(UroToday.com) The 2025 EAU annual meeting featured a non muscle invasive bladder cancer session and a presentation by Dr. Sharada Mokkapati discussing translational correlates using urinary genomic disease burden to assess cretostimogene grenadenorepvec in the BOND-003 and CORE-001 trials. Urinary genomic disease burden profiling uses next-generation sequencing to identify mutations and DNA alterations associated with bladder cancer. It has shown in prior series to be associated with bladder cancer recurrences and responses to therapy. Cretostimogene grenadenorepvec is an oncolytic immunotherapy with a dual mechanism of action. It selectively replicates in and lyses bladder cancer cells with Retinoblastoma-E2F pathway alterations. The subsequent release of virus- and tumor-specific antigens initiates anti-tumor immune activation which is further amplified by the GM-CSF transgene, a potent cytokine:

Cretostimogene has been studied as monotherapy in BOND-003 (75.4% complete response rate) and as combination therapy in CORE-001 (82.9% complete response rate) in patients with BCG-unresponsive non-muscle invasive bladder cancer. In this translational analysis presented at EAU 2025, Dr. Mokkapati and colleagues evaluated the associations between urinary genomic disease burden and cretostimogene.
All patients who received at least one dose of cretostimogene and had urinary genomic disease burden testing were included. Urine samples were collected at baseline and sentinel time points after treatment. Urinary genomic disease burden testing was performed with the UroAmp minimal residual disease assay (Convergent Genomics), which employs deep NGS-whole genome sequencing of a 60-gene bladder cancer specific panel and low pass genomic sequencing to identify aneuploidy. UroAmp quantifies minimal residual disease by the genomic disease burden, which is a percentile ranking of the variant allele frequency from a sample relative to its percentile ranking within the established training set. Risk scores for recurrence were calculated using a machine learning algorithm and categorized as minimal residual disease-positive or negative. Molecular response was based on change in urinary genomic disease burden during treatment, and correlations between urinary genomic disease burden and clinical response were assessed.
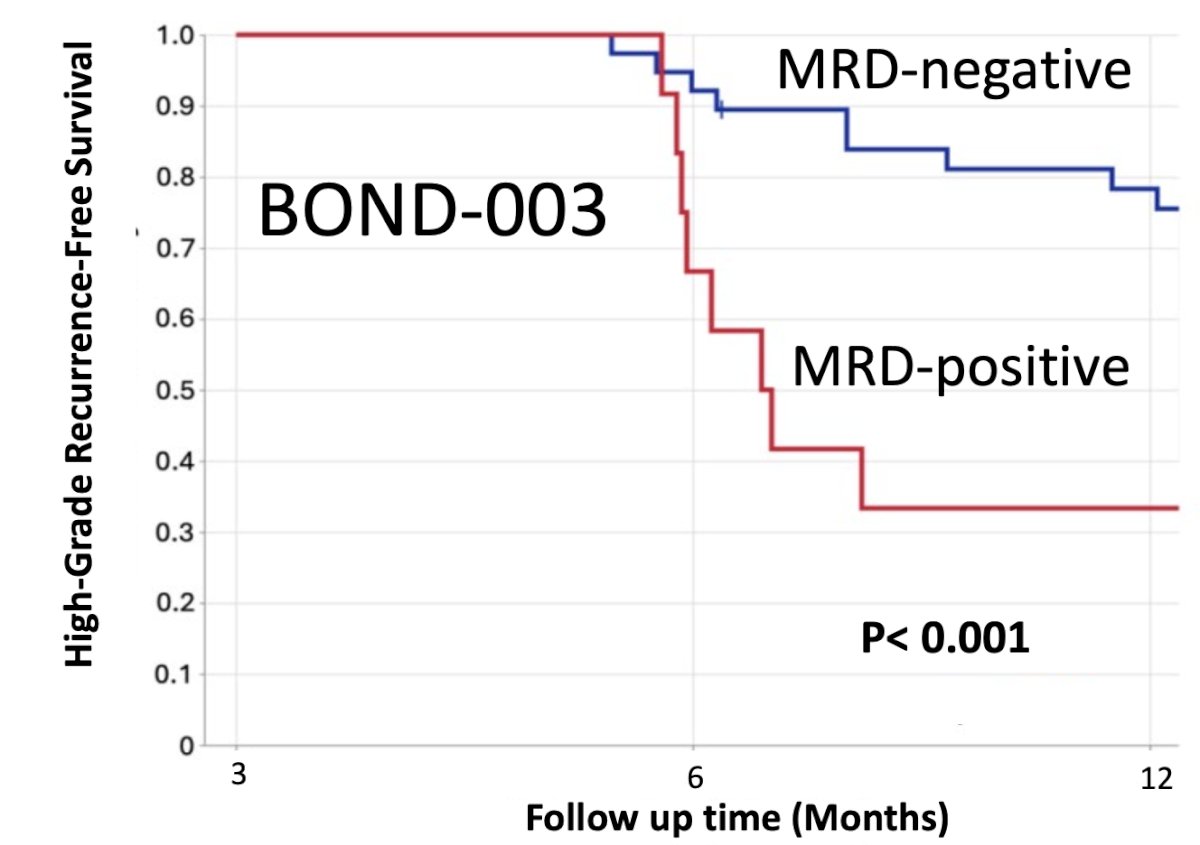
Pre-treatment mutations in TP53, TERT, chromatin-modifying enzymes, proliferation pathways, and aneuploidy were most prevalent across BOND-003 and CORE-001. Overall, 86% of samples in both studies were classified as a higher risk, minimal residual disease positive population at baseline. When aggregated across both studies, minimal residual disease status was highly correlated with clinical response over time. The following figure from BOND-003 shows the impact of minimal residual disease status on high grade recurrence free survival (p < 0.001):
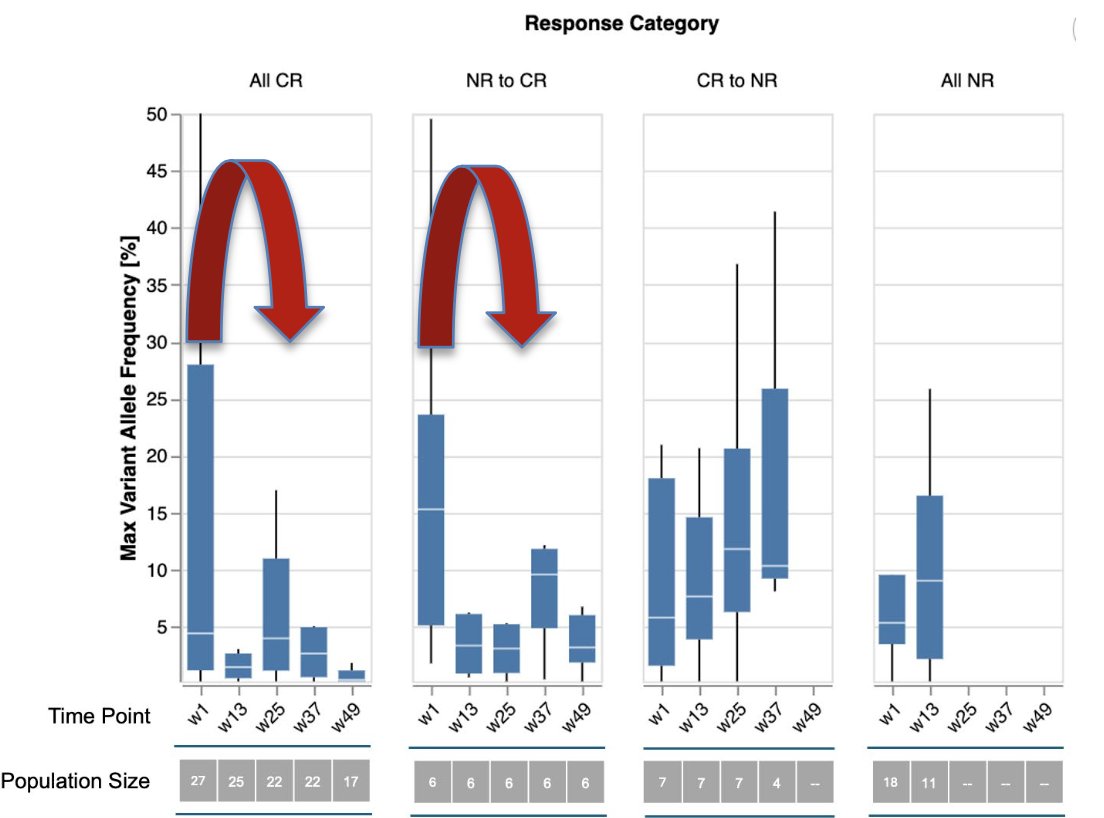
Both studies showed a statistically significant reduction in urinary genomic disease burden in patients achieving complete responses at the 3- and 6 month time points:

Follow-up assessments indicate a consistent pattern of response, suggestive of durable treatment effect. The notable reduction in urinary genomic disease burden in the patients who were salvaged by re-induction reinforces the value of this treatment strategy:
Dr. Mokkapati concluded her presentation by discussing translational correlates using urinary genomic disease burden to assess cretostimogene grenadenorepvec in the BOND-003 and CORE-001 trials with the following take home points:
- Cretostimogene monotherapy and in combination show promising activity in BCG unresponsive non muscle invasive bladder cancer
- Urine tumor DNA profiling with the UroAmp platform enables quantitative assessment of the clinical and molecular response to cretostimogene
- UroAmp stratified patients treated with cretostimogene as minimal residual disease positive or negative and was associated with durable 12 month recurrence free survival
- The notable reduction in variant allele frequency in the 54% of patients who were salvaged by re-induction reinforces the value of re-induction
- Longitudinal minimal residual disease assessment may be able to support the stratification of treatment escalation or de-escalation in future clinical trials
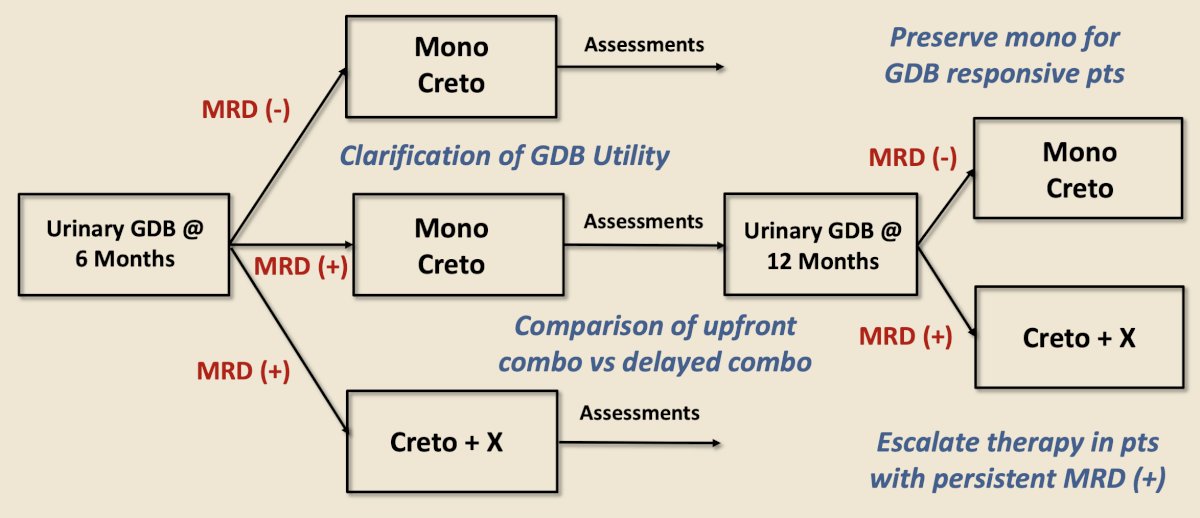
The following figure demonstrates a biomarker driven study design assessing urinary genomic disease burden at 6 months, triaging patients to the cretostimogene treatment regimen received, followed by urinary genomic disease burden at 12 months, and then reassessment of subsequent cretostimogene therapy:
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 European Association of Urology (EAU) Annual Meeting held in Madrid, Spain between March 21st and 24th 2025