when compared to the NCCN risk score (n = 1,034, AUC 0.84 versus 0.76; p < 0.0001, respectively):
Performance of both PPP2 nomograms was independent of PROMISE version: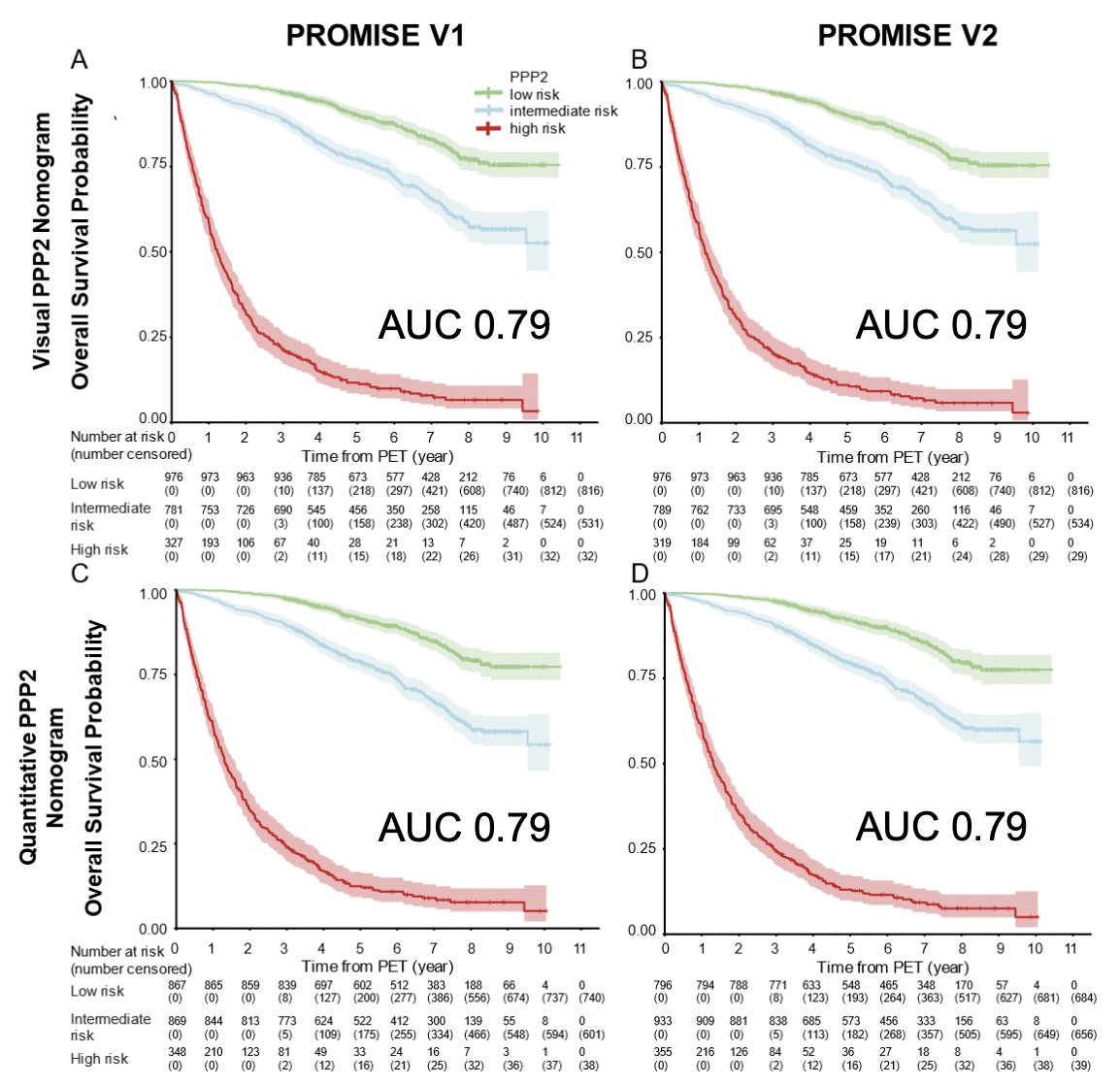
Additionally, performance of both PPP2 nomograms was independent of 68Ga versus 18F-based PSMA radiotracers: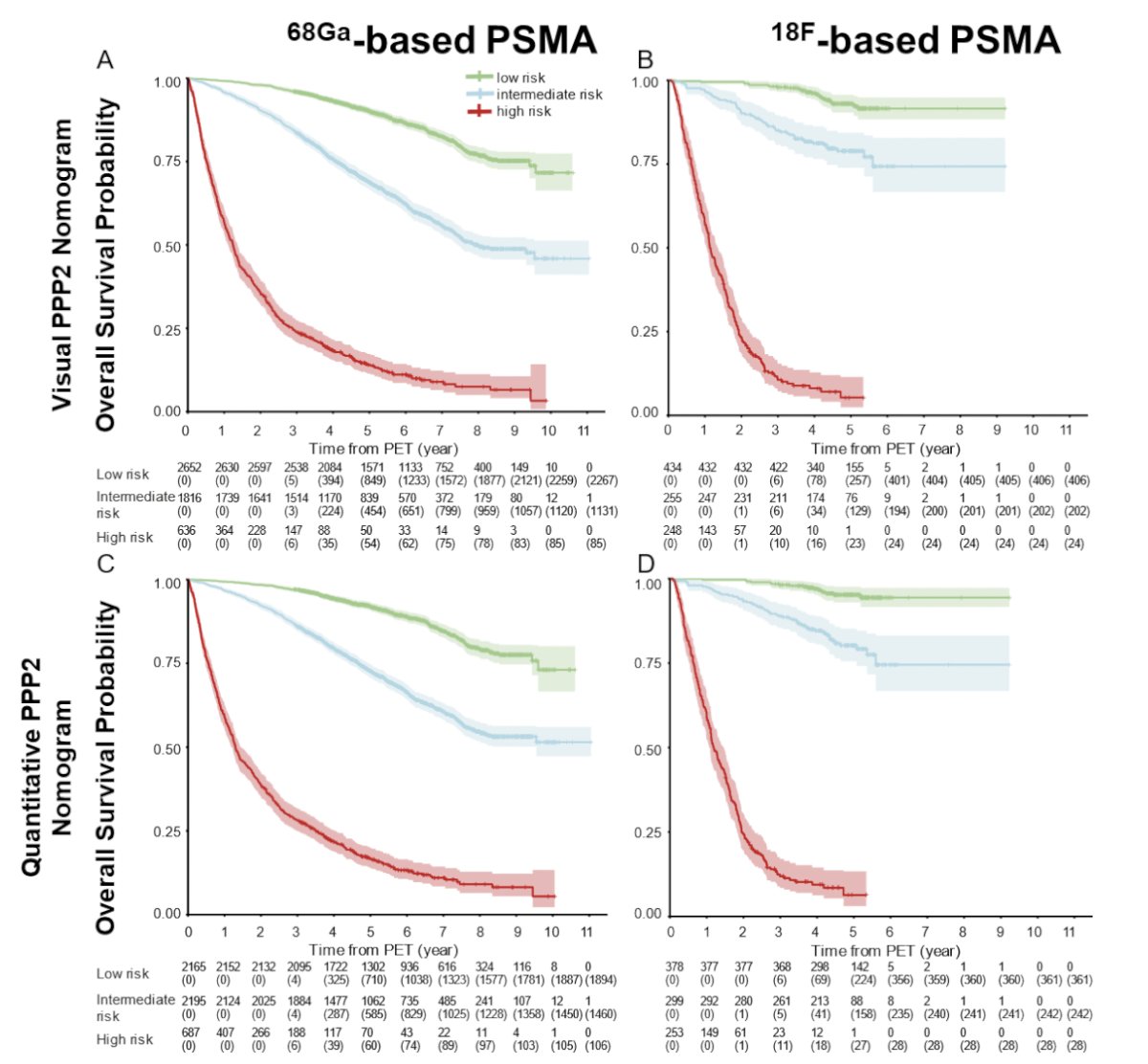
Dr. Karpinski concluded her presentation discussing the three-tier risk stratification of prostate cancer by PPP2 with the following take-home points:
- PPP2 nomograms accurately stratify prostate cancer patients, regardless of radiopharmaceutical (68Ga versus 18F) or PROMISE version (v1 versus v2)
- PPP2 nomograms yield superior accuracy compared to NCCN or EAU risk groups
- Follow-up continues in the PROMISE Registry (NCT06320223, promisepet.org)
Presented by: Madeleine Karpinski, DKTK and NCT University Hospital Essen, Essen, Germany
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the Society of Nuclear Medicine and Molecular Imaging (SNMMI) 2025 Annual Meeting, New Orleans, LA, Sat, Jun 21 – Tues, Jun 24, 2025.