(UroToday.com) The 2025 European Society for Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, was host to a prostate cancer poster session. Dr. Joan Carles presented the results of an ad hoc analysis from TALAPRO-2 evaluating time to response with talazoparib + enzalutamide in patients with metastatic castration-resistant prostate cancer (mCRPC).
In the randomized, double-blind, phase III TALAPRO-2 trial, men received either talazoparib plus enzalutamide or placebo plus enzalutamide as initial treatment for mCRPC.1,2 Patients were recruited into two cohorts – an unselected cohort and a cohort with homologous recombination repair (HRR) gene alterations (HRR-deficient).1,2
At the primary analysis, treatment with talazoparib plus enzalutamide was shown to significantly improve the primary endpoint of radiographic progression-free survival (rPFS) and secondary efficacy endpoints, including objective response rate (ORR) and prostate-specific antigen (PSA) response (proportion of patients with a PSA response of ≥50%) versus placebo plus enzalutamide in both the unselected and HRR-deficient cohorts.1,2
At the final analysis for overall survival (OS), treatment with talazoparib plus enzalutamide was shown to significantly improve the key secondary endpoint of OS versus placebo plus enzalutamide in both the unselected (HR: 0.80; 95% CI: 0.66–0.96; p=0.016) and HRR-deficient (HR: 0.62; 95% CI: 0.48–0.81, p=0.0005) cohorts. Furthermore, updated results for rPFS and secondary efficacy endpoints were consistent with the primary analyses.3,4
Time to objective response (TTR) and time to PSA response provide supportive information to further analyze the ORR and PSA response and are important decision-making factors for clinicians with patients who may have a high burden of disease or who are symptomatic.
Patients were randomized 1:1 to the talazoparib arm (talazoparib 0.5 mg once daily [QD], or 0.35 mg for those with renal impairment, plus enzalutamide 160 mg QD) or the control arm (placebo QD plus enzalutamide 160 mg QD), stratified by HRR gene alteration status (unselected cohort only) and prior abiraterone (or orteronel) and/or docetaxel treatment versus no such prior treatment for castration-sensitive prostate cancer.1,2
Before randomization, all patients were prospectively assessed for HRR gene alterations in solid tumor tissue, and a protocol amendment allowed concurrent prospective testing of circulating tumor DNA (ctDNA).1,2 The primary endpoint was rPFS by blinded independent central
review (BICR).1,2 Secondary endpoints included:
- OS (alpha-protected)
- ORR by BICR (in patients with measurable soft tissue disease at baseline)
- Duration of soft tissue response
- PSA response (proportion of patients with a PSA response of ≥50%)
Imaging scans were done every 8 weeks until Week 25 and every 12 weeks thereafter.1,2 TTR and time to PSA response were defined as time from randomization to first complete or partial response and first PSA response (≥ß50%), respectively. TTR was assessed in patients with measurable disease at baseline; time to PSA response was measured in all patients randomized
to treatment.1,2 TTR was also assessed in exploratory subgroups by HRR gene alteration status in the unselected cohort as defined below:
- HRR-non-deficient (by both ctDNA and tumor tissue test)
- Undetermined HRR (HRR-deficient by ctDNA or tumor tissue test and unknown by the other, or unknown by both)
- HRR-deficient (by either ctDNA or tumor tissue test)
At data cutoff (September 3, 2024), 119 patients in the talazoparib arm and 130 in the control arm of the unselected cohort were evaluable for a response. The ORR was higher in the talazoparib arm (61%) than in the control arm (44%). The median TTR was similar between the talazoparib (2 months) and control (1.9 months]) arms. In the talazoparib arm, median TTR was ≤2.1 months in all subgroups, except in patients with undetermined HRR status (median, 3.5 months).

The median TTR was fairly consistent for patients regardless of age, geographic region, Eastern Cooperative Oncology Group performance status (ECOG PS), Gleason score, disease stage at diagnosis, progression at entry, or baseline PSA level.
The median duration of response was similar between the talazoparib (20.4 months) and control (19.8 months) arms.

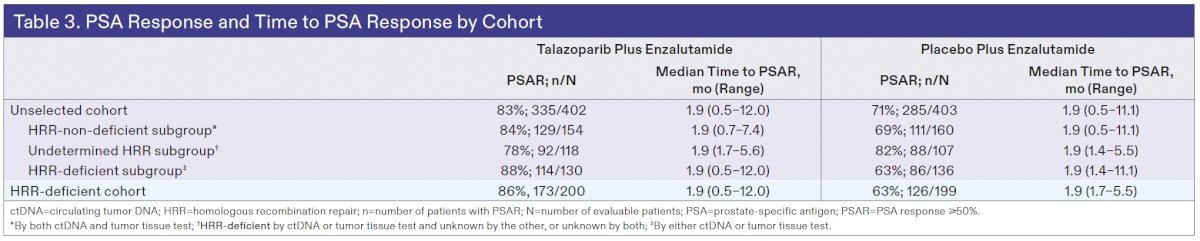
In the overall unselected cohort, the PSA response was higher in the talazoparib arm (83% versus 71%). The median time to PSA response was 1.9 months in both treatment arms and was consistent across HRR status subgroups (1.9 months in all subgroups; Table 3).
In the HRR-deficient cohort, 72 patients in the talazoparib arm and 65 in the control arm were evaluable for a response. The ORR was higher in the talazoparib arm (69% versus 38%). The median TTR was similar between the talazoparib (2.1 months) and control (1.9 months) arms. In the talazoparib arm, the median TTR was fairly consistent for patients regardless of age, geographic region, ECOG PS, Gleason score, disease stage at diagnosis, progression at entry, or baseline PSA level. The median duration of response was longer in the talazoparib arm (22.1 versus 11.4 months.
The PSA response was higher in the talazoparib arm (86% versus 63%). The median time to PSA response was 1.9 months in both treatment arms.
Dr. Carles concluded as follows:
- The median time-to-response was short in patients with mCRPC receiving talazoparib plus enzalutamide (unselected cohort: 2.0 months; HRR-deficient cohort: 2.1 months) and those receiving placebo plus enzalutamide (unselected cohort: 1.9 months; HRR deficient cohort: 1.9 months)
- The median time to PSA response was 1.9 months for patients in both cohorts and consistent regardless of HRR gene alteration status
Presented by: Joan Carles, MD, PhD, Department of Medical Oncology, Vall D'Hebron University Hospital, 08035 Barcelona, Spain
Written by: Rashid K. Sayyid, MD, MSc, Assistant Professor, Urologic Oncologist, Department of Urology at The University of Arizona and Banner University Medical Center – Tucson, AZ, @rksayyid on X during the 2025 European Society for Medical Oncology (ESMO) Annual Congress, Berlin, Germany, October 17–21, 2025
References:
- Agarwal N, Loriot Y, McGregor BA, Fay AP, Gafanov RA, Franke FA, et al. TALAPRO-2: Talazoparib plus enzalutamide in metastatic castration-resistant prostate cancer. Lancet. 2023; 402(10398):291–303.
- Fizazi K, Shore N, Sandhu S, Saad F, Tagawa ST, Chi KN, et al. PEACE-1: Abiraterone plus prednisone and radiotherapy in metastatic hormone-sensitive prostate cancer. Nat Med. 2024; 30(1):257–264.
- Agarwal N, Sonpavde G, Loriot Y, Gafanov RA, Kramer G, Azad A, et al. TALAPRO-3: Talazoparib plus enzalutamide in homologous recombination repair–deficient mCSPC. Lancet. 2025; 406(10502):447–460.
- Fizazi K, Chi KN, Saad F, Zhang J, Mellado B, Attard G, et al. ARASENS-2: Darolutamide plus androgen deprivation therapy and docetaxel in metastatic hormone-sensitive prostate cancer. Lancet. 2025; 406(10502):461–474.