(UroToday.com) The 2025 ASCO annual meeting featured a quality care and health services research session and a presentation by Dr. Nobuaki Matsubara discussing the final patient-reported outcomes in unselected men receiving talazoparib + enzalutamide versus placebo + enzalutamide as initial treatment for metastatic castration-resistant prostate cancer (mCRPC) in the phase 3 TALAPRO-2 study. TALAPRO-2 demonstrated statistically significant improvement with talazoparib + enzalutamide versus placebo + enzalutamide in radiographic progression-free survival (primary endpoint; HR 0.63, 95% CI 0.51–0.78; p < 0.0001) in unselected men with mCRPC.1 Prior patient reported outcome analyses (data cutoff: August 16, 2022) reported no clinically meaningful between-arm differences in any functioning scales and a longer time to definitive deterioration in global health status (GHS)/quality of life for talazoparib + enzalutamide (median 30.8 months) versus placebo + enzalutamide (25.0 months; HR 0.780, 95% CI 0.62–0.99; p = 0.038).2 At the 2025 ASCO annual meeting, Dr. Matsubara and colleagues reported updated (data cutoff: September 3, 2024) final patient reported outcomes for the unselected cohort.
Patient reported outcomes were assessed at day 1 (baseline) and scheduled visits (every 4 weeks until week 53, and then every 8 weeks) until radiographic progression using the EORTC QLQ-C30 and its prostate cancer module, QLQ-PR25, and worst pain by BPI-SF item 3. Prespecified patient reported outcome analyses included overall mean change from baseline (per longitudinal repeated measures mixed-effects model), time to deterioration, and time to definitive deterioration. The clinically meaningful threshold was ≥10 points for EORTC scales and ≥2 points for BPI-SF. Between-arm comparisons of time to deterioration/time to definitive deterioration were made using a stratified log-rank test and a Cox proportional hazards model.
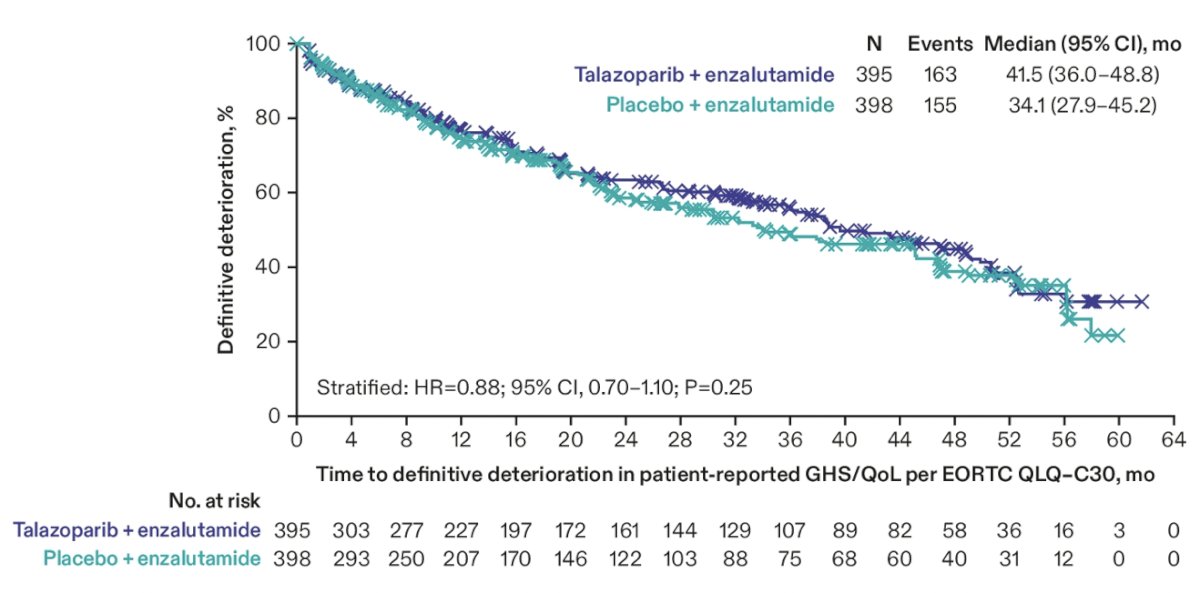
Of the 805 men randomized to treatment, 793 (talazoparib + enzalutamide, n=395; placebo + enzalutamide, n=398) had 1 baseline + ≥1 follow-up patient reported outcome score. Baseline characteristics were balanced between the treatment arms. With extended follow-up (median 52.5 months, 95% CI 50.6-53.4), the median time to definitive deterioration for GHS/quality of life in the talazoparib + enzalutamide arm was 41.5 months versus 34.1 months in the placebo + enzalutamide arm (HR 0.88, 95% CI 0.70–1.10; p = 0.2487):
Median time to definitive deterioration for urinary symptoms in the talazoparib + enzalutamide arm was 59.8 months versus 58.0 months in the placebo + enzalutamide arm (HR 0.86, 95% CI 0.62–1.19; p = 0.3655). There were no clinically meaningful between-arm differences in QLQ-C30 functioning and symptoms scales observed:
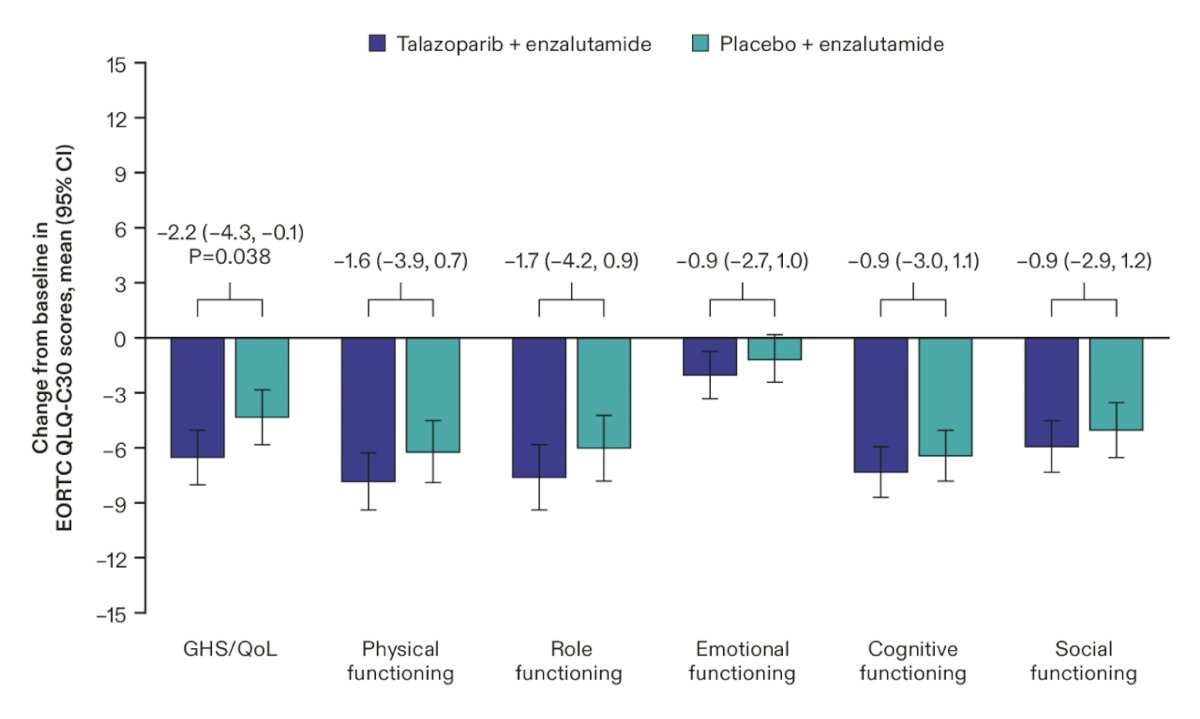
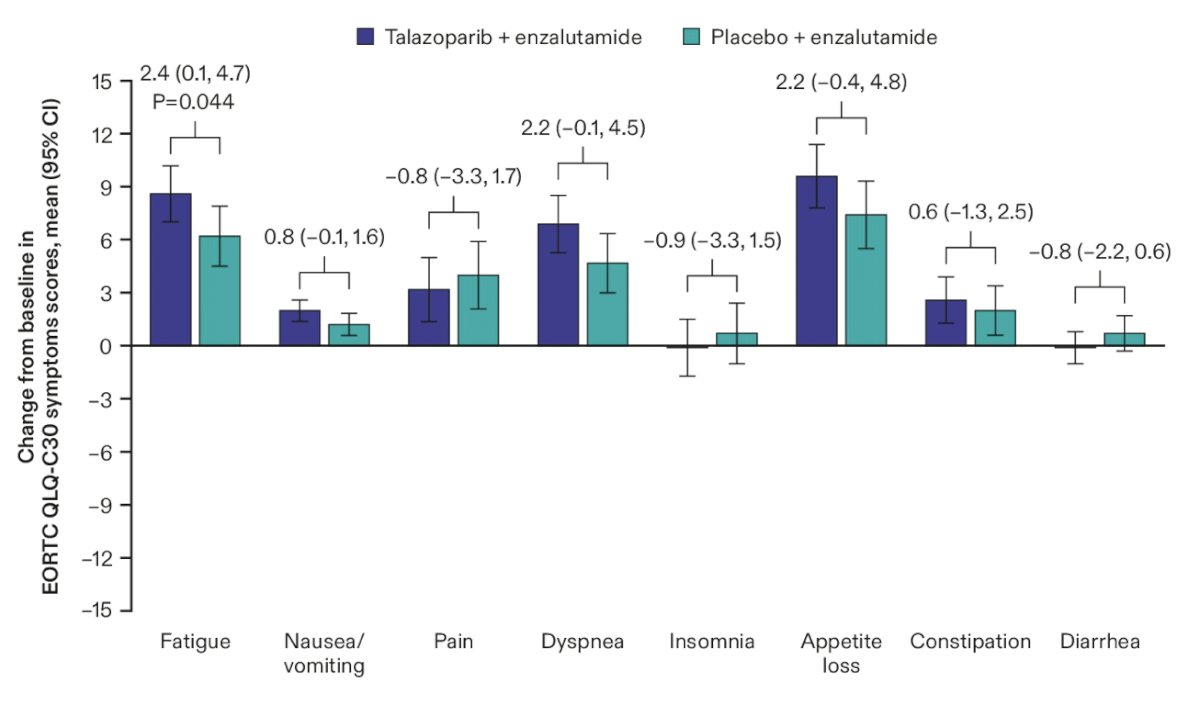
The only between arm differences with a p value < 0.05 were GHS/quality of life, where patients reported slightly more deterioration in the talazoparib + enzalutamide arm (estimated mean difference = -2.2, 95% CI -4.3 to -0.1; p = 0.038) and fatigue, which was slightly worse in the talazoparib + enzalutamide arm (estimated mean difference = -2.4, 95% CI 0.1 to 4.7; p = 0.044). Mean changes from baseline in QLQ-PR25 prostate cancer specific symptoms scales were similar between treatment arms:
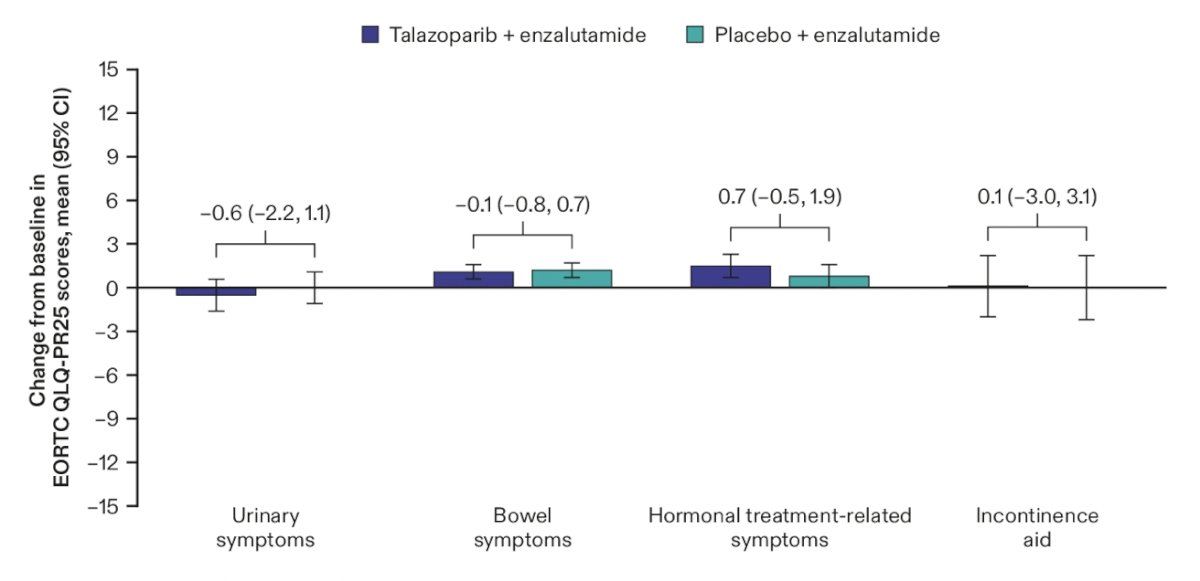
There was no clinically meaningful between arm differences in patient reported worst pain in the last 24 hours (estimated mean difference = -0.1, 95% CI -0.4 to 0.1; p = 0.27) or time to deterioration for worst pain by BPI-SF (HR 0.95, 95% CI 0.68-1.33, p = 0.37) observed. In addition to time to pain analyses, time to opiate use for prostate cancer was similar between the talazoparib + enzalutamide arm and placebo + enzalutamide arm (HR 0.94, 95% CI 0.74-1.19, p = 0.60)
Dr. Matsubara concluded his presentation discussing the final patient reported outcomes in TALAPRO-2 with the following take home points:
- With extended follow-up, quality of life was maintained with talazoparib + enzalutamide
- These data confirm that quality of life is not compromised when talazoparib is added to enzalutamide, for initial treatment of unselected men with mCRPC
Presented by: Nobuaki Matsubara, MD, National Cancer Center Hospital East, Kashiwa, Japan
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.
Related content: Talazoparib-Enzalutamide Combintation and Quality of Life in mCRPC Patients - Nobuaki Matsubara
References:
- Agarwal N, Azad AA, Carles J, et al. Talazoparib plus enzalutamide in men with first-line metastatic castration-resistant prostate cancer (TALAPRO-2): A randomized, placebo-controlled, phase 3 trial. Lancet. 2023 Jul 22;402(10398):291-303.
- Matsubara N, Azad AA, Agarwal N, et al. First-line talazoparib plus enzalutamide versus placebo plus enzalutamide for metastatic castration-resistant prostate cancer: Patient-reported outcomes from the randomized, double-blind, placebo-controlled, phase 3 TALAPRO-2 trial. Lancet Oncol. 2025;26(4):470-480.