(UroToday.com) The 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, was host to the Poster Session A: Prostate Cancer. Dr. Neeraj Agarwal presented Poster 194: Estimated net benefit of talazoparib + enzalutamide for patients with mCRPC using a Q-TWiST analysis.
As Dr. Agarwal reviewed, TALAPRO-2 previously demonstrated significantly prolonged radiographic progression-free survival and overall survival with TALA + ENZA compared with PBO + ENZA in both the unselected population (cohort 1) and in patients with homologous recombination repair mutations (HRRm; cohort 2).1 While long-term safety and patient-reported outcomes have been reported, this analysis aimed to contextualize clinical benefit using a quality-adjusted survival framework.
TALAPRO-2 is a phase 3, randomized, double-blind, placebo-controlled trial evaluating talazoparib plus enzalutamide in adults with asymptomatic or mildly symptomatic mCRPC receiving ongoing ADT. Patients were randomized 1:1 to talazoparib 0.5 mg once daily plus enzalutamide 160 mg once daily or placebo plus enzalutamide. The unselected population (cohort 1), which included patients regardless of HRR alteration status, was enrolled first. Patients with HRR gene alterations from this group were then combined with additional HRR-altered patients to form the HRR-deficient population (cohort 2). The primary endpoint was radiographic progression-free survival by blinded independent central review using RECIST 1.1 and PCWG3 criteria. Overall survival was a key alpha-protected secondary endpoint, along with patient-reported outcomes and safety. The study design is shown below.
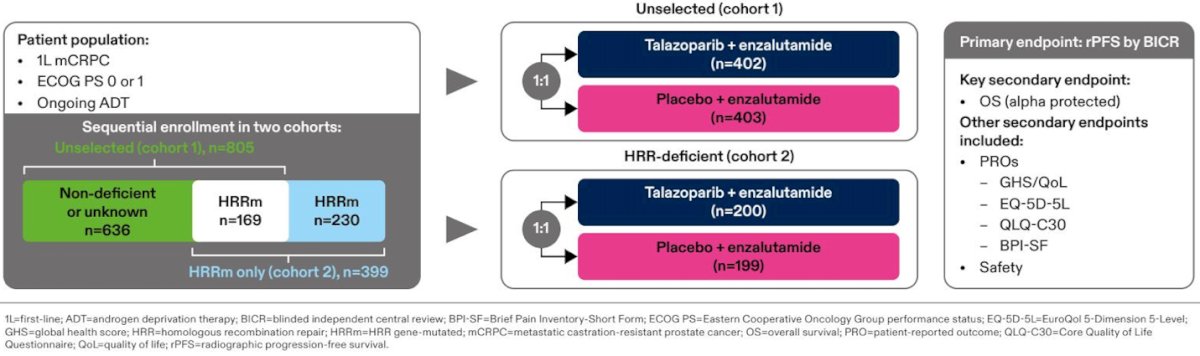
This analysis included the intention-to-treat unselected population (402 patients in the talazoparib arm and 403 in the placebo arm) and the HRR-deficient population (200 and 199 patients, respectively). Using restricted mean survival time at 64 months of follow-up, overall survival was partitioned into three health states: time with grade 3–4 adverse events prior to progression (TOX), time without symptoms of progression or significant toxicity (TWiST), and time after radiographic progression prior to death (REL). This approach provides a more granular assessment of treatment benefit by balancing efficacy and toxicity over time.
Dr Agarwal highlighted that utility values were derived from individual EQ-5D-5L responses collected in the study population. A threshold analysis was performed using a hypothetical range of utility weights to test the robustness of results across different assumptions. Time spent in each predefined health state was weighted by its corresponding utility and then summed to generate quality-adjusted time without symptoms or toxicity (Q-TWiST). Mean between-treatment differences were calculated for each health state, and bootstrapping methods were used to estimate confidence intervals for both means and mean differences. A positive mean between-treatment difference indicated a net clinical benefit for talazoparib plus enzalutamide compared with enzalutamide alone.
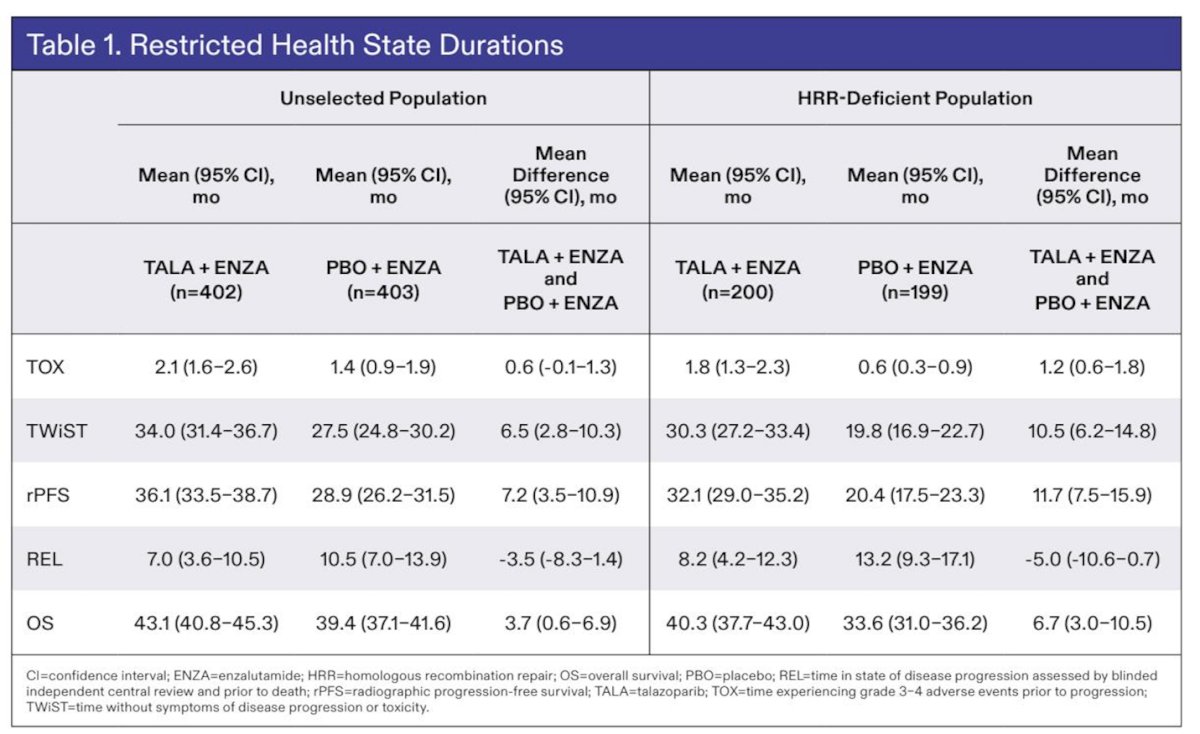
In both cohorts, time spent in TOX was slightly longer with TALA + ENZA compared with PBO + ENZA. However, time spent in TWiST was substantially longer with TALA + ENZA. In the unselected cohort, mean TWiST was 34.0 months with TALA + ENZA versus 27.5 months with PBO + ENZA, representing a mean difference of 6.5 months. In the HRRm cohort, TWiST was 30.3 months versus 19.8 months, with a mean difference of 10.5 months. (Table below)
In both populations, time in the REL state was shorter with talazoparib plus enzalutamide, largely driven by patients spending more time progression-free. Overall survival was numerically longer in the talazoparib combination arm compared with enzalutamide alone across both cohorts.
A threshold utility analysis was conducted using both hypothetical and trial-derived utility values to test the robustness of the Q-TWiST findings. At one extreme, the model assumed severe quality-of-life impairment prior to progression but no impact after progression (TOX weight = 0; REL weight = 1). At the opposite extreme, the model assumed no quality-of-life impact before progression but severe impairment after progression (TOX weight = 1; REL weight = 0).
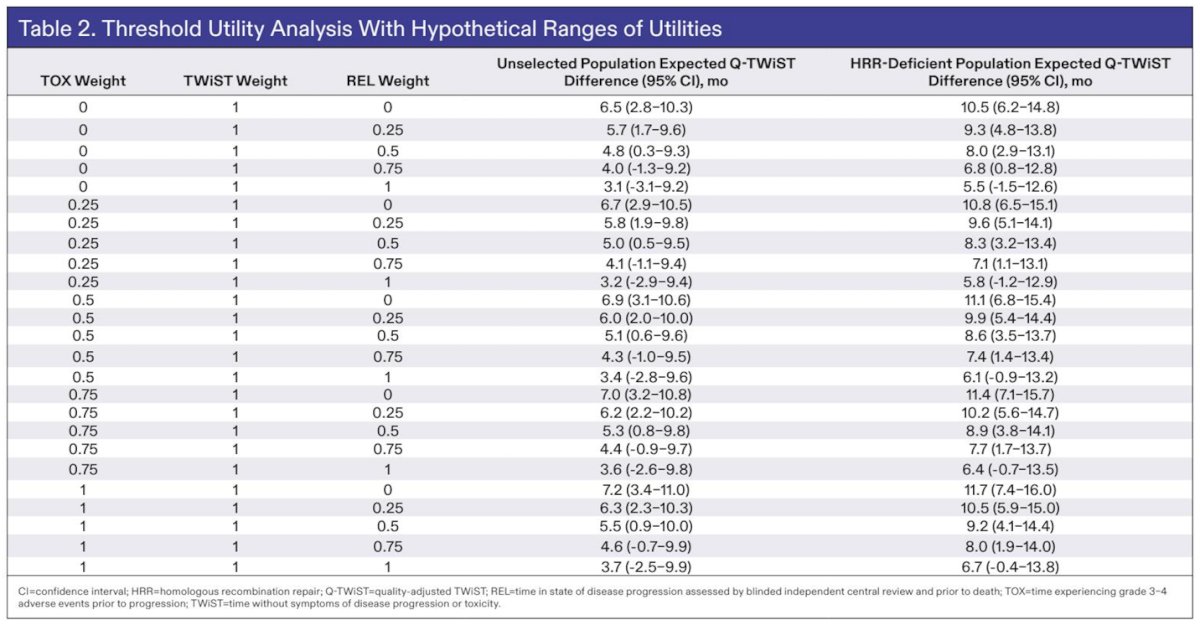
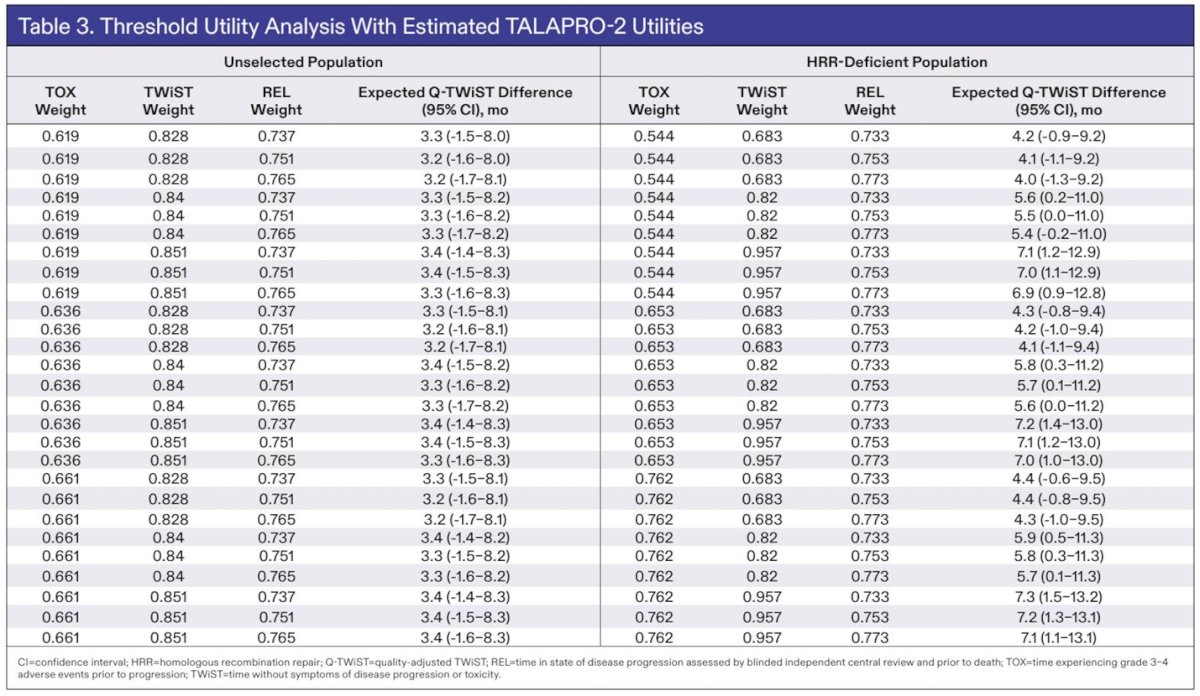
Across the full range of utility assumptions, Q-TWiST remained numerically longer with talazoparib plus enzalutamide compared with placebo plus enzalutamide. The mean between-treatment difference ranged from 3.2 to 3.4 months in the unselected population and from 4.0 to 7.3 months in the HRR-deficient population, supporting a consistent quality-adjusted survival advantage with the combination.
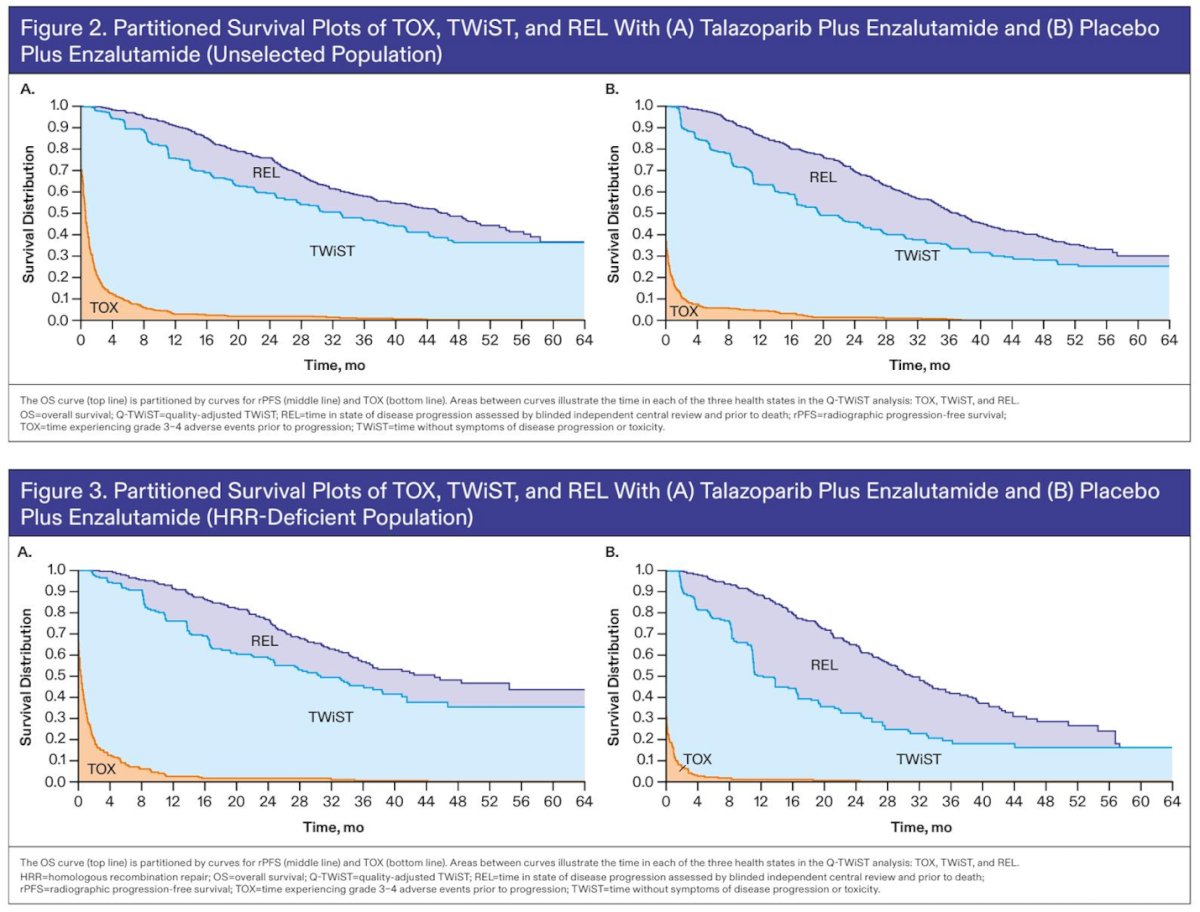
The partitioned survival analyses shown in the figures below illustrate the average time spent in each health state across both the unselected and HRR-deficient populations. In both cohorts, patients treated with talazoparib plus enzalutamide experienced longer time without symptoms of progression or significant toxicity (TWiST), slightly longer time in the TOX state, and shorter time after progression (REL) compared with those receiving placebo plus enzalutamide. These findings reinforce that the combination extended time in the most clinically meaningful health state while reducing time spent in the post-progression period.
Dr. Agarwal emphasized the clinical relevance of integrating survival duration with quality of life. He concluded his presentation with the following key points:
- In this post hoc analysis of TALAPRO-2, talazoparib plus enzalutamide demonstrated longer Q-TWiST compared with placebo plus enzalutamide in both the unselected and HRR-deficient mCRPC populations, indicating a net clinical benefit.
- The Q-TWiST advantage was primarily driven by shorter time in the REL state, despite slightly longer time spent in the TOX state with the combination.
- These analyses were conducted in the two pre-specified TALAPRO-2 populations; future evaluations may further explore Q-TWiST in clinically relevant subgroups.
- The observed Q-TWiST benefit provides additional support for first-line talazoparib plus enzalutamide in patients with unselected and HRR-deficient mCRPC.
Presented by: Neeraj Agarwal, MD, FASCO, Professor, Presidential Endowed Chair of Cancer Research, Director GU Program and the Center of Investigational Therapeutics (CIT), Huntsman Cancer Institute, University of Utah, Salt Lake City, UT
Written by: Julian Chavarriaga, MD – Urologic Oncologist, Department of Urology at Penn State Health. @chavarriagaj on Twitter during the 2026 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA, between February 26th and 28th, 2026.
References: