(UroToday.com) The 2024 American Society of Clinical Oncology Genitourinary (ASCO GU) cancers symposium held in San Francisco, CA between January 25th and 27th was host to a prostate cancer poster session. Dr. Neal Shore presented the results of a post-hoc analysis of TALAPRO-2 radiographic progression-free survival (rPFS) and overall survival (OS) outcomes, stratified by genomic subgroups defined by the likelihood of BRCA or homologous recombination repair (HRR) gene alteration status.
TALAPRO-2 is a phase III randomized, double-blind, placebo-controlled trial that evaluated the combination of talazoparib and enzalutamide in the first-line treatment setting for mCRPC patients. Patients were randomized 1:1 to talazoparib 0.5 mg once daily (reduced dose from standard of 1.0 mg) plus enzalutamide 160 mg once daily versus placebo + enzalutamide. Notably, this was a biomarker unselected cohort of ‘all comers’. Prior to randomization, all patients were prospectively assessed for HRR gene alterations in tumor tissue and/or circulating tumor DNA (ctDNA) using FoundationOne CDx and/or FoundationOne Liquid CDx. The primary endpoint was rPFS, assessed via blinded independent central review (BICR). The trial design for TALAPRO-2 was as follows: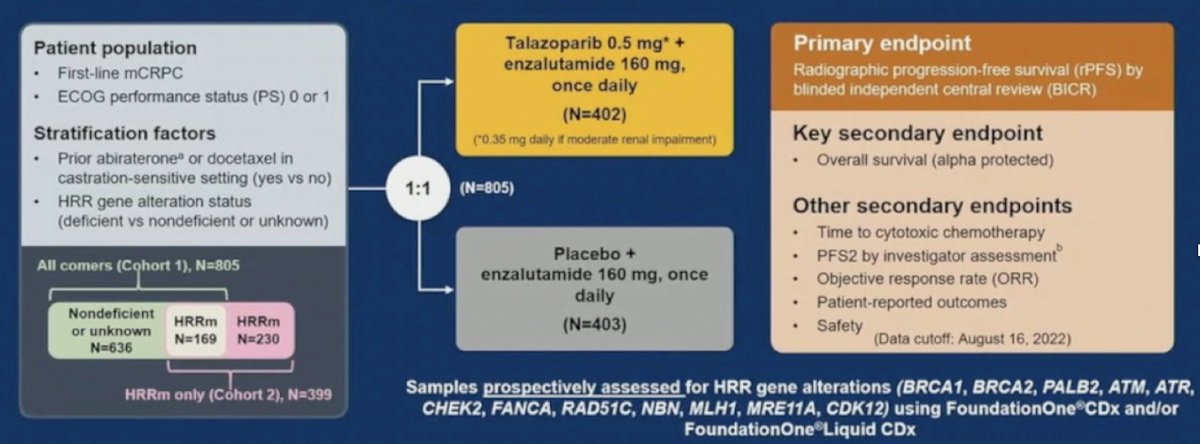
21% of patients in each arm were HRR deficient. The combination of talazoparib + enzalutamide was associated with a 37% improvement in rPFS, compared to placebo + enzalutamide (median: not reached versus 22 months; HR: 0.63, 95% CI: 0.51 – 0.78, p<0.001). OS data remains immature, with a trend towards an OS improvement in the overall cohort (HR: 0.89, 95% CI: 0.69 – 1.14, p=0.35).1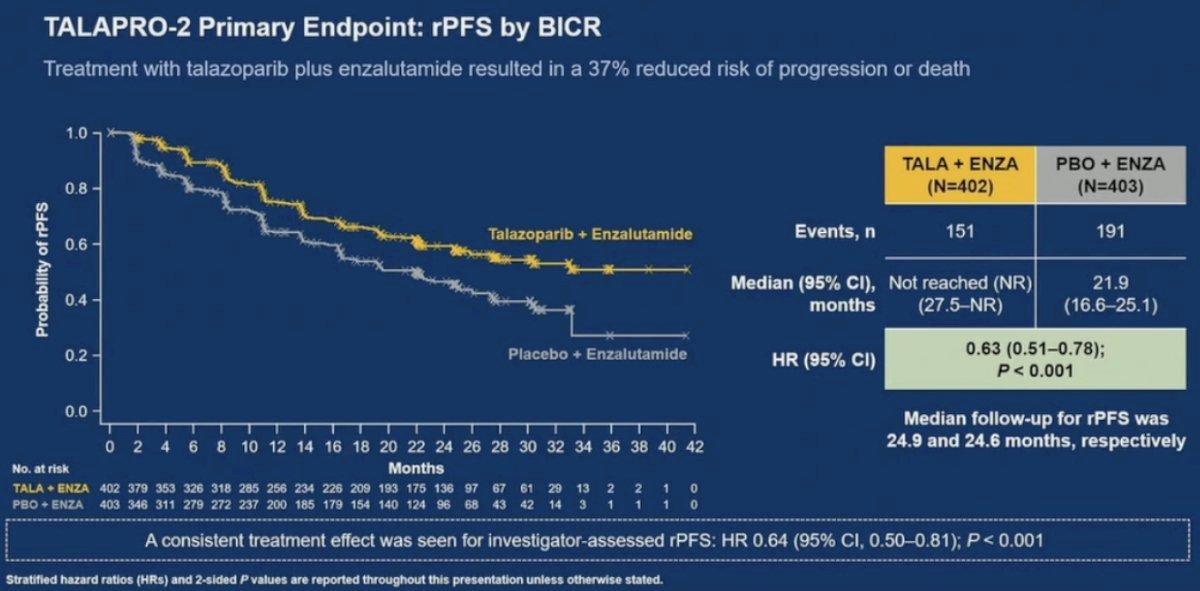
To further investigate if the intention-to-treat (ITT) results for TALAPRO-2 all-comer cohort were driven by unidentified biomarker-positive patients, Dr. Shore and colleagues investigated the correlation between rPFS/OS outcomes and patient BRCA or HRR alteration status.
Within each analysis by BRCA or HRR alteration status, three exploratory subgroups based on the likelihood of BRCA/HRR alterations were defined using all available FoundationOne records, from both prospective and retrospective exploratory testing:
- BRCA1/2 mutated (BRCAm; 10% ITT) or HRR mutated (HRRm; 33% ITT)
- A positive test result in either ctDNA and/or tumor tissue testing.
- Undetermined BRCAm (38% ITT) or undetermined HRRm (28% ITT)
- Patients with one negative BRCAm/HRRm test result not confirmed by the other test, or for whom the results of both tests were indeterminate.
- Non-BRCAm (51% ITT) or non-HRRm (39% ITT)
- Patients with negative BRCAm or HRRm status confirmed by both ctDNA and tumor tissue testing.
As expected, both rPFS and OS benefits were observed for both the BRCAm (HRs: 0.24 and 0.53, respectively) and HRRm subgroups (HRs: 0.51 and 0.68, respectively). Notably, an rPFS benefit was observed in the non-BRCAm and non-HRRm subgroups with the addition of talazoparib to enzalutamide (non-BRCAm: median: 33.1 versus 22.1 months; HR: 0.71, 95% CI: 0.52 – 0.96). A trend towards improved OS was also observed in the non-BRCAm (HR: 0.76, 95% CI: 0.56 – 1.03) and non-HRRm subgroups (HR: 0.88, 95% CI: 0.63 – 1.23).
For both rPFS and OS outcomes in the undetermined BRCAm and HRRm subgroup, the hazard ratio magnitudes of effect were lower than those observed for the BRCAm and HRRm, as expected. However, the corresponding HRs were also of lower magnitude of effect compared to those in the non-BRCAm and non-HRRm subgroups – Dr. Shore explained that intermediate HR values between those observed in patients with and without BRCA and HRR mutations would have been expected given the alteration status uncertainty. The reasons for these findings remain unclear. However, Dr. Shore noted that the OS data in the undetermined HRRm (36%) and undetermined BRCAm (39%) groups were the least mature of all subgroups.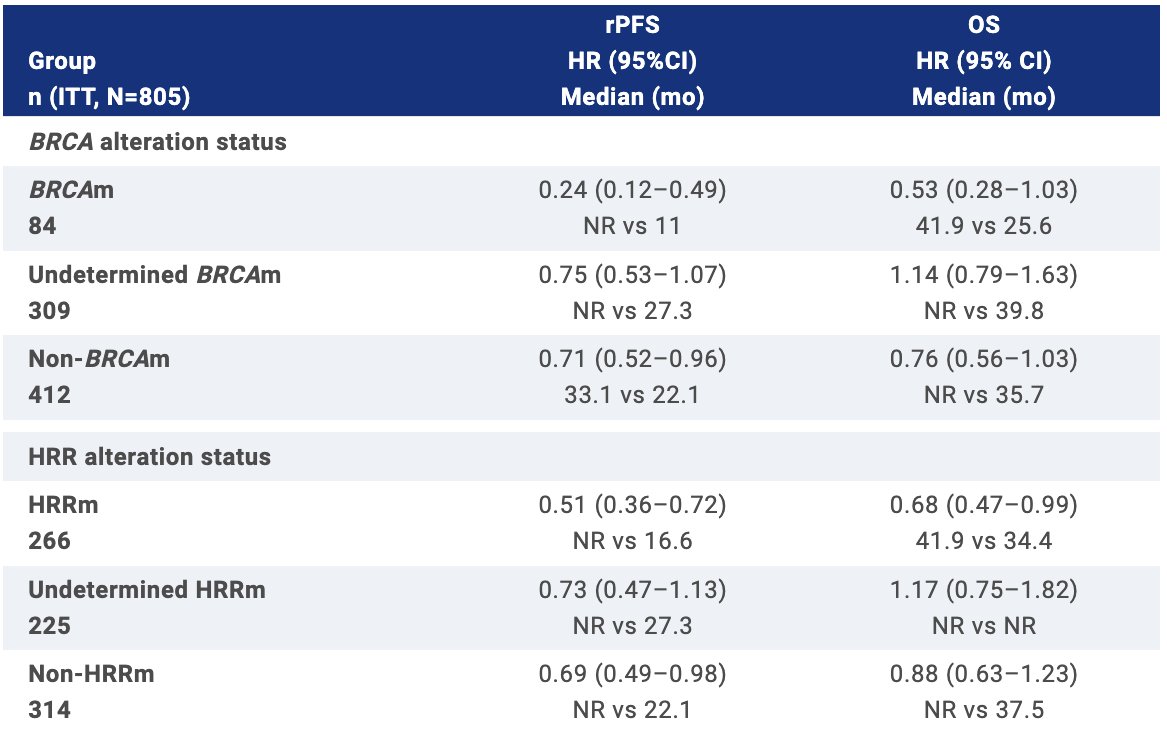
Dr. Shore concluded that the statistically significant rPFS improvement in the TALAPRO-2 all-comer intention-to-treat population did not seem to be attributable to patients with undetected BRCA/HRR alterations. There was evidence of an rPFS benefit in the non-BRCAm and non-HRRm subgroups in favor of talazoparib addition to enzalutamide. While the OS data are still maturing, there is a clear benefit for patients with BRCAm and no detrimental impact for patients negative for BRCAm or HRRm, by both tumor and ctDNA
Presented by: Neal Shore, MD, FACS, Urologist, Director, CPI, Carolina Urologic Research Center, Atlantic Urology Clinics, Myrtle Beach, SC
Written by: Rashid Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2024 American Society of Clinical Oncology Genitourinary (ASCO GU) Cancers Symposium, San Francisco, CA, January 25th – January 27th, 2024
References: