(UroToday.com) The 2025 ASCO annual meeting featured a developmental therapeutics immunotherapy oral abstract session and a presentation by Dr. Ricky Tong discussing clinical responses to SYNC-T therapy and in situ personalized vaccination with intratumoral immunotherapy in patients with metastatic castration-resistant prostate cancer (mCRPC). Prostate cancer is an immunologically “cold” tumor, with low expression of PD-L1, minimal T cell infiltration, low tumor mutational burden, and an immunosuppressive tumor microenvironment. To date, objective response rates to anti-PD-1 therapies are 3-5%, with little to no overall survival benefit. When combining anti-PD-1 therapies with anti-CTLA-4 therapies, objective response rates are still only 0-25%. Moreover, there are significant rates of grade 3 and 4 toxicities (42-53%), with many (26-40%) discontinuing therapy secondary to treatment related adverse events, especially with checkpoint combinations. Currently, our ability to combine targeted biologics is limited because of systemic autoimmune side effects.
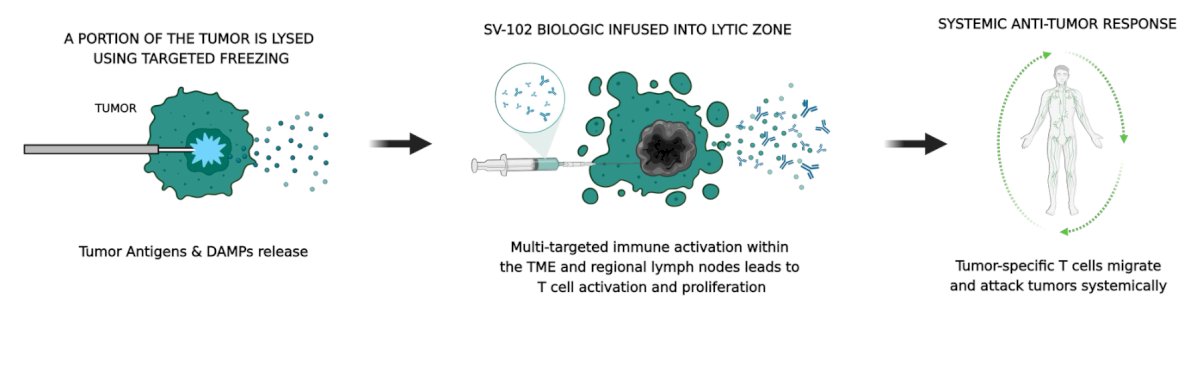
SYNC-T is a novel in situ therapy designed to personalize cancer therapy through partial oncolysis of the subject’s tumor to enhance immune activation. It utilizes antigen release and the multi-target drug approach to both reduce immune suppression and enhance immune activation. The immune therapy is designed to generate a systemic anti-tumor T cell response, and intratumoral targeting allows for low dose administration and high loco-regional concentrations with minimal systemic exposure that results in reduced toxicity:
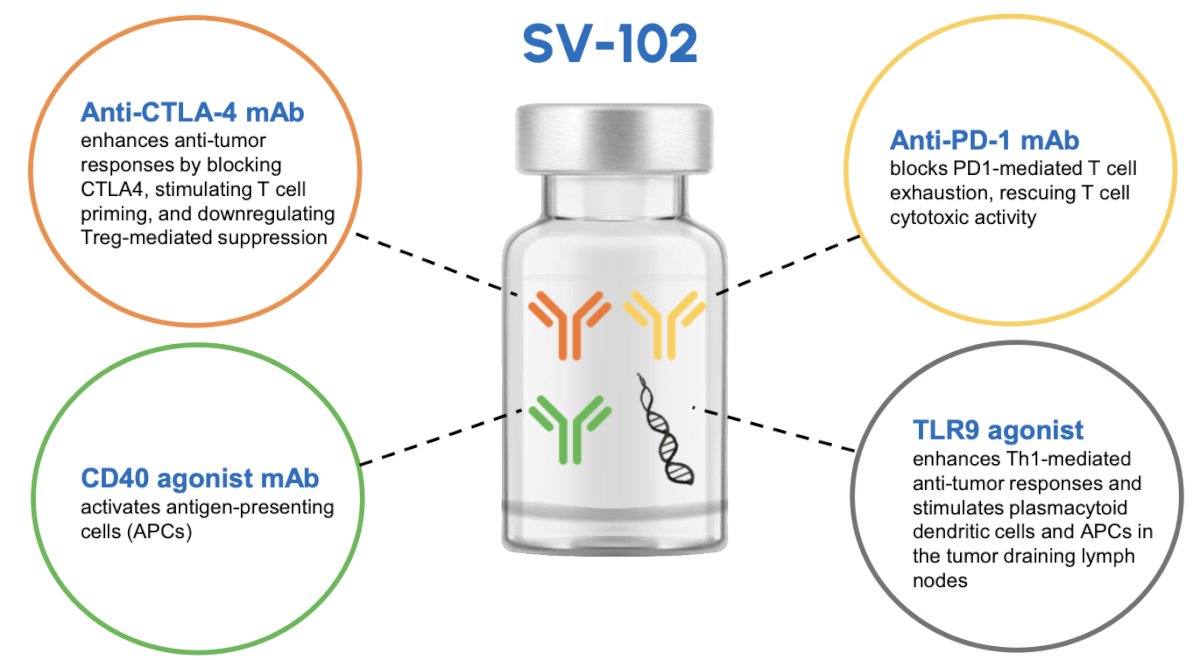
SV-102 is a SYNC-T drug candidate that is a multi-target drug with four active immunotherapeutic ingredients: an anti-CTL4 monoclonal antibody, an anti-PD-1 monoclonal antibody, a CD40 agonist monoclonal antibody, and a TLR9 agonist.
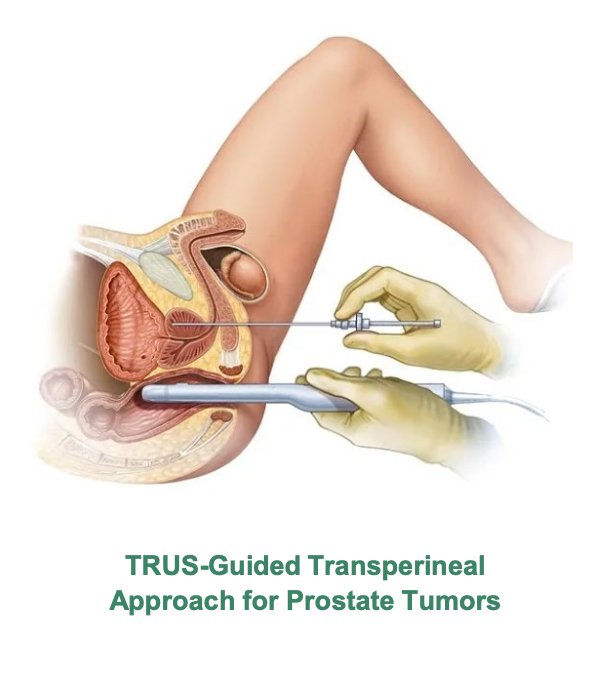
SYNC-T therapy uses clinical procedural skills that are routine for a urologist:
- The procedure employs commonly used a MR and/or transrectal ultrasound for probe placement in the prostate
- Oncolysis is first performed via targeted freezing using the ICESPHERE Cryoablation Needle to generate a ~10 mm ice ball, followed by passive thawing
- After passive thawing, 15 mL of the SV-102 multi-target biologic is infused into the lytic zone at a rate of 3 mL/min
- For soft tissue metastases outside of the prostate that are targeted for oncolysis, the procedure is performed by interventional radiologists using CT or ultrasound guided percutaneous needle placement
The SV-102 phase 1 trial was an investigator initiated trial evaluating the safety and efficacy of SYNC-T therapy SV-102 for mCRPC patients. Key inclusion criteria were as follows:
- Histologically confirmed metastatic prostate cancer
- Failure of previous treatment with one or more approved second generation androgen receptor pathway inhibitors with or without prior chemotherapy or refused hormone therapy
- Measurable disease by RECIST 1.1 criteria
- Soft tissue disease that can be targeted by SYNC-T therapy
Key exclusion criteria were as follows:
- Known other primary malignancy other than prostate cancer that is progressing or has required active treatment in the previous 3 years
- Obstructed urinary system before or after stenting
- Undergone major surgery or local prostate intervention within 28 days prior to SYNC-T cycle
- Active infection requiring systemic therapy
- Received a live vaccine within 30 days prior to enrollment
- Significant cardiac or other medical illness
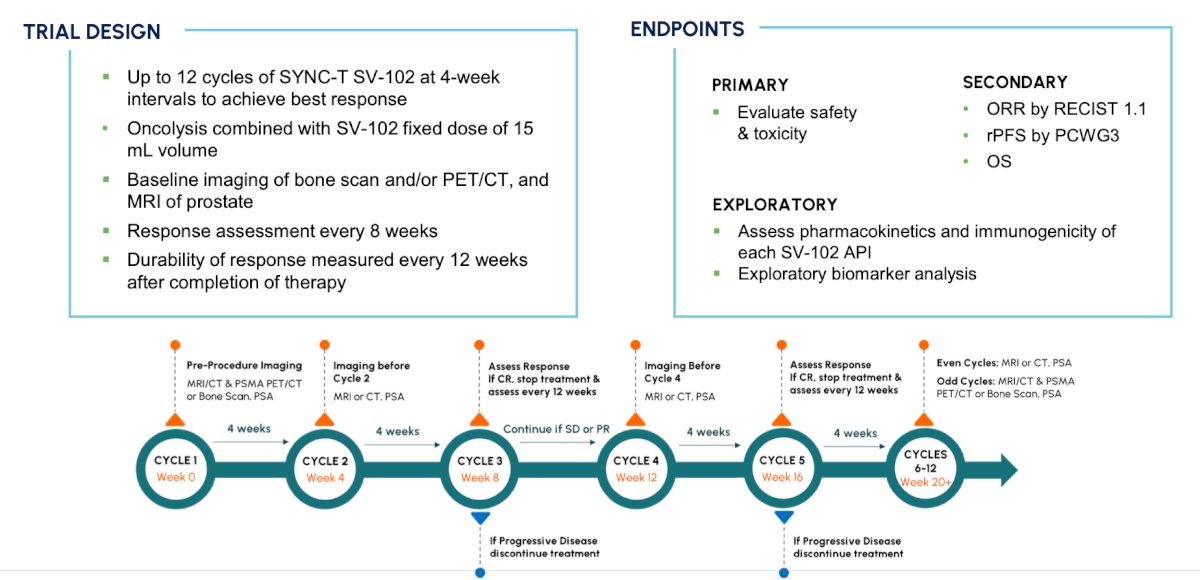
Image-guided partial cryolysis of a tumor was followed by intratumoral infusion of SV-102, comprised of fixed low dose of anti-PD-1 mAb, anti-CTLA4 mAb, CD40 agonist mAb, and TLR9 agonist CpG-ODN. All subjects received the same dose of SV-102. Subjects received SYNC-T Therapy q4 weeks for up to 12 cycles (median = 6). One site of primary prostate or soft tissue metastasis was targeted at each cycle. The primary objective was to evaluate safety and tolerability, with a secondary objective to assess tumor response by PCWG3 and RECIST 1.1. The trial design is as follows:
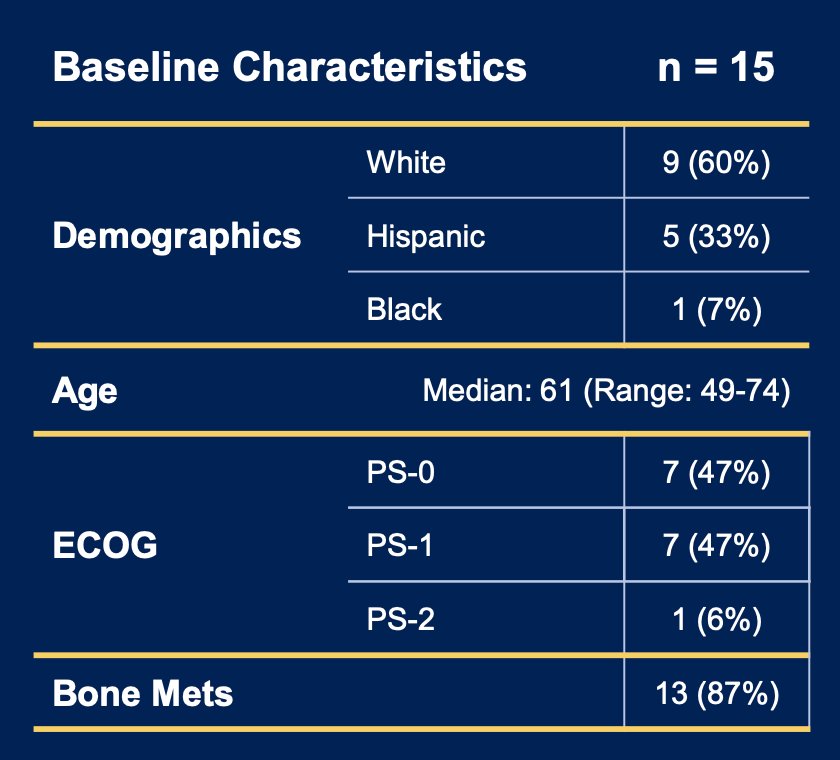
There were 15 subjects, 13 with bone metastases, and documented failure to prior hormonal therapy (n = 10) or refused therapy (n = 5) that were recruited to this single-arm study (NCT05544227). The median age was 61 (range: 49-74), 60% were white, and most were ECOG 0-1:
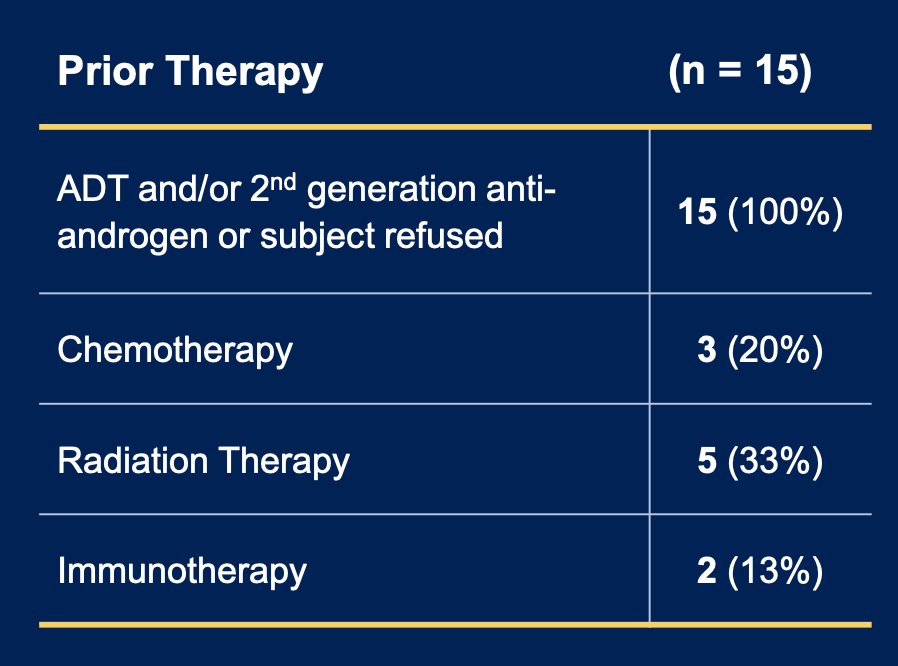
Prior treatments included one or more of 1st, 2nd generation hormonal blockade, chemotherapy, immunotherapy, or radiation therapy:
Within 15 evaluable subjects, there were 8 radiographic complete responses (53%, the two-sided 95% CI is 29.4% to 78.7%, rejecting 20% CR null hypothesis; p = 0.0085) with complete resolution of primary, bone, and soft tissue metastases:

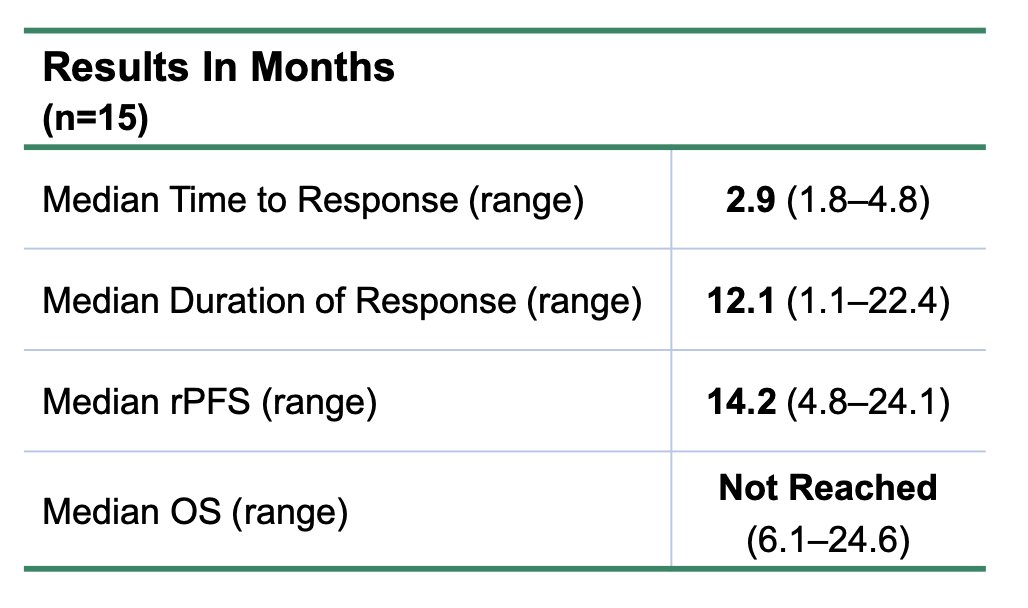
Additionally, 5 partial responses (33%) with an overall response rate of 87%. For PSA results, 47% declined by > 50% or had PSA < 0.02 throughout treatment. Among the 15 subjects, 3 have died resulting in 80% survival with a 17.2 month median follow-up. The
median time to response was 2.9 months (range 1.8-4.8) with a median duration of response of 12.1 months to date (range 1.1-22.4):
The following is a case example of a participant that had complete resolution of > 50 bone metastases after 7 treatment cycles:

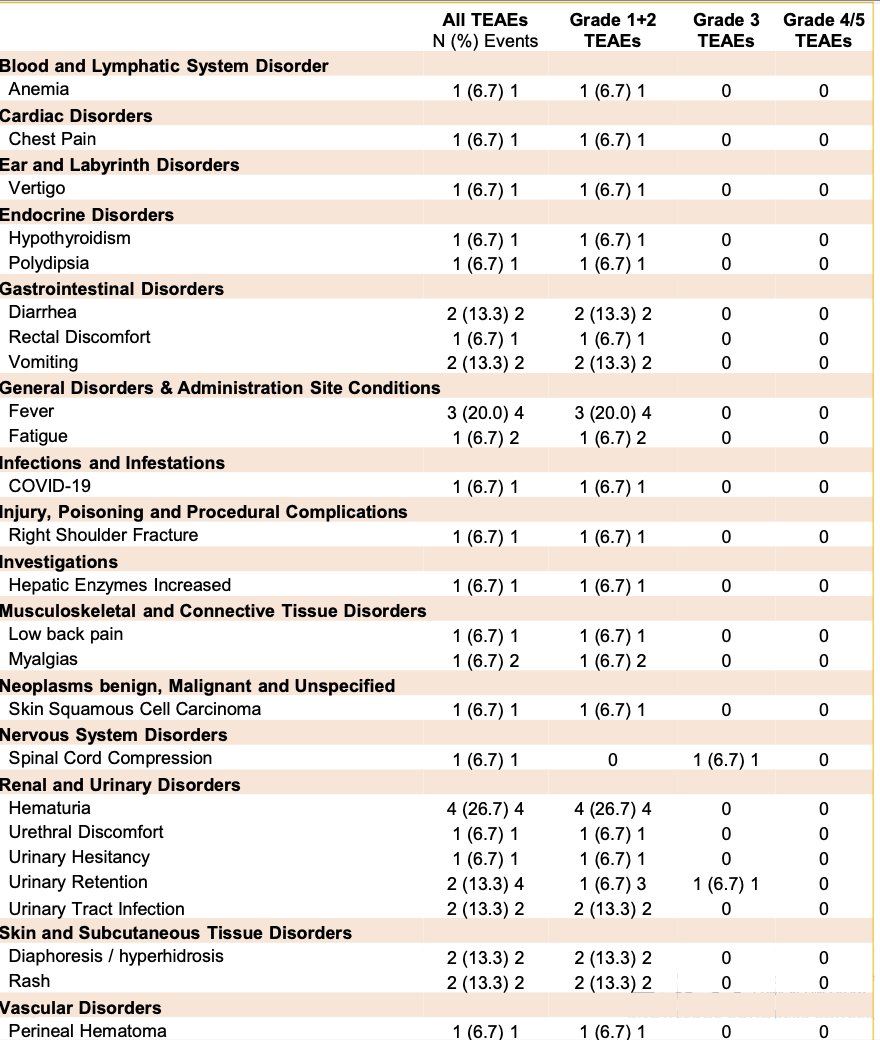
SYNC-T Therapy was well-tolerated, with 41 treatment emergent adverse events in 13 subjects. The majority (95%) of treatment emergent adverse events were grade 1 or 2, most commonly fever and hematuria. There were 2 grade 2 immune related adverse events of hepatitis and hypothyroidism, and 2 grade 3 treatment emergent adverse events of urinary retention and spinal cord compression:
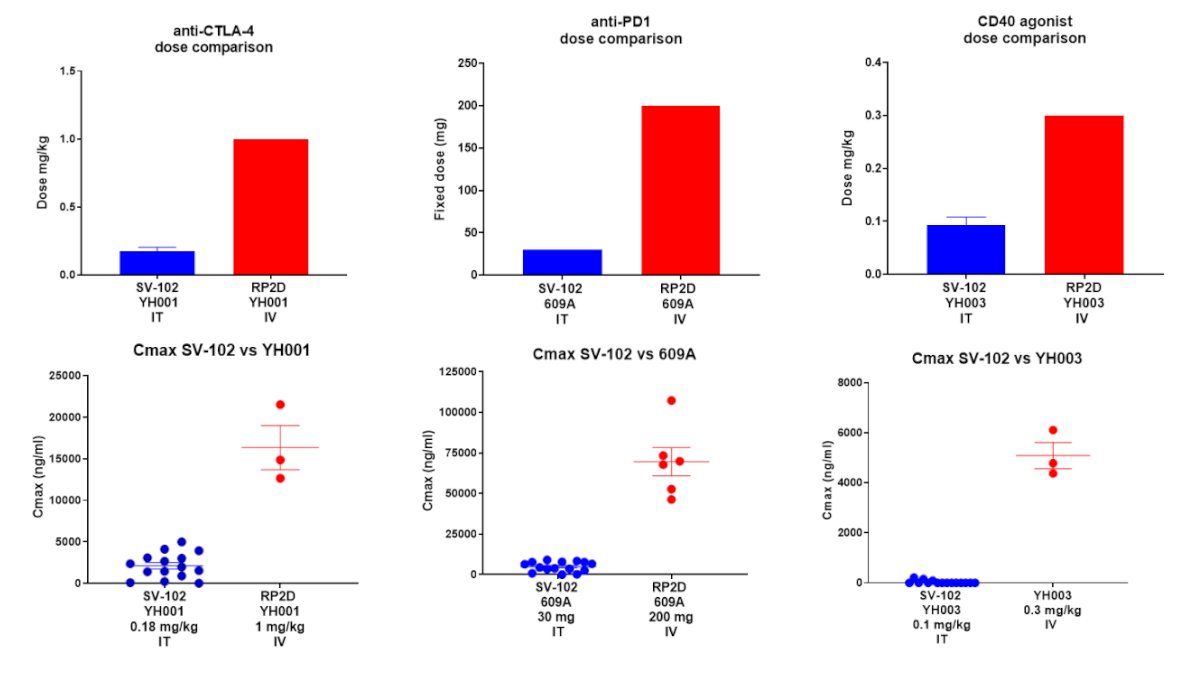
APIs in SV-102 are dosed at much lower levels than the IV recommended phase 2 dose, with much lower systemic exposure:
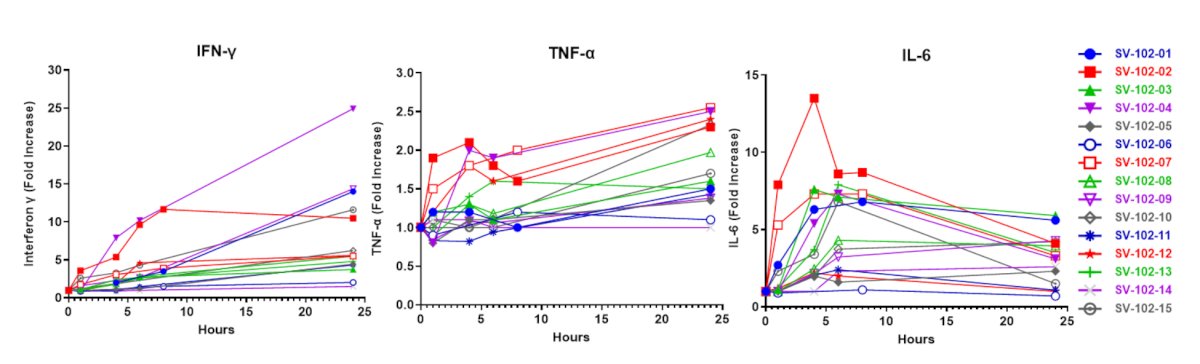
Pro-inflammatory cytokines increased during the first 24 hours after SYNC-T therapy, including IFN-gamma, TNF-alpha, and IL-6, all showing significant increases from pre-treatment:
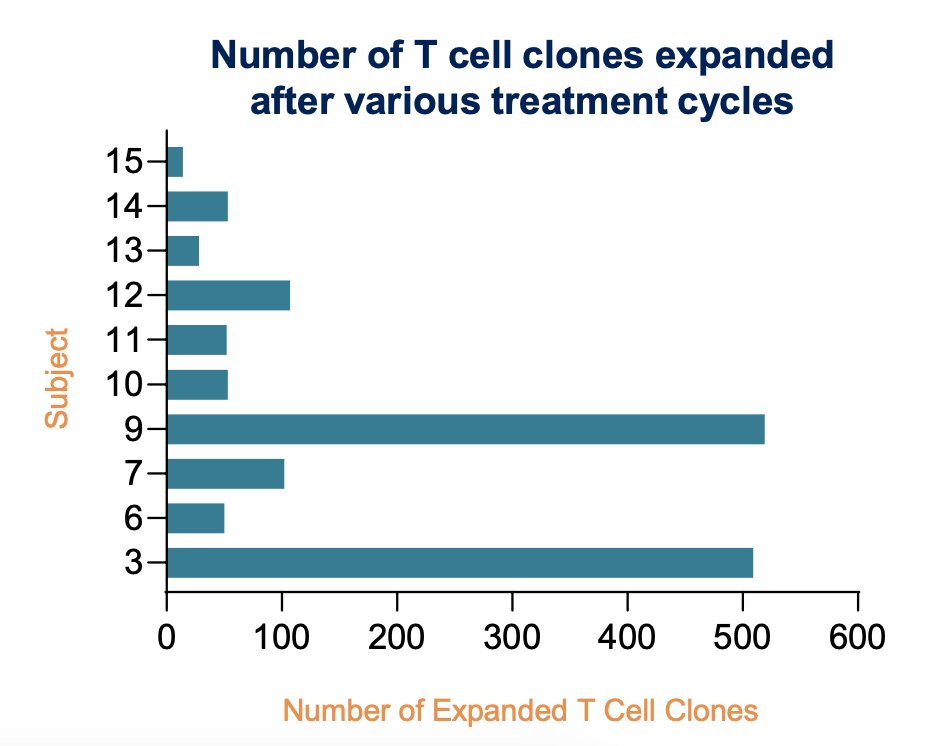
SYNC-T therapy induced a robust peripheral polyclonal T cell expansion, which increased after additional treatment cycles. Data shows expanded TCR-beta clones associated with known MHC-restricted tumor antigens. Further, SYNC-T therapy may drive a positive selection of polyclonal responses against some tumor antigens:
This trial had several limitations, including the small number of subjects treated thus far with SYNC-T therapy SV-102, the single center experience, and a heterogeneous population with both hormone refractory (n = 10) and hormone-naïve (n = 5) patients.
Dr. Tong concluded his presentation discussing clinical responses to SYNC-T therapy and in situ personalized vaccination with intratumoral immunotherapy in patients with mCRPC with the following take home points:
- SYNC-T therapy SV-102 for mCRPC demonstrates highly encouraging clinical activity
- A significant portion of subjects in this pilot study have achieved either a complete response or near complete response with resolution of all bone metastases
- The initial safety data demonstrated no grade 3 or 4 autoimmune adverse events
- The infusion of SYNC-T therapy SV-102 directly into the tumor uses significantly lower doses than delivering immunotherapies systemically via an IV
- A multi-center US phase 2a trial is underway (LEGION-100 trial)
Presented by: Ricky T. Tong, MD, PhD, Lankenau Medical Center, Main Line Health, Penn Wynne, PA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.