(UroToday.com) The 2025 ESMO annual meeting featured a prostate cancer session and a presentation by Neal D. Shore, MD, FACS, discussing patient-reported outcomes in a randomized phase 1 study of mevrometostat + enzalutamide versus enzalutamide alone in patients with metastatic castration‑resistant prostate cancer (mCRPC).
EZH2 is overexpressed in patients with CRPC and is associated with more advanced disease and a poor prognosis. EZH2 also contributes to disease progression via transcriptional repression of tumor suppressor genes and activation of the androgen receptor, co-regulation of androgen receptor-mediated transcriptional programs, as well as cell cycle deregulation.
Mevrometostat is an oral potent selective inhibitor of EZH2. Previously, dose exploration of mevrometostat + enzalutamide showed promising antitumor activity versus enzalutamide alone in patients with mCRPC, and a manageable safety profile. At the 2025 ESMO annual meeting, Dr. Shore and colleagues reported health-related quality of life outcomes from the randomized, dose-expansion part of this phase 1 study.
Patients with progressive mCRPC who received prior abiraterone and ≤1 prior chemotherapy were randomized 1:1 to mevrometostat (1,250 mg BD on an empty stomach) + enzalutamide (160 mg QD) or enzalutamide alone:
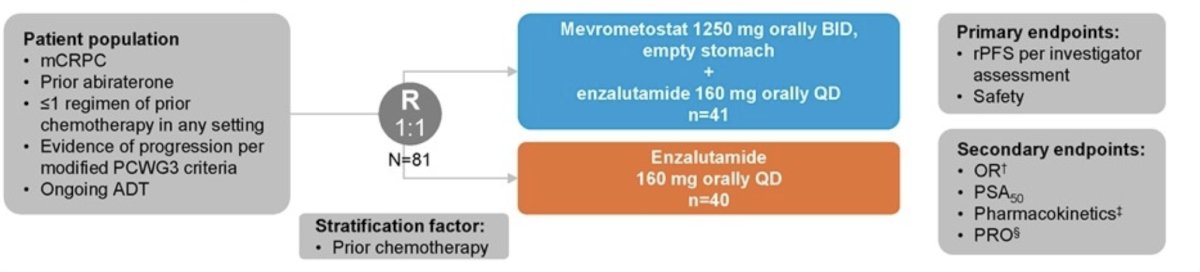
Patients completed the FACT-P questionnaire at baseline and regularly until disease progression. Prespecified analyses included treatment comparison of estimated overall mean change from baseline and time to definitive clinically meaningful deterioration (time from first dose to first greater than threshold point decrease from baseline and no subsequent less than threshold point decrease from baseline) for FACT-P total score (≥10-point change) and FACT-P subscales (prostate cancer subscale [≥3-point change], trial outcomes index [≥9-point change] and FACT-General total score [≥7-point change]). Time to definitive clinically meaningful deterioration was compared via a stratified log-rank test and Cox proportional hazard model.
As of September 2, 2024, 68/81 patients had a baseline plus ≥1 post-baseline score (mevrometostat + enzalutamide, n = 36; enzalutamide, n = 32). No significant differences were observed between arms in change from baseline in FACT-P total score, FACT-G total score, FACT-P subscales, or the four wellbeing domains, except for the physical wellbeing domain, which favored the enzalutamide alone arm:

Kaplan-Meier curves for time to definitive clinically meaningful deterioration in FACT-P total score, prostate cancer subscale score, and trial outcome index score, and FACT-G score are shown as follows:
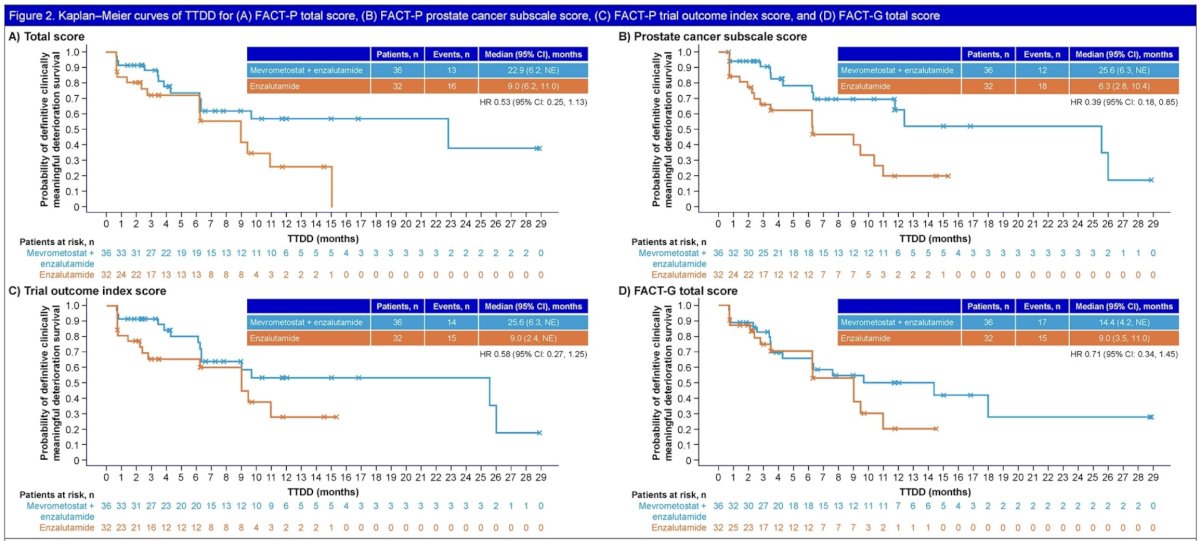
A delay in time to definitive clinically meaningful deterioration was observed in the FACT-P prostate cancer subscale and the social/family wellbeing domain for mevrometostat + enzalutamide versus enzalutamide alone. Time to definitive clinically meaningful deterioration was also similar for FACT-P total score, FACT-P trial outcomes index, and FACT-G total score for mevrometostat + enzalutamide versus enzalutamide alone. Limitations of this analysis include the small sample size, the open-label study design, and the lack of type 1 error control.
Dr. Shore concluded his presentation discussing patient-reported outcomes in a randomized phase 1 study of mevrometostat + enzalutamide versus enzalutamide alone in patients with mCRPC with the following take-home points:
- In this pre-specified analysis of patient-reported outcomes using the FACT-P questionnaire, the addition of mevrometostat to enzalutamide resulted in no clinically meaningfully differences in quality of life outcome measures compared with enzalutamide alone
- Time to definitive clinically meaningful deterioration was longer with mevrometostat + enzalutamide versus enzalutamide alone for the FACT-P prostate cancer subscale; this was also similar between treatment groups for FACT-P and FACT-G total scores, and the FACT-P trial outcome index score
- Pivotal phase 3 studies of mevrometostat with enzalutamide are ongoing to further investigate these findings:
– MEVPRO-1 (NCT06551324), in patients with mCRPC previously treated with abiraterone
– MEVPRO-2 (NCT06629779), in patients with mCRPC who are androgen receptor pathway inhibitor-naïve
– MEVPRO-3 (NCT07028853), in patients with metastatic castration-sensitive prostate cancer who are androgen receptor pathway inhibitor-naïve
Presented by: Neal D. Shore, MD, FACS, Director, CPI (Certified Principal Investigator by the Association of Clinical Research Professionals), Medical Director for the Carolina Urologic Research Center, AUC Urology Specialists, Myrtle Beach, South Carolina
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Meeting, Berlin, Germany, Fri, Oct 17 – Tues, Oct 21, 2025.