(UroToday.com) The 2025 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA was host to the Trials in Progress Poster Session A: Prostate Cancer. Neeraj Agarwal, MD, FASCO, presented the trial in progress poster 288: Mevrometostat (PF-06821497) in combination with enzalutamide in patients with metastatic castration-resistant prostate cancer previously treated with abiraterone acetate: The phase 3, randomized MEVPRO-1 study.
Resistance to androgen receptor (AR) pathway inhibitors (ARPIs), such as abiraterone and enzalutamide, in metastatic castration-resistant prostate cancer (mCRPC) may be driven by the persistence of AR signaling through various mechanisms.1-3 Enhancer of zeste homolog 2 (EZH2) has been implicated in the pathogenesis of prostate cancer and ARPI resistance. Combining ARPIs with therapies that target alternative signaling pathways, including epigenetic modifiers like EZH2, represents a promising strategy to overcome the aforementioned resistance mechanisms.5-7
Dr. Agarwal described the study design of a phase 3 trial evaluating whether the addition of mevrometostat, a potent and selective EZH2 inhibitor, to enzalutamide can overcome anti-androgen resistance and extend the duration of clinical benefit in patients with mCRPC previously treated with abiraterone. Initial results from the phase 1 dose-escalation study (NCT03460977) demonstrated promising activity for mevrometostat in combination with enzalutamide, with a manageable adverse-event profile in abiraterone-exposed patients with mCRPC.7
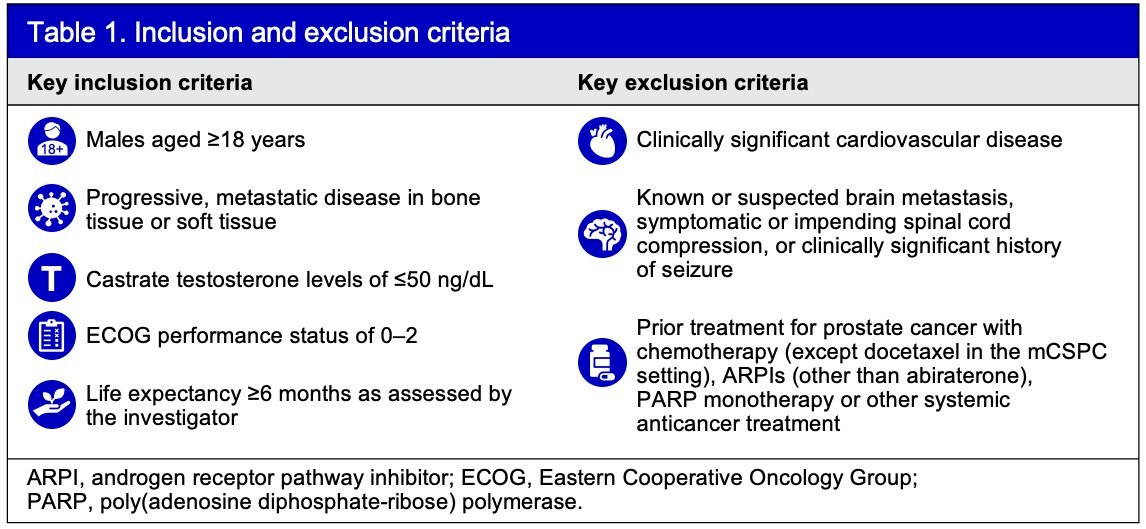
MEVPRO-1 (NCT06551324) is a global, open-label, phase 3 trial in patients with mCRPC aged ≥18 years with progression on/after ≥12 weeks abiraterone, castration testosterone levels ≤50 ng/dL, ECOG performance status 0–2, and life expectancy ≥6 months. Inclusion and exclusion criteria are summarized below:
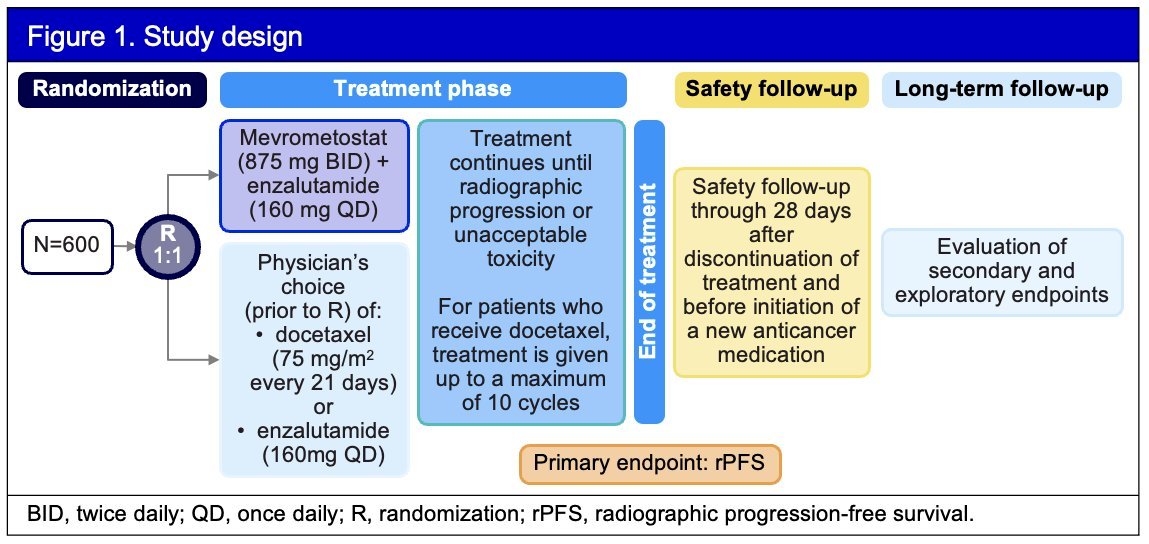
The investigators aim to randomize 600 patients in a 1:1 ratio to receive either mevrometostat (875 mg BID with food) plus enzalutamide (160 mg QD) or the physician’s choice of enzalutamide (160 mg QD) or docetaxel (75 mg/m² IV every 21 days). The study design is illustrated in the figure below.
Randomization will be stratified by:
- Previous docetaxel use in the metastatic castration-sensitive setting
- Physician’s choice of comparator (either enzalutamide or docetaxel) prior to randomization
- Presence of hepatic metastases
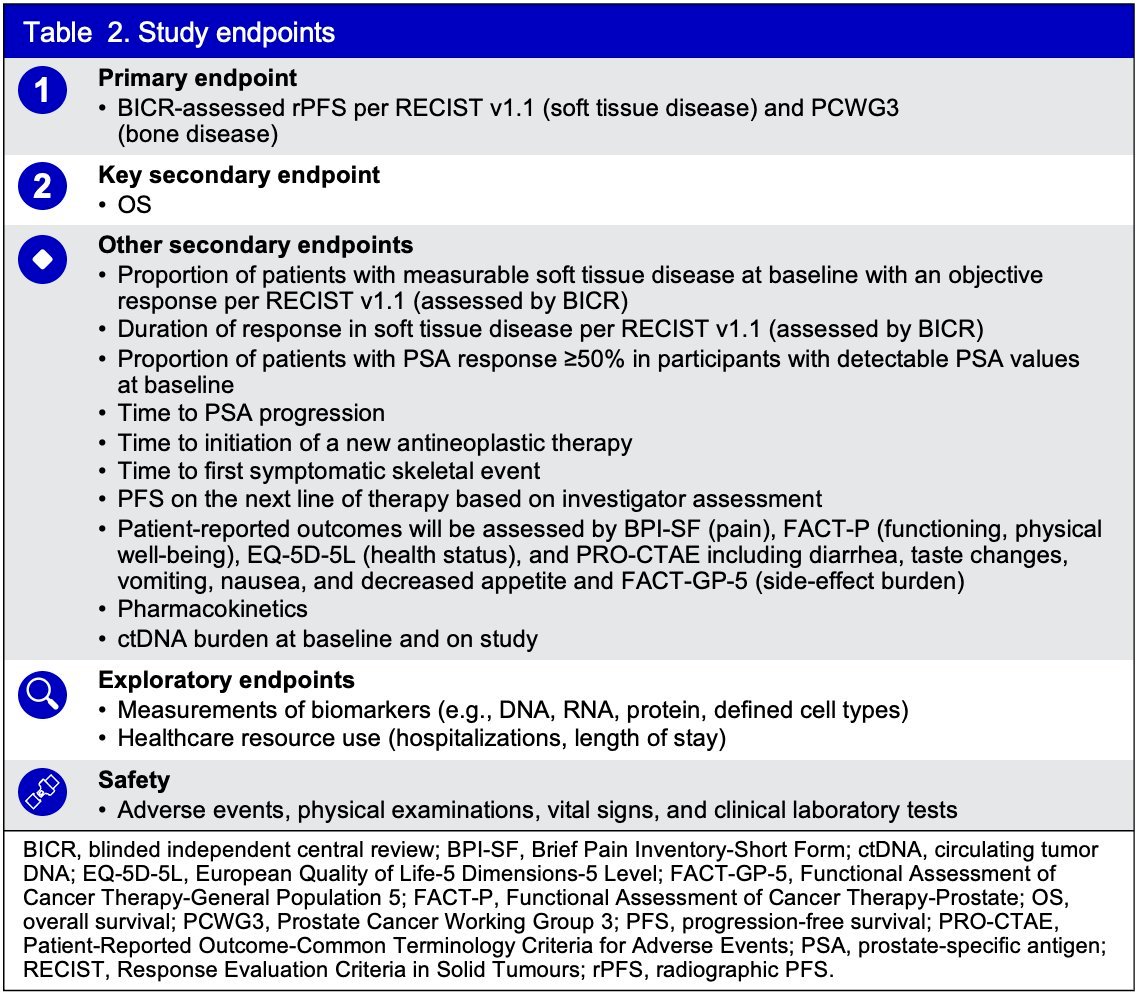
The primary efficacy endpoint is radiographic progression-free survival (rPFS), assessed by blinded central radiology review using RECIST 1.1 for soft tissue and PCWG3 criteria for bone lesions. The key secondary endpoint is overall survival (OS), while additional secondary endpoints include overall response rate, duration of response, patient-reported outcomes, pharmacokinetics, and circulating tumor DNA burden. Safety will be evaluated through adverse event monitoring, physical examinations, vital signs, and clinical laboratory tests. Study endpoints are summarized below.
The statistical analysis approach includes stratified log-rank tests for comparisons, with hazard ratios (HRs) and 95% confidence intervals (CIs) estimated using a stratified Cox proportional hazards model. Time-to-event endpoints will be summarized using Kaplan–Meier analysis.
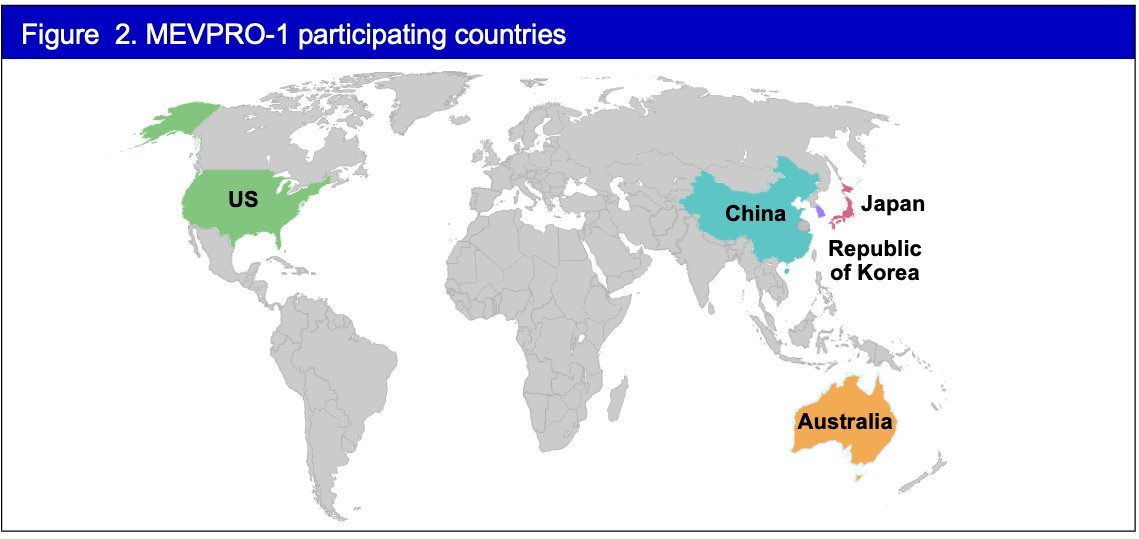
The first patient was enrolled in the MEVPRO-1 study on October 21, 2024. Currently, patient enrollment is ongoing in five countries, as outlined below. The study is expected to be completed in October 2028.
Presented by: Neeraj Agarwal, MD, FASCO, Medical Oncologist, Professor of Medicine, and a Presidential Endowed Chair of Cancer Research at the Huntsman Cancer Institute (HCI), University of Utah, United States.
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 Genitourinary (GU) American Society of Clinical Oncology (ASCO) Annual Meeting, San Francisco, CA, Thurs, Feb 13 – Sat, Feb 15, 2025.
References:- Armenia J, Wankowicz SAM, Liu D, et al. The long tail of oncogenic drivers in prostate cancer. Nat Genet. 2018;50(5):645-651.
- Quigley DA, Dang HX, Zhao SG, et al. Genomic hallmarks and structural variation in metastatic prostate cancer. Cell. 2018;174(3):758-769.e9.
- Wedge DC, Gundem G, Mitchell T, et al. Sequencing of prostate cancers identifies new cancer genes, routes of progression, and drug targets. Nat Genet. 2018;50(5):682-692.
- Beltran H, Prandi D, Mosquera JM, et al. Divergent clonal evolution of castration-resistant neuroendocrine prostate cancer. Clin Cancer Res. 2019;25(23):6916-6924.
- Ku SY, Rosario S, Wang Y, et al. Rb1 and Trp53 cooperate to suppress prostate cancer lineage plasticity, metastasis, and antiandrogen resistance. Science. 2017;355(6320):78-83.
- Berger A, Brady NJ, Bareja R, et al. N-Myc-mediated reprogramming drives lineage plasticity in advanced prostate cancer. J Clin Invest. 2019;129(9):3924-3940.
- Schweizer MT, Gulati R, Montgomery B, et al. Early effects of androgen deprivation therapy and survival in men with localized prostate cancer: Results from the Scandinavian Prostate Cancer Group-4 trial. J Clin Oncol. 2024;42(16_suppl):5061.