(UroToday.com) The 2025 ASCO annual meeting featured a urothelial carcinoma trials in progress session and a presentation by Gary D. Steinberg, MD, discussing updates to CORE-008, a phase 2 multi-arm, multi-cohort study to evaluate intravesical cretostimogene grenadenorepvec in patients with high-risk non-muscle invasive bladder cancer.
Treatment for high-risk non-muscle invasive bladder cancer includes TURBT followed by intravesical BCG. Despite high initial response rates, over 50% of patients will recur and 20-40% are at risk for progression. Treatment of high-risk non-muscle invasive bladder cancer is challenged by the ongoing BCG shortage, thus there exists a need for clinically effective, well-tolerated, and readily available treatment options.
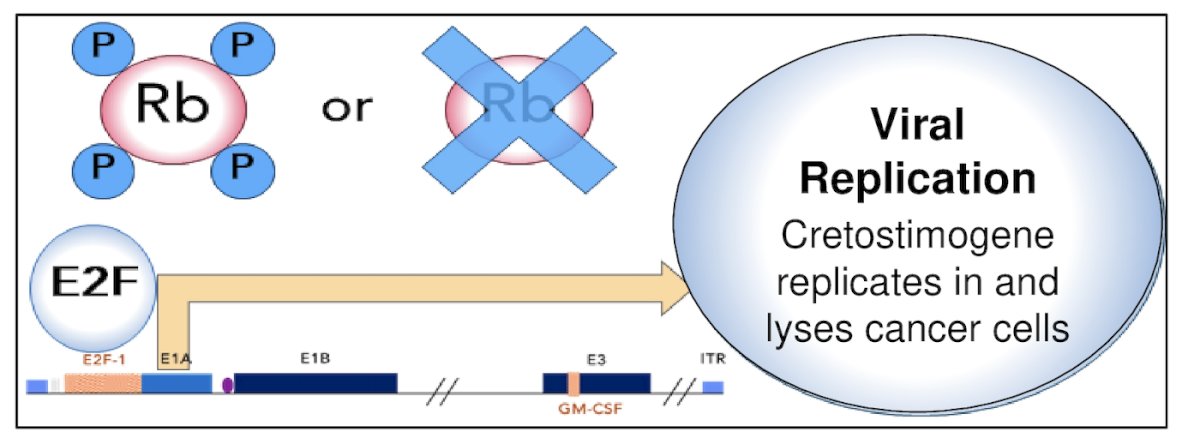
Cretostimogene grenadenorepvec is an oncolytic immunotherapy with a dual mechanism of action. It selectively replicates in and lyses bladder cancer cells with Rb-E2F pathway alterations. The subsequent release of virus- and tumor-specific antigens initiate antitumor immune activation which is further amplified by the GM-CSF transgene:
Cretostimogene received fast track and breakthrough therapy designations by the US FDA for high-risk BCG-unresponsive non-muscle invasive bladder cancer with CIS indication. Given the strength of these data, the CORE-008 clinical trial was developed as a phase 2, multi-arm, multi-cohort trial to further evaluate the efficacy and safety of cretostimogene in patients with high-risk non-muscle invasive bladder cancer.
Eligibility criteria for CORE-008 included pathologic confirmation of high-risk non-muscle invasive bladder cancer, both CIS containing and papillary only, as defined by the AUA guidelines. Cohort A (BCG-naive) includes patients who have not received prior BCG, and cohort B (BCG-exposed) consists of patients who have received prior BCG and recurred at the initial clinical evaluation or at a delayed time point.
Cohort CX, recently added, will evaluate safety and high-grade event free survival of cretostimogene in combination with intravesical gemcitabine, either concurrent (Arm 1) or sequential (Arm 2) in BCG-exposed and BCG-unresponsive patients. The combination is believed to leverage complementary mechanisms and potential immune modulating synergy to enhance outcomes:
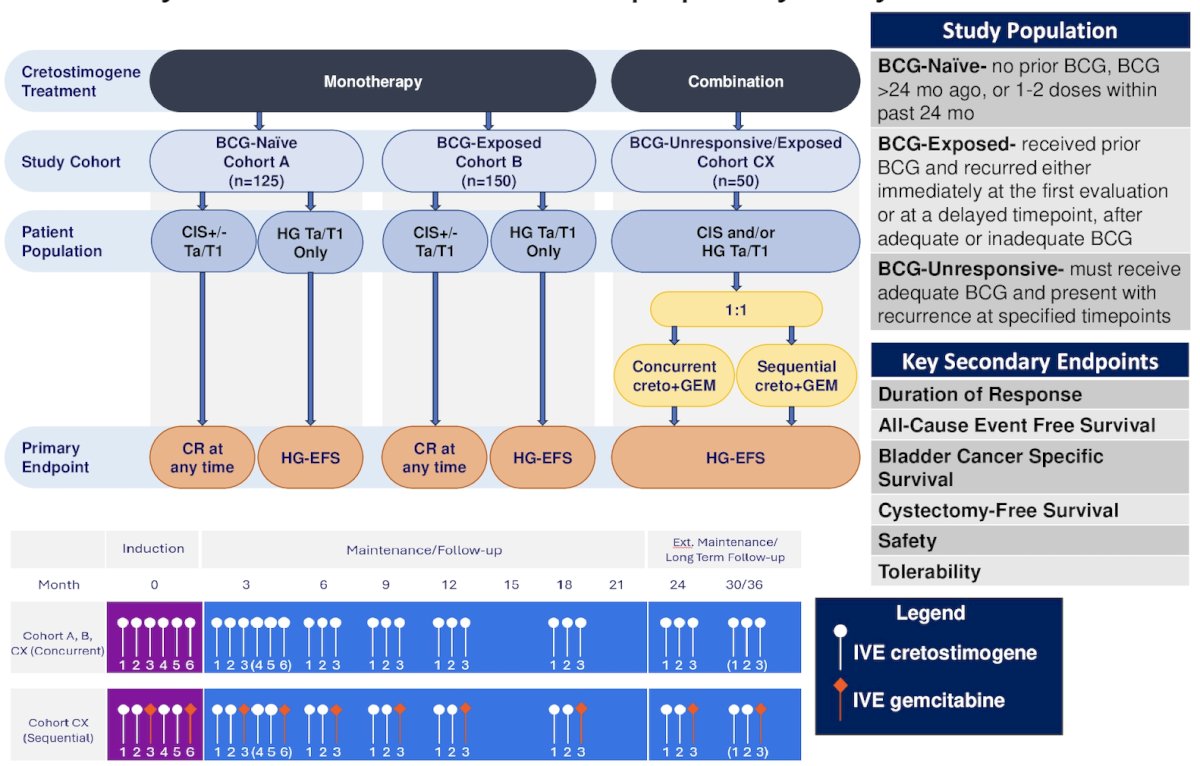
Intravesical cretostimogene will be instilled with n-dodecyl-β-D-maltoside (DDM), an excipient that enhances adenoviral delivery, for six weekly doses during the induction phase, followed by three weekly maintenance cycles quarterly through month 12, then every six months through month 36. Re-induction is permitted.
The primary endpoint for CIS is complete response at any time and high-grade event free survival for papillary-only disease. Secondary endpoints will include duration of response, all-cause event free survival, bladder cancer specific survival, cystectomy-free survival, safety, and tolerability. Exploratory outcome measures include health-related quality of life, overall survival, and biomarker assessments.
CORE-008 is open to recruitment across 49 sites, with the first patient enrolled in October 2024. Cohort A (BCG-naïve) – the CIS-containing arm is complete, and the HG Ta/T1 only arm is planned for the second half of 2025. Cohort B has received collaborative support from the Society of Urologic Oncology-Clinical Trials Consortium (SUO-CTC). Cohort CX (BCG-exposed and BCG unresponsive) is open for enrolment with the first patients having been randomized.
Presented by: Gary D. Steinberg, MD, Professor, Department of Urology, Rush University, Chicago, IL
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the American Society of Clinical Oncology (ASCO) 2025 Annual Meeting, Chicago, IL, Fri, May 30 – Tues, Jun 3, 2025.