(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany was host to a prostate cancer poster session. Dr. Yufan Y. Zhao presented a post hoc analysis of ARASENS evaluating the impact of lead-in androgen deprivation therapy (ADT) on severe neutropenia (grade≥3) secondary to docetaxel in metastatic hormone sensitive prostate cancer (mHSPC) patients.
ADT has been a standard of care for prostate cancer since the 1940s and is recommended across various disease stages, including mHSPC. The addition of docetaxel to ADT has been shown to improve overall survival in mHSPC based on results of the CHAARTED, STAMPEDE trials.1,2 However, docetaxel is associated with clinically significant myelosuppression – grade ≥3 neutropenia and febrile neutropenia (FN) are common and impactful adverse events.
It remains unclear whether lead-in ADT prior to docetaxel initiation can reduce the risk of severe (grade ≥3) neutropenia. In this study, Dr. Zhao and colleagues evaluated the association between lead-in ADT and the incidence of grade ≥3 neutropenia and developed and validated a clinical model to predict cycle-1 grade ≥3 neutropenia risk in men with mHSPC.
The study investigators conducted a post hoc analysis of the phase Ill ARASENS trial (NCT02799602), which randomized men with mHSPC to ADT + docetaxel plus darolutamide versus placebo. Of the 1,306 men with mHSPC enrolled in the ARASENS trial, 847 were included in the final analysis after applying the exclusion criteria (Figure 1).
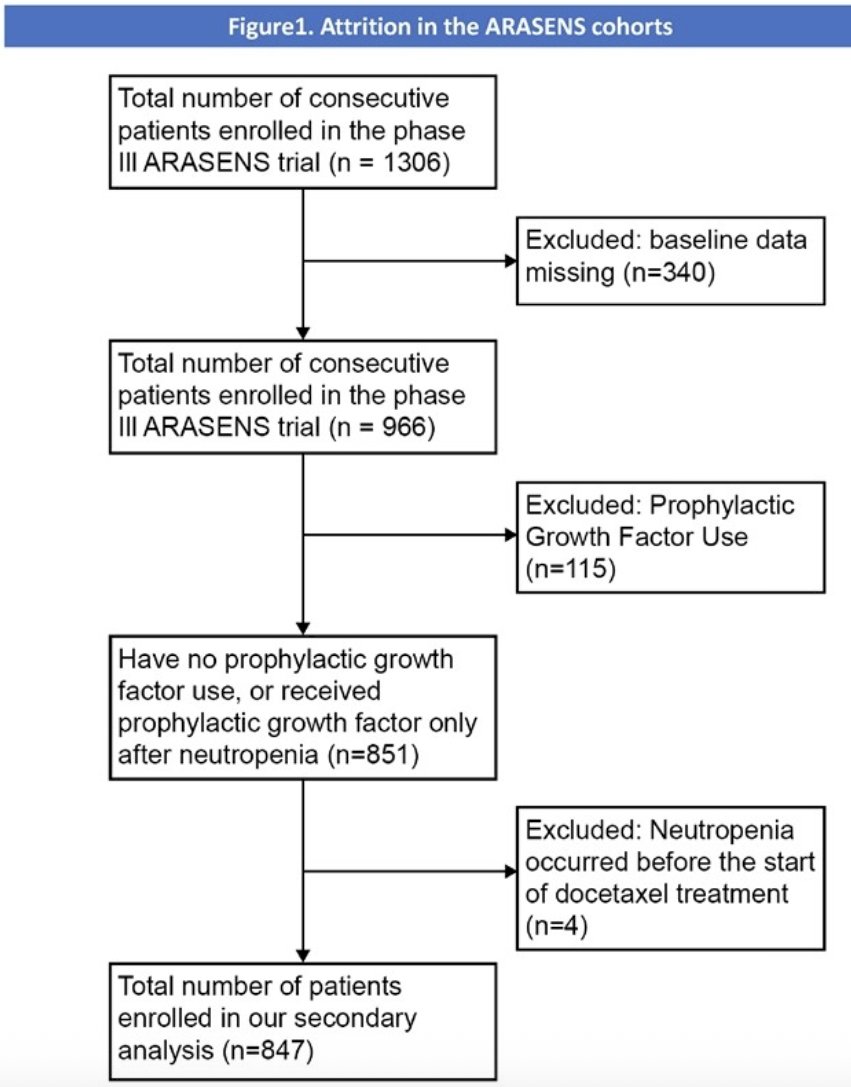
The study investigators divided patients into a lead-in ADT group (initiating ADT before the docetaxel treatment, n=748) and a no lead-in ADT group (initiating on or after the docetaxel treatment, n=99), and compared the incidence of grade ≥3 neutropenia. The primary endpoint was the incidence of grade ≥ 3 neutropenia. The inverse probability treatment weighting (IPTW) method was used to the balance baseline characteristics of the two groups.
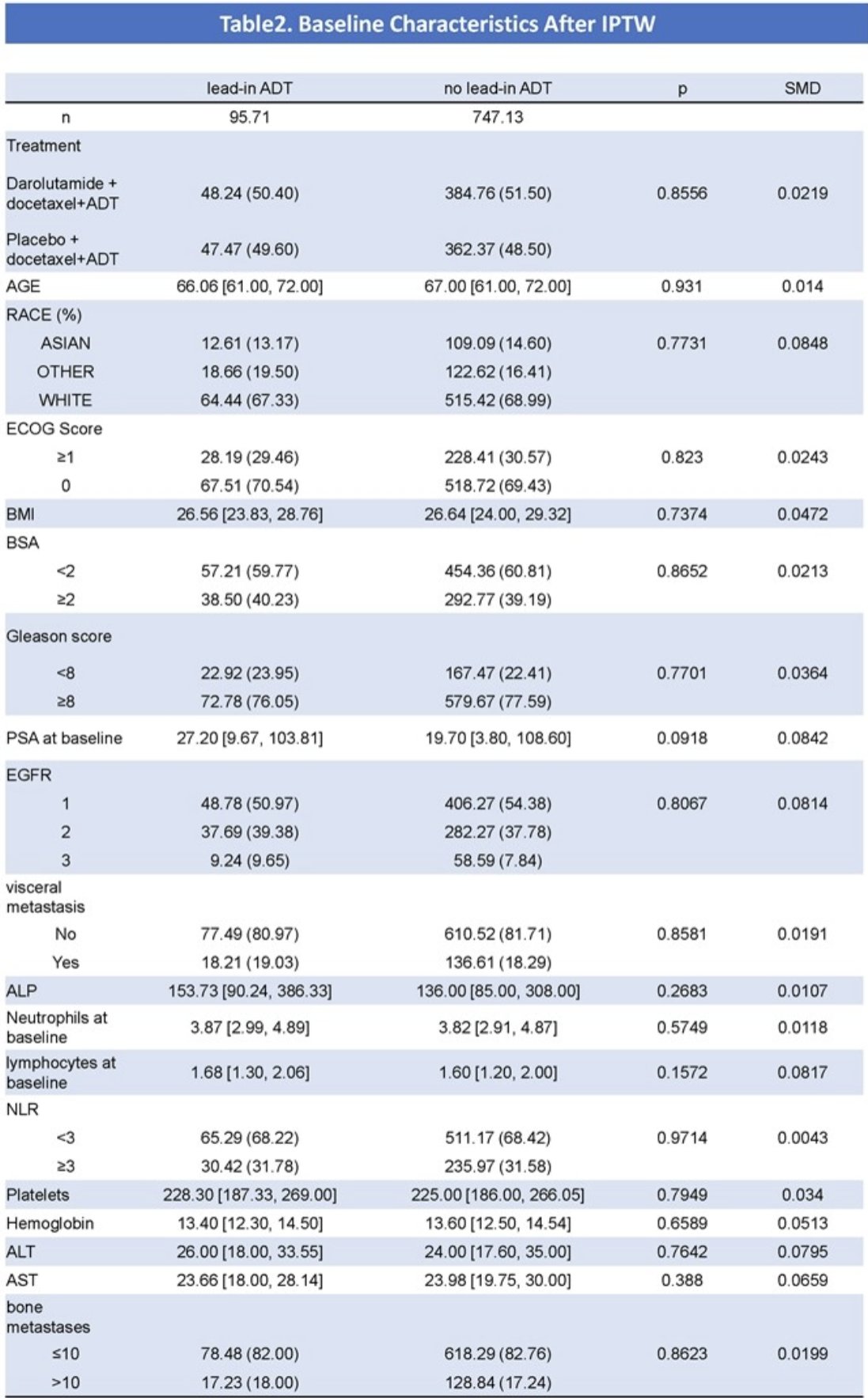
847 patients were enrolled – 748 patients with lead-in ADT and 99 patients without lead-in ADT. The baseline characteristics after IPTW are summarized below.
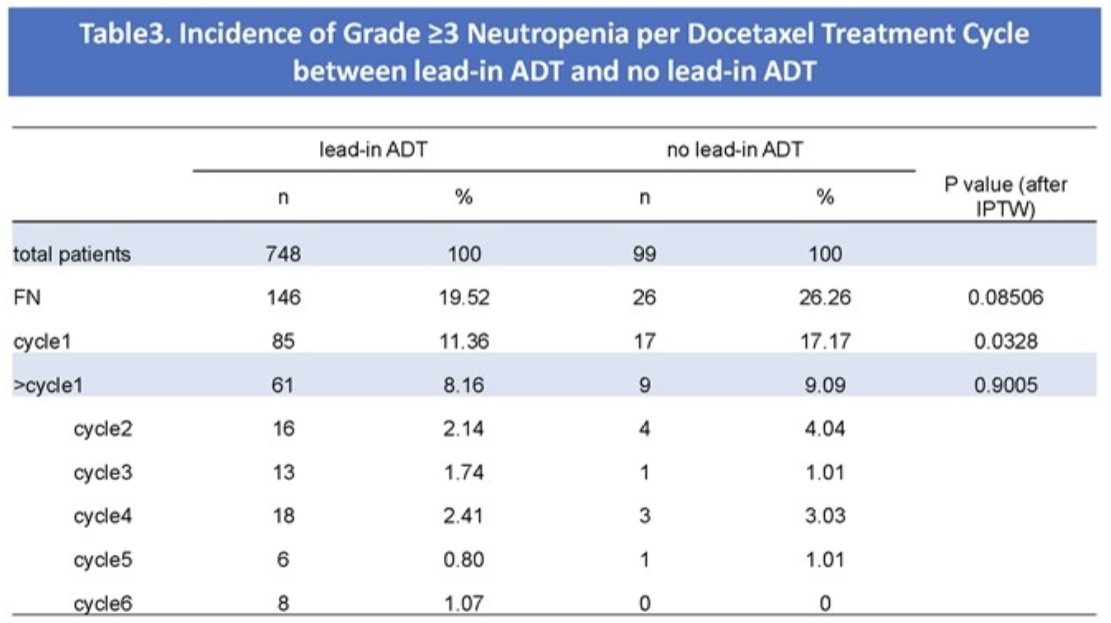
The incidence of grade ≥3 neutropenia after the 1st cycle was significantly lower among patients receiving lead-in ADT (11.4% vs. 17.2%, p=0.03).
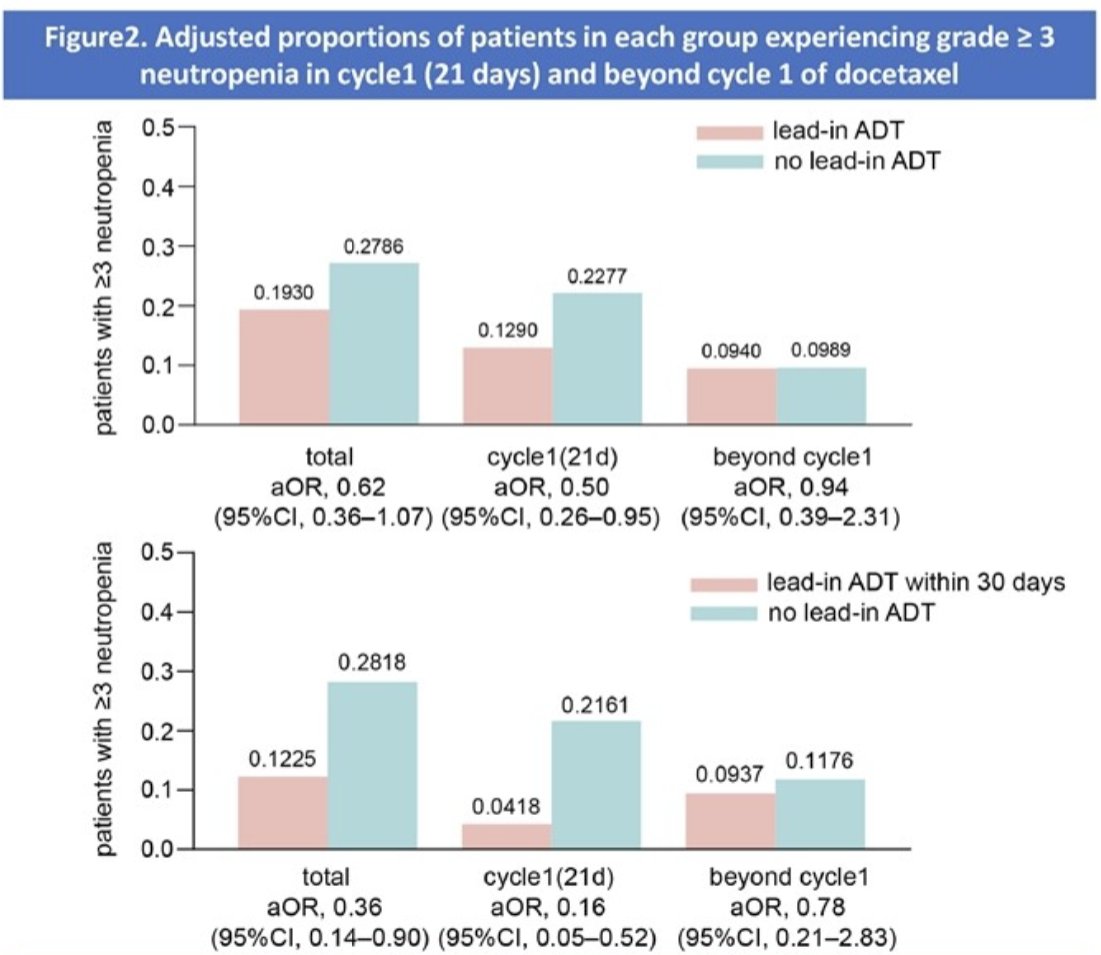
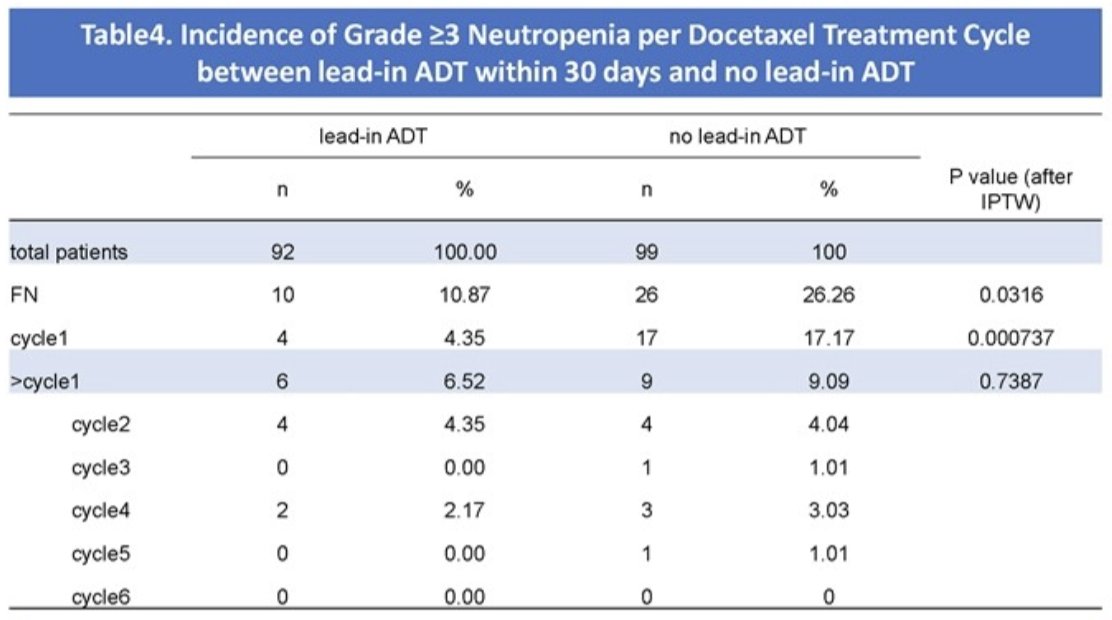
On subgroup analysis, patients receiving lead-in ADT within 30 days were less likely to experience grade ≥ 3 neutropenia compared to patients with no lead-in ADT, especially in the first docetaxel cycle (4% vs 17.2%, p=0.0007).
The cohorts were split into training and testing sets based on the treatment categories in ARASENS. The clinical predictive model demonstrated high performance and calibration for predicting grade ≥ 3 neutropenia in the first cycle in the test cohort (AUC=0.718) and the test cohort (AUC=0.76).

Dr. Zhao concluded that patients receiving lead-in ADT, especially within 30 days, had a lower incidence of grade ≥3 neutropenia in the first cycle compared to patients not receiving lead-in ADT, which contributes to better grade ≥3 neutropenia prevention in cycle 1 of docetaxel treatment for patients.
Presented by: Dr. Yufan Y. Zhao, Department of Urology, Fudan University Shanghai Cancer Center, Shanghai, China
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Sweeney CJ, Chen YH, Carducci M, et al. Chemohormonal Therapy in Metastatic Hormone-Sensitive Prostate Cancer. N Engl J Med. 2015; 373(8):737-746.
- James ND, Sydes MR, Clarke NW, et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet. 2016; 387(10024):1163-1177.
- Smith MR, Hussain M, Saad F, et al. Darolutamide and Survival in Metastatic, Hormone-Sensitive Prostate Cancer. N Engl J Med. 2022; 386(12):1132-1142.