(UroToday.com) The 2025 Western Section AUA annual meeting featured a urothelial carcinoma session and a presentation by Siamak Daneshmand, MD, discussing updates to the CORE-008 trial protocol, a phase 2 multi-arm, multi-cohort study to evaluate intravesical cretostimogene grenadenorepvec in patients with high-risk non-muscle invasive bladder cancer. Treatment for high-risk non-muscle invasive bladder cancer includes TURBT followed by intravesical BCG, yet high recurrence rates and the ongoing BCG shortage highlight the need for effective, well-tolerated, and readily available treatment options.
Cretostimogene is an oncolytic immunotherapy with a dual mechanism of action. It selectively replicates in and lyses cancer cells with Retinoblastoma-E2F pathway alterations, releasing virus- and tumor-specific antigens that initiate antitumor immune activation, further enhanced by the GM-CSF transgene. The BOND-003 trial (cretostimogene in BCG unresponsive non-muscle invasive bladder cancer with CIS) demonstrated a 75% complete response and median duration of response of 27.9 months, with 0% Grade 3+ treatment-related adverse events. These results led to cretostimogene receiving Fast Track and Breakthrough Therapy Designations by the US FDA for BCG-unresponsive non-muscle invasive bladder cancer. The CORE-008 clinical trial (NCT06567743) was developed as a phase 2, multi-arm, multi-cohort trial to evaluate the efficacy and safety of cretostimogene in patients with high-risk non-muscle invasive bladder cancer.
Eligibility criteria for CORE-008 comprises pathologic confirmation of high-risk non-muscle invasive bladder cancer (per the AUA/SUO guideline), CIS-containing and papillary only. The study includes Cohort A (BCG-naive: no prior BCG, BCG >24 months ago, or 1-2 doses in past 24 months), Cohort B (BCG-exposed: recurrence after prior BCG), both receiving cretostimogene monotherapy, as well as Cohort CX (BCG-exposed and BCG-unresponsive), which will evaluate the safety and high-grade event-free survival of cretostimogene in combination with intravesical gemcitabine:
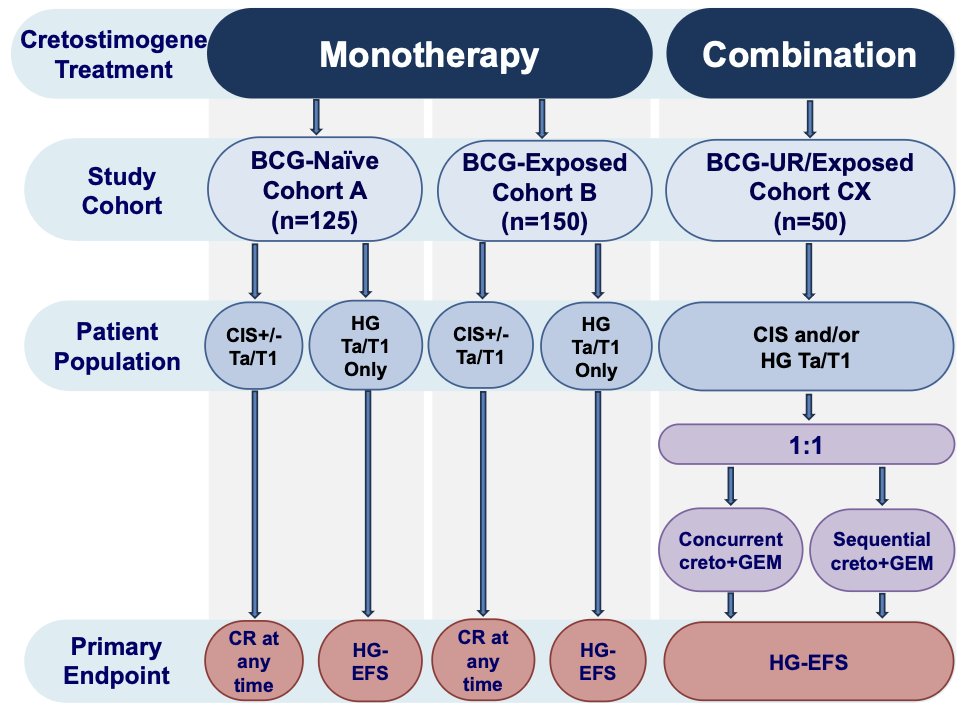
For Cohorts A and B, intravesical cretostimogene will be instilled in combination with DDM, an excipient that enhances adenoviral delivery, for six weekly doses during the induction phase, followed by three weekly maintenance cycles quarterly through month 12, then every six months through month 36. Re-induction is permitted across all cohorts:

The primary endpoint for the CIS population is complete response at any time and high-grade event-free survival for patients with papillary-only disease. Secondary endpoints will include duration of response, all-cause event-free survival, bladder cancer-specific survival, cystectomy-free survival, safety, and tolerability. Exploratory outcome measures include health-related quality of life, overall survival, and biomarker assessments.
CORE-008 is actively recruiting patients. Enrollment for the CIS containing arms on Cohort A has been successfully completed, with an HG Ta/T1-only arm planned. Cohort B has received collaborative support from the Society of Urologic Oncology Clinical Trials Consortium (SUO-CTC). Additionally, Cohort CX has completed enrollment.
Presented by: Siamak Daneshmand, MD, Professor of Urology and Medicine (Clinical Scholar), Director of Urologic Oncology and Clinical Research, Keck School of Medicine, University of Southern California, USC Norris Comprehensive Cancer Center, Los Angeles, CA
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Western Section American Urological Association (AUA) Annual Meeting, Napa Valley, CA, Sun, Nov 2 – Thurs, Nov 6, 2025.