(UroToday.com) The 2026 American Urological Association annual meeting featured practice-changing, paradigm-shifting clinical trials in urology and a presentation by Dr. Rana McKay discussing data from ARASEC, a US prospective, open-label, phase 2 study with an external control assessing darolutamide + ADT in metastatic hormone-sensitive prostate cancer (mHSPC).
Why is ARASEC needed? By 2020, combination therapy was the recommended standard of care for mHSPC. Data on darolutamide + ADT in mHSPC were requested by clinicians and patients. Importantly, an ADT control arm was not possible in the USA because ADT was no longer the standard of care. Thus, ARANOTE1 and ARASEC were planned and initiated:

ARASEC is a phase 2, open-label, single-arm study enrolling patients with confirmed mHSPC and no prior systemic therapy. Patients received darolutamide 600 mg orally twice daily + ADT (luteinizing hormone-releasing hormone agonist/antagonist or orchiectomy). The external control arm was derived from 394 patients with mHSPC treated with ADT alone in CHAARTED.2 To remove biases in evaluating outcomes that could arise due to differences in baseline profiles between arms, patients were matched 1:1 using a propensity score summarizing baseline characteristics relevant to disease outcomes. The trial design for ARASEC is as follows:
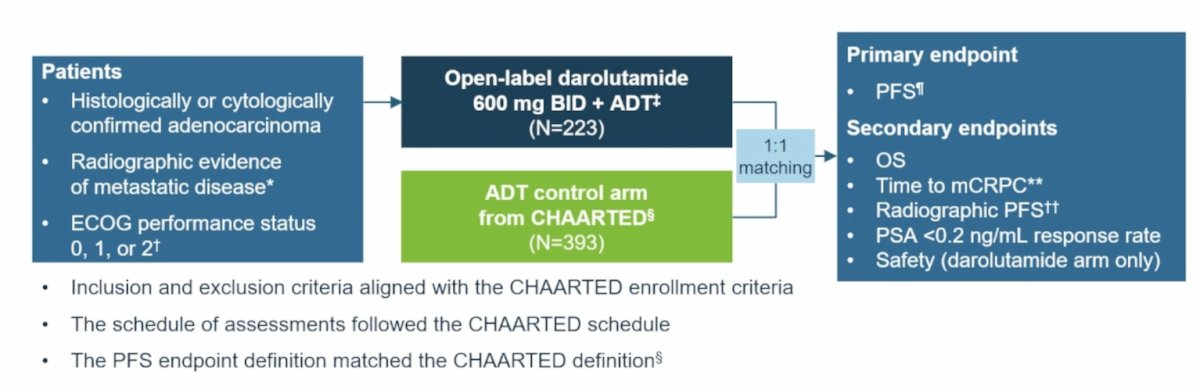
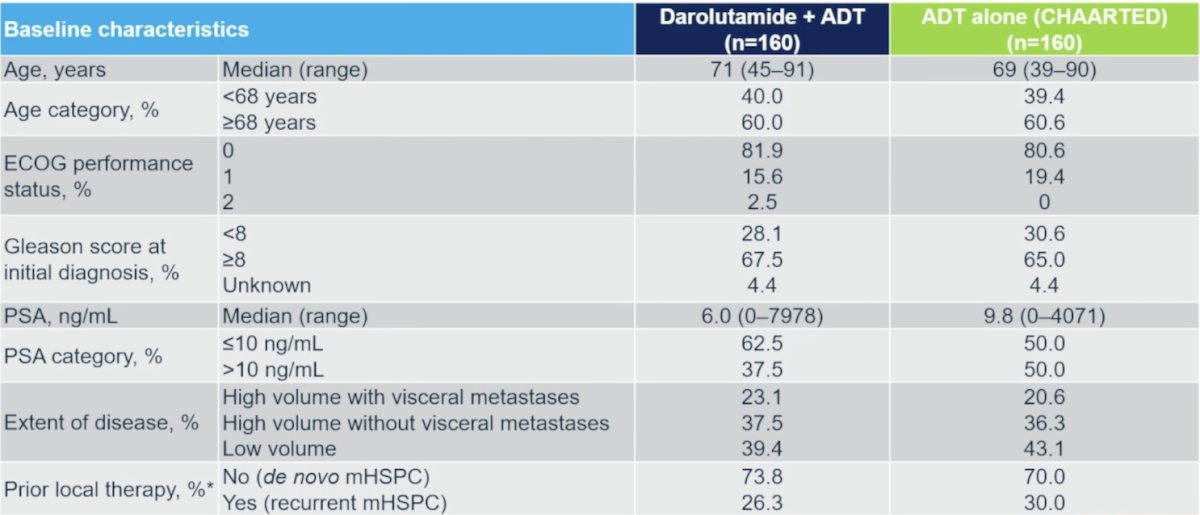
The distribution of propensity scores was based on (i) age (< 68 versus ≥68 years), (ii) ECOG performance status (0 versus >0), (iii) CHAARTED-defined extent of disease (high volume with visceral metastases versus high volume without visceral metastases versus low volume), (iv) prior therapy (yes versus no, as a proxy for recurrent versus de novo disease), (v) Gleason score (<8 versus >=8 versus unknown), and (vi) baseline PSA level (<=10 versus >10 ng/mL). Matching patients with scores within a narrow window across the cohorts ensured that patients in CHAARTED were representative of patients in the darolutamide + ADT arm. The primary endpoint is progression-free survival, as defined in CHAARTED. Secondary endpoints include:
- Overall survival
- Radiographic progression-free survival
- Time to CRPC
- Undetectable PSA response rate (< 0.2 ng/mL) at 6 months
- Safety
Before matching, there were 220 patients in the ARASEC trial and 392 in the CHAARTED control arm. After propensity score matching, there were 160 patients in each arm that were used in the analysis. After matching, baseline characteristics were well balanced in the treatment arms:
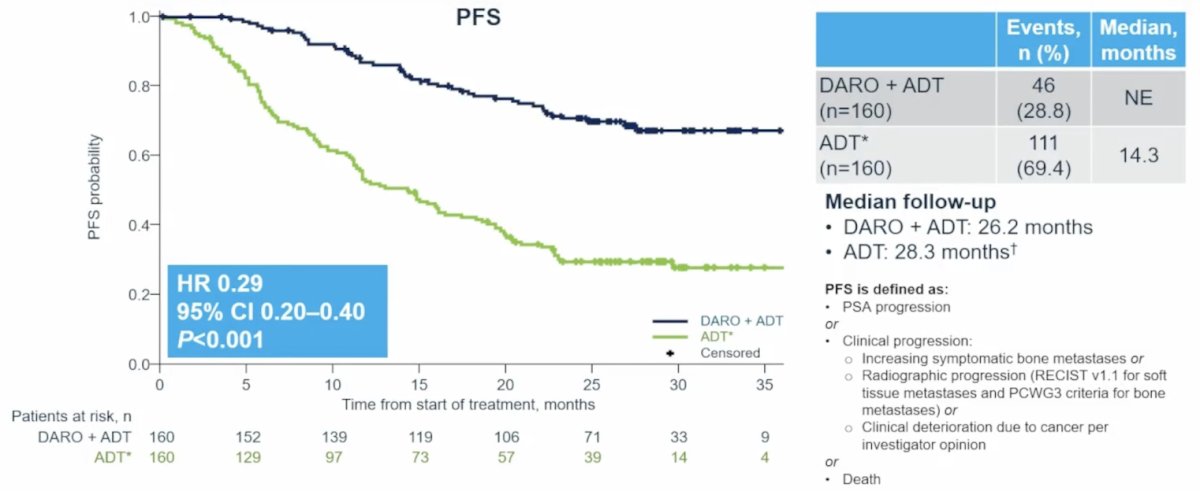
ARASEC met its primary endpoint, demonstrating significantly improved progression-free survival with darolutamide + ADT versus ADT (HR 0.29, 95% CI 0.20-0.40):
Additionally, darolutamide + ADT significantly improved overall survival versus ADT (HR 0.50, 95% CI 0.30-0.82):
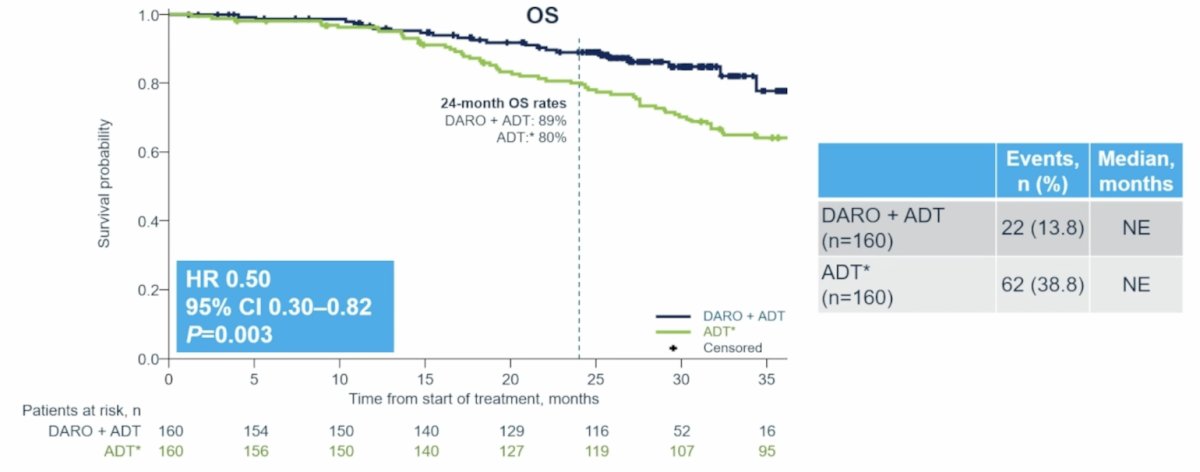
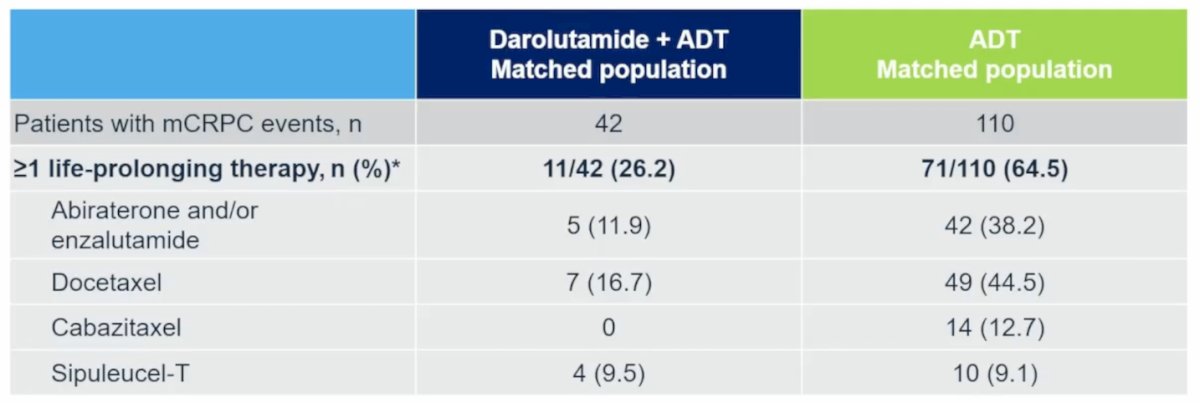
This overall survival benefit was achieved despite proportionally more patients in the ADT arm (65%) versus the darolutamide arm (26%) receiving subsequent life-prolonging therapy:
Darolutamide + ADT also significantly delayed time to mCRPC (HR 0.26, 95% CI 0.18-0.38) and radiographic progression-free survival (HR 0.30, 95% CI 0.19-0.48) versus ADT:

PSA < 0.2 ng/mL response rates were more than doubled in the darolutamide arm versus the ADT arm at all time points assessed:

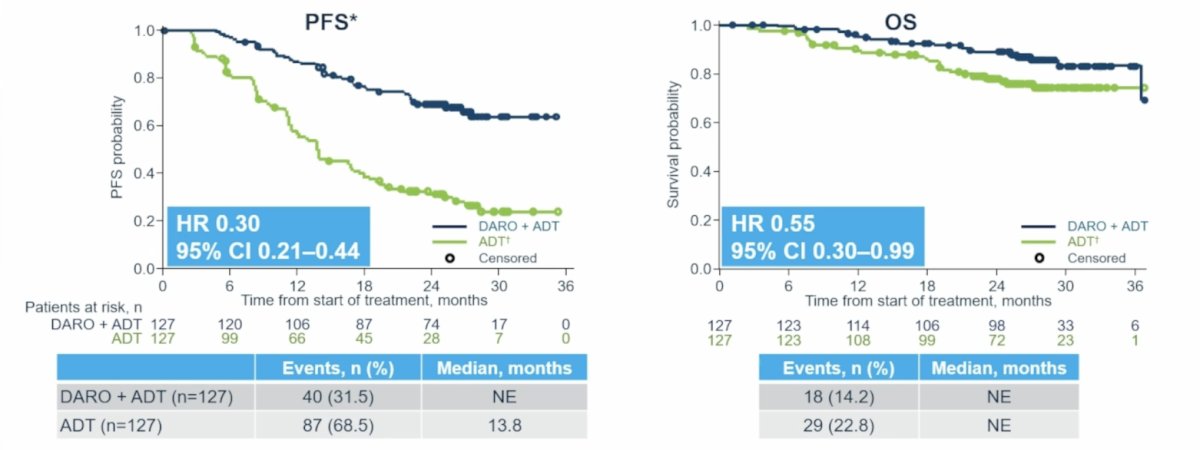
In an effort to address time bias, sensitivity analyses were performed. To answer the question “How does darolutamide + ADT perform versus a contemporary ADT arm?” Dr. McKay and colleagues compared the ARASEC darolutamide arm post hoc with the ARANOTE ADT arm using the same propensity score matching as the primary analysis (n = 127/arm). The sensitivity analysis versus a contemporary phase 3 cohort strongly supports the ARASEC primary findings, with all confidence intervals, including for overall survival, below 1:

Specifically, in the sensitivity analysis versus ARANOTE, darolutamide + ADT prolonged progression-free survival (HR 0.30, 95% CI 0.24-0.44) and overall survival (HR 0.55, 95% CI 0.30-0.99):
A second question is: “Do the outcomes change if we include the matched patients?” To answer this question, Dr. McKay and colleagues performed a prespecified analysis in all enrolled patients in the ARASEC darolutamide arm and CHAARTED ADT arms, using propensity score-based IPTW to adjust for differences in baseline characteristics. The sensitivity analyses in the broader match-eligible population also strongly support the ARASEC primary findings:

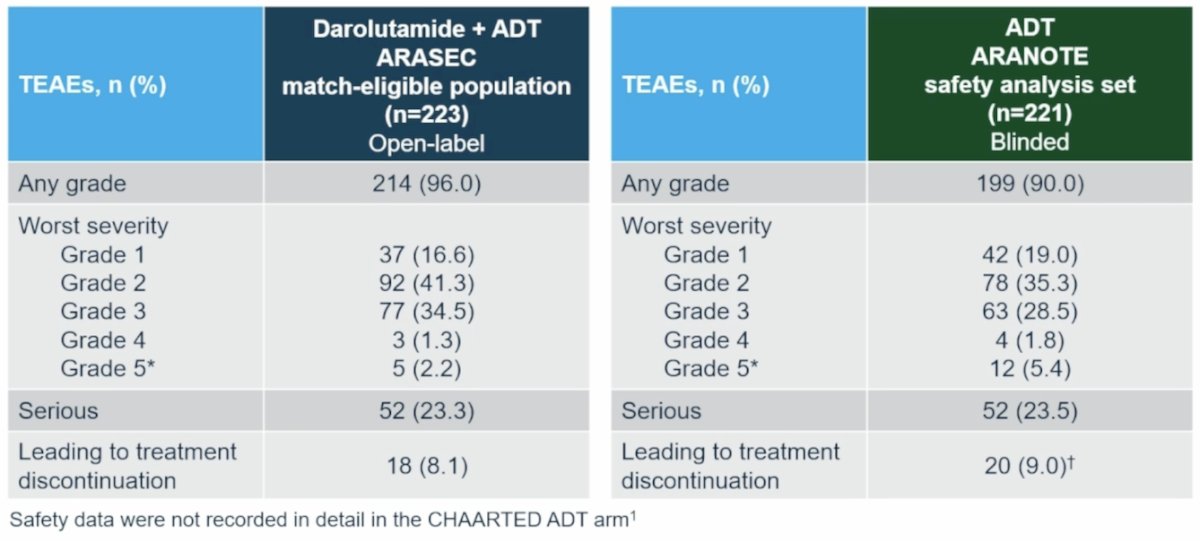
The safety and tolerability profile of darolutamide is in line with the well-established safety profile of darolutamide:
Dr. McKay concluded her presentation discussing data from ARASEC, a US prospective, open-label phase 2 study with an external control assessing darolutamide + ADT in mHSPC, with the following take-home points:
- ARASEC provides further evidence for the efficacy and safety of darolutamide + ADT in mHSPC, reinforcing findings from ARANOTE, in a US population
- Darolutamide + ADT resulted in significant progression-free survival (HR 0.29), overall survival (HR 0.50), and PSA response (p < 0.001) versus ADT alone
- Sensitivity analysis versus a contemporary trial (ARANOTE) control arm strongly supports the robustness of these results
- This is the first study in prostate cancer to use propensity score matching with external phase 3 control arms:
Presented by: Rana McKay, MD, Medical Oncologist, Professor of Medicine and Urology, UC San Diego School of Medicine, San Diego, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Urological Association (AUA) 2026 Annual Meeting, Washington, DC, Fri, May 15 – Mon, May 18, 2026.
References:
- Saad F, Vjaters E, Shore N, et al. Darolutamide in Combination with Androgen-Deprivation Therapy in Patients with Metastatic Hormone-Sensitive Prostate Cancer From the Phase III ARANOTE Trial. J Clin Oncol. 2024 Dec 20;42(36):4271-4281.
- Sweeney CJ, Chen YH, Carducci M, et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med. 2015;373(8):737-746.