(UroToday.com) The 2026 ASCO GU Annual Symposium was host to a prostate cancer poster session. Dr. Pedro Barata presented an analysis of real-world patient characteristics and treatment patterns among metastatic castration-resistant prostate cancer (mCRPC) patients treated with talazoparib + enzalutamide in the United States.
In June 2023, the US Food and Drug Administration (FDA) approved talazoparib plus enzalutamide for patients with homologous recombination repair gene-mutated (HRRm) mCRPC.1 The TALAPRO-2 trial demonstrated significant radiographic progression-free survival and overall survival benefit with this combination.2 HRR mutations are present in approximately 20–25% of patients with mCRPC and may result in poor prognosis.3 However, there is limited real-world evidence evaluating HRRm testing and treatment patterns among patients with mCRPC treated with talazoparib plus enzalutamide in the United States.
The study objective was to assess the clinical characteristics, treatment patterns, and homologous recombination repair mutation (HRRm) testing among patients with mCRPC treated with talazoparib plus enzalutamide in a US real-world setting.
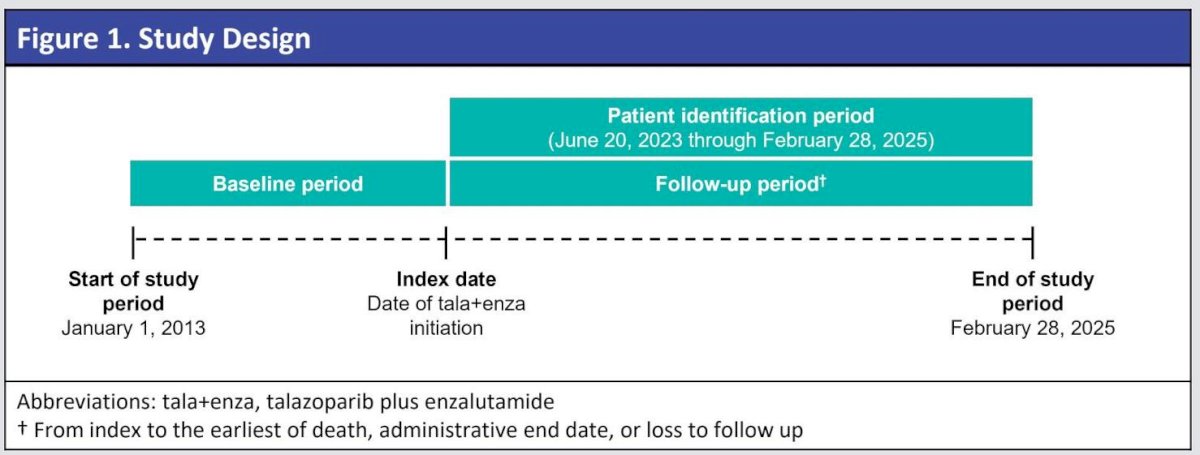
This was a non-interventional, retrospective cohort study of US patients with mCRPC using the nationwide Flatiron Health electronic health record–derived database, which includes data from over 280 oncology clinics (~800 sites of care). The study cohort included adult male patients with a diagnosis of mCRPC who initiated talazoparib plus enzalutamide between June 20, 2023, and February 28, 2025.
Descriptive statistics were used to summarize demographic and clinical characteristics, treatment patterns, and HRRm gene testing.
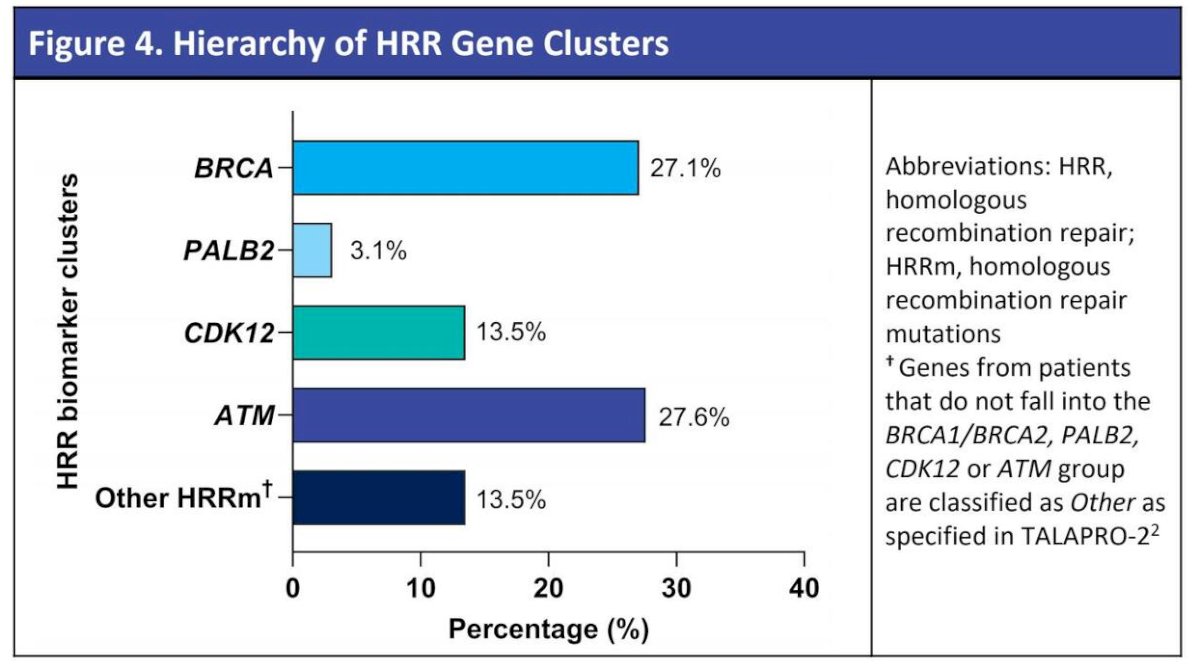
HRR gene clustering hierarchy was used to classify patients into specific groups consistent with TALAPRO-2:
- BRCA cluster (BRCA1/2)
- PALB2 cluster
- CDK12 cluster
- ATM cluster
- Other HRR genes
Follow-up extended from the index date until the earliest of death, administrative censoring, or loss to follow-up.
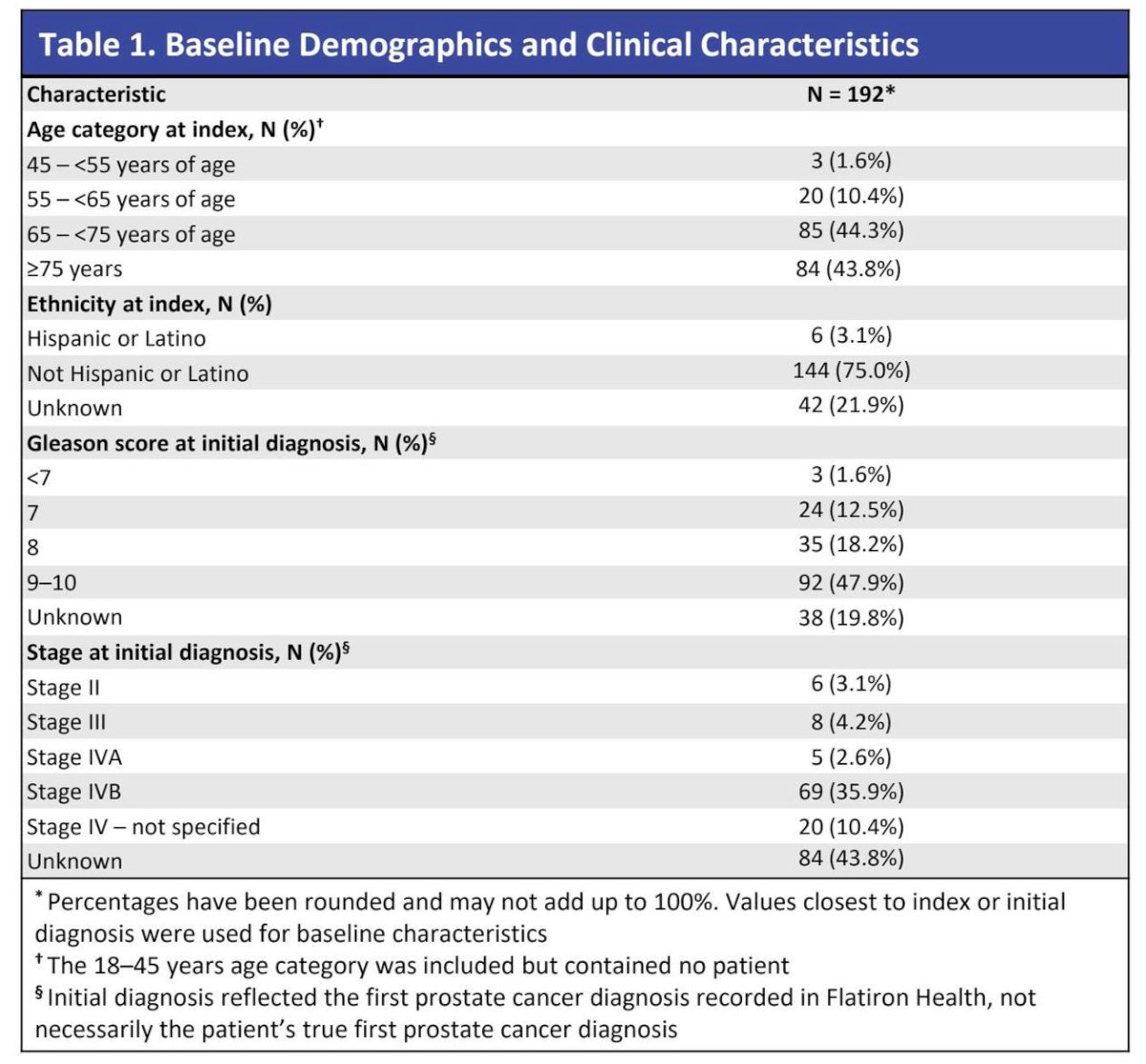
A total of 192 patients with mCRPC treated with talazoparib plus enzalutamide were identified.
- Median age: 73 years (Q1–Q3: 69–80)
- 43.8% were ≥75 years
- 75.0% were non-Hispanic/Latino
- At initial prostate cancer diagnosis, nearly half (47.9%) had Gleason score of 9 or 10
The median follow-up from initiation of talazoparib plus enzalutamide was 8.2 months (IQR: 4.9–12.0).
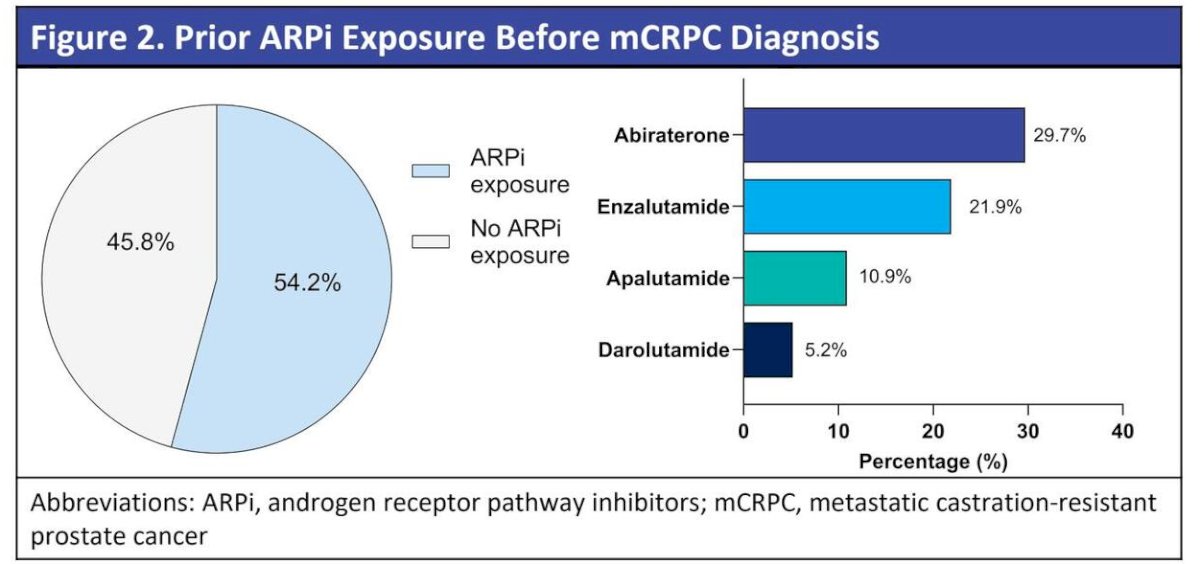
54.2% received prior androgen receptor pathway inhibitors (ARPIs):
- Abiraterone: 29.7%
- Enzalutamide: 21.9%
- Apalutamide: 10.9%
- Darolutamide: 5.2%
Additionally, 10.9% received docetaxel prior to mCRPC diagnosis.
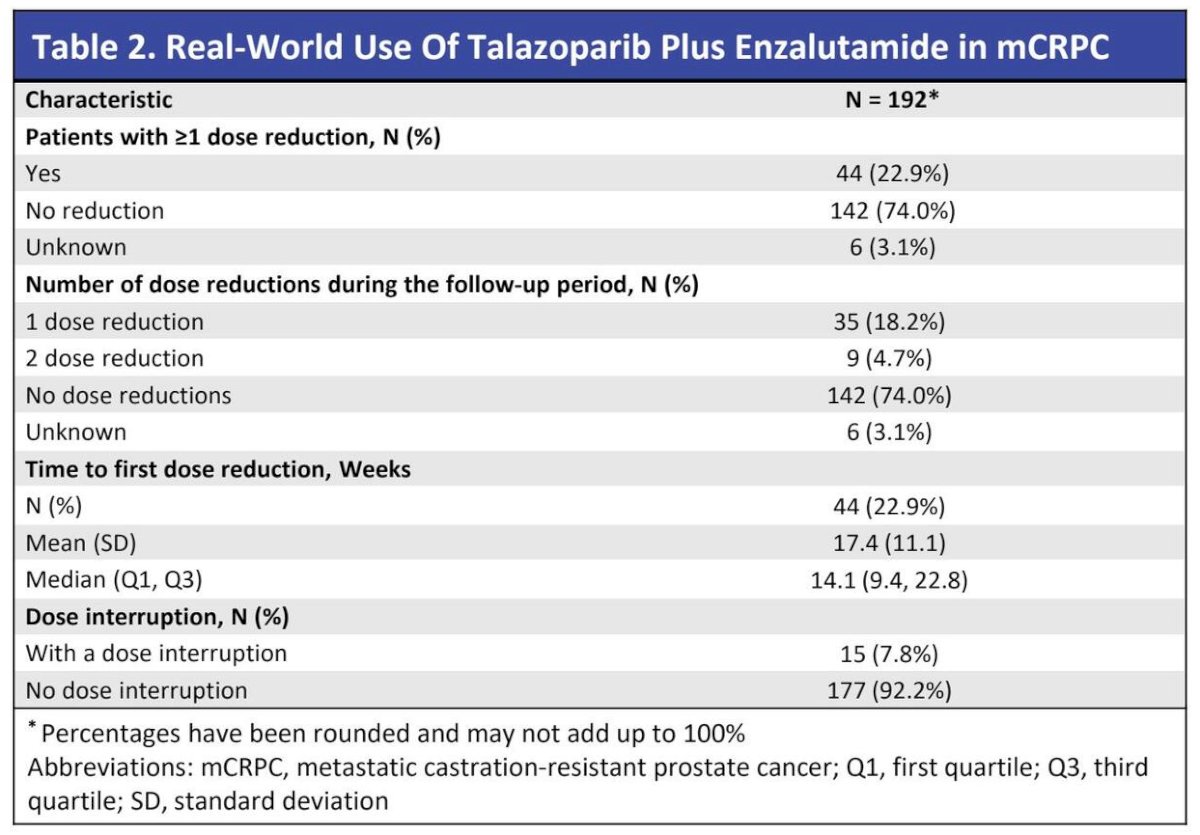
Dose modifications were as follows:
- 22.9% required ≥1 dose reduction
- 74% had no dose reduction
- Median time to first dose reduction: 14.1 weeks
- 7.8% experienced dose interruption
These findings suggest generally manageable tolerability in early real-world use.
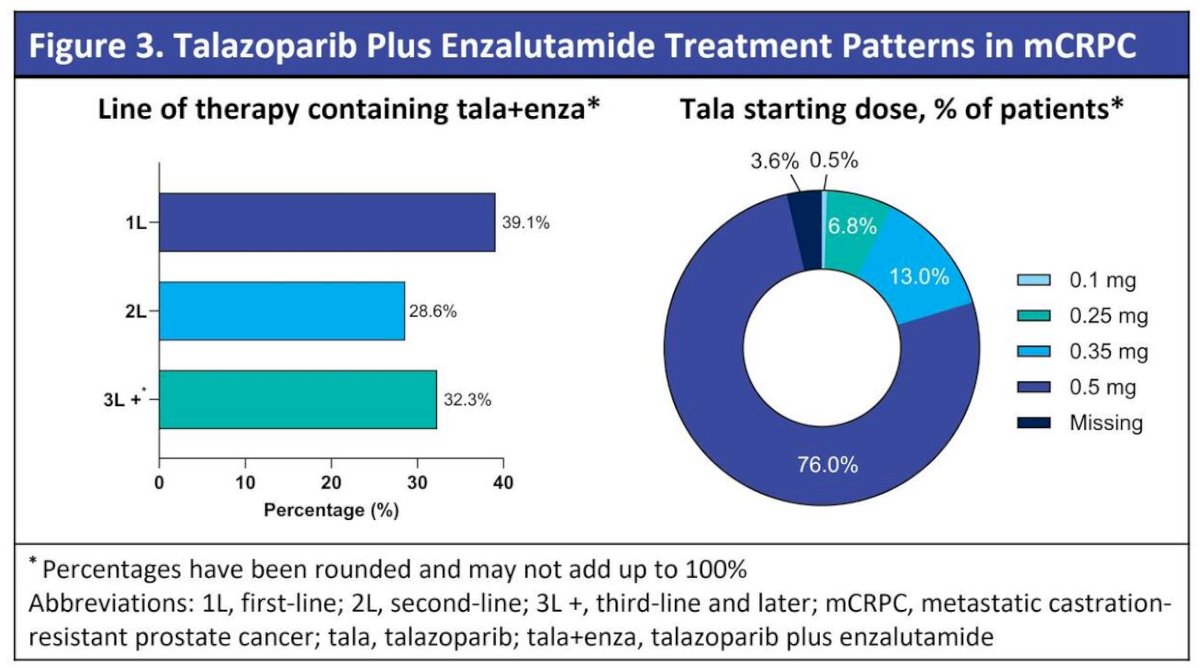
Talazoparib plus enzalutamide was initiated in the following settings:
- 1L mCRPC: 39.1%
- 2L: 28.6%
- 3L+: 33.2%
Starting dose distribution:
- 0.5 mg: 76.0%
- 0.35 mg: 13.0%
- 0.25 mg: 6.8%
- 0.1 mg: 3.6%
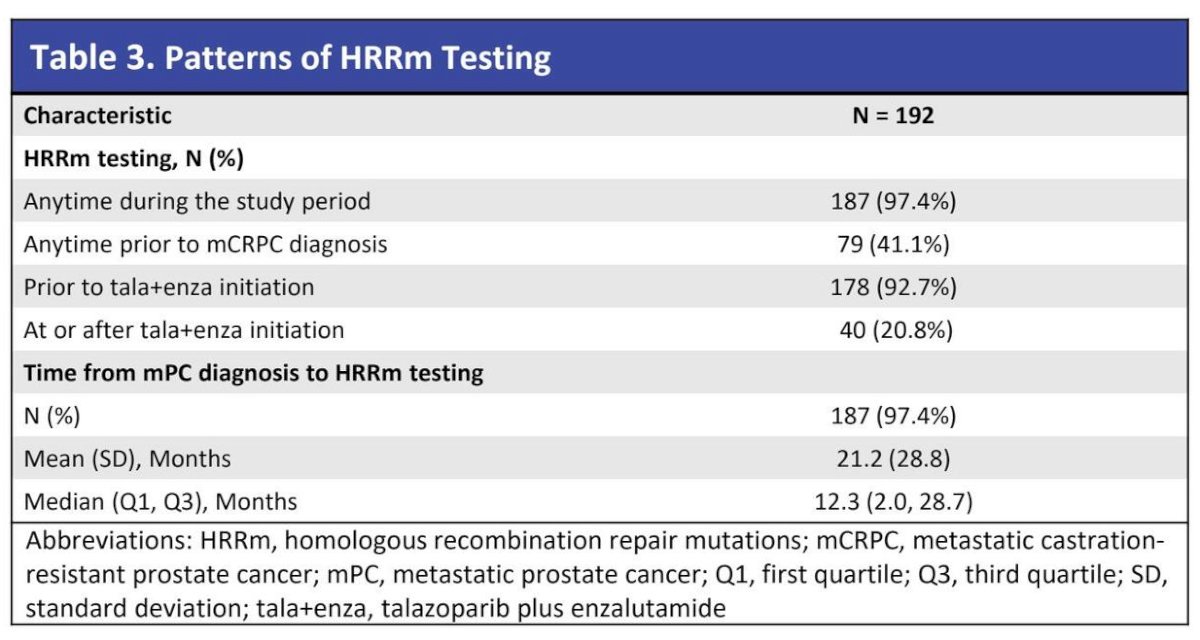
- 92.7% had documented HRRm testing prior to talazoparib + enzalutamide initiation
- 41.1% had documented HRRm mutations
- 74.1% tested prior to mCRPC diagnosis
- 20.8% tested after talazoparib + enzalutamide initiation
Among patients initiating talazoparib plus enzalutamide, HRR gene mutations were as follows:
- ATM: 27.6%
- BRCA: 27.1%
- CDK12: 13.5%
- Other HRRm: 13.5%
- 15.1% had no documented positive mutation or test prior to initiation
Notable limitations were as follows:
- Median follow-up of 8.2 months limits long-term outcome assessment
- Generalizability outside the US community oncology settings may be limited
- Early-treated or externally treated patients may not have been fully captured
Dr. Barata concluded as follows:
- This is the first real-world study to examine treatment patterns of patients treated with talazoparib + enzalutamide and HRRm testing using a US electronic health record database
- More than half (54.2%) of patients received androgen receptor pathway inhibitors prior to mCRPC diagnosis
- In a real-world setting, most patients (60.9%) received talazoparib + enzalutamide as a second-line or later therapy and the majority of patients (92.7%) had documented HRRm testing prior to talazoparib + enzalutamide initiation
- In this real-world study, the most common HRRm clusters in patients with mCRPC who were treated with talazoparib + enzalutamide were BRCA (27.1%) or ATM (27.6%)
- This study highlights the heterogeneous treatment and HRRm testing patterns among patients with mCRPC treated with talazoparib + enzalutamide; future studies should assess clinical outcomes when follow-up permits
Presented by: Pedro C. Barata, MD, MSc, Associate Professor at University Hospitals Seidman Cancer Center, Cleveland, OH
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center, Tucson, AZ – @rksayyid on X during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References
- U.S. Food and Drug Administration. FDA approves talazoparib with enzalutamide for HRR gene-mutated metastatic castration-resistant prostate cancer. Silver Spring (MD): U.S. FDA; 2023.
- Smith MR, Sandhu SK, Kelly WK, et al. Talazoparib plus enzalutamide in metastatic castration-resistant prostate cancer. N Engl J Med. 2023;388(19):1795-1806.
- Mateo J, Carreira S, Sandhu S, et al. DNA-repair defects and olaparib in metastatic prostate cancer. N Engl J Med. 2015;373(18):1697-1708.