(UroToday.com) The 2025 Western Section AUA annual meeting featured a urothelial carcinoma session and a presentation by Dr. Mark Tyson discussing the first results from BOND-003 Cohort P, a multi-national, single-arm study of intravesical cretostimogene grenadenorepvec for treatment of high-risk, papillary-only, BCG-unresponsive non-muscle invasive bladder cancer. Patients with high-risk BCG-unresponsive non-muscle invasive bladder cancer have limited treatment options.
The US FDA has approved treatments for BCG-unresponsive patients with CIS, but additional bladder-sparing treatments are needed, especially for the BCG-unresponsive papillary-only population (with a complete response of 25% at 12 months). Cretostimogene grenadenorepvec, an oncolytic immunotherapy, selectively replicates in and lyses cancer cells with Retinoblastoma-E2F pathway alterations. This releases tumor-specific antigens, initiating antitumor immune activation, further amplified by the GM-CSF transgene. Cretostimogene received US FDA Fast Track and Breakthrough Therapy Designations for high-risk BCG-unresponsive non-muscle invasive bladder cancer with CIS. The BOND-003 Cohort P study (NCT04452591) is a multi-national, single-arm clinical trial assessing the efficacy and safety of intravesical cretostimogene in high-risk, papillary-only, BCG-unresponsive non-muscle invasive bladder cancer patients.
Eligibility criteria for Cohort P include age ≥18 years, ECOG performance status of 0-2, and histologically confirmed BCG-unresponsive HG Ta/T1 papillary disease without CIS within 90 days of study enrollment. BCG unresponsive disease is defined as recurrent high-grade Ta/T1 within 6 months of the last adequate BCG dose per FDA guidance. High-grade T1 after a single BCG induction course are also eligible. Patients must have no evidence of residual bladder cancer before treatment. Intravesical cretostimogene will be instilled for six weekly doses during the induction phase, followed by three weekly maintenance cycles quarterly through month 12, then every six months through month 36. Re-induction is permitted after the first disease assessment for patients with persistent HG Ta and/or CIS. Primary disease assessments include cystoscopy (biopsy as indicated), urine cytology, axial imaging, and mandatory biopsy at month 12, with centralized review of pathologic samples: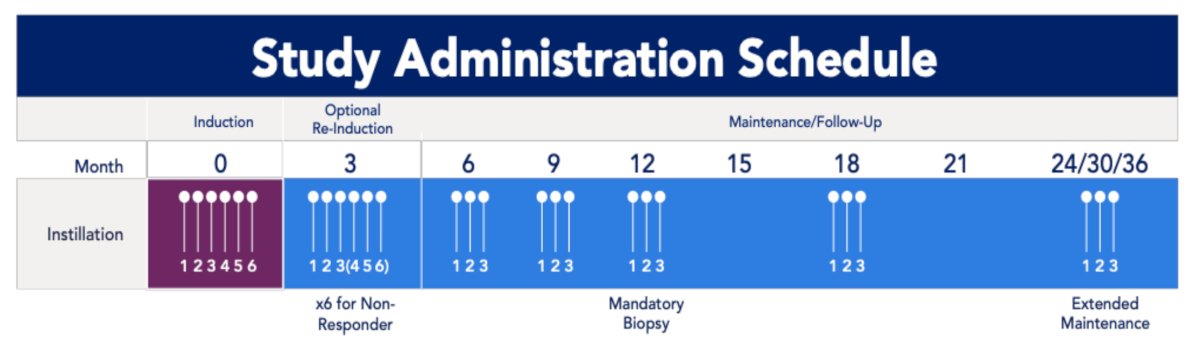
The primary endpoint is high-grade event-free survival, and secondary endpoints include recurrence-free survival, progression-free survival, safety, and time to next intervention. There are 35+ clinical sites that have been selected in the United States and Japan.
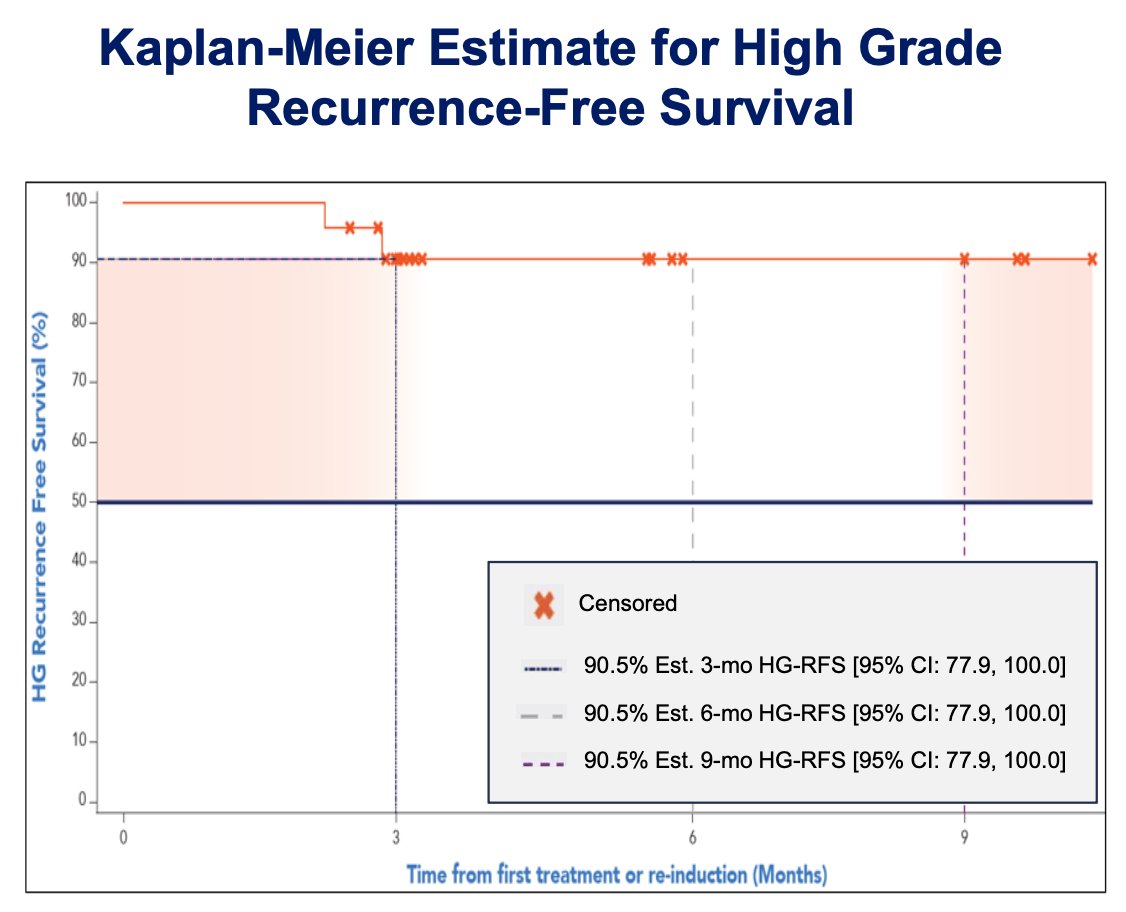
The first 24 patients who received treatment with cretostimogene and were evaluated for high-grade recurrence-free survival and safety were evaluated. Kaplan-Meier estimates at 3- and 9-month high-grade recurrence-free survival are 90.5%, respectively, with a 95% CI of 77.9-100%:
Cretostimogene demonstrated a favorable safety profile, with no serious treatment-related adverse events and no discontinuations related to therapy on Cohort P.
Dr. Tyson concluded his presentation discussing the first results from BOND-003 Cohort P with the following take-home points:
- The first results from BOND-003 Cohort P of cretostimogene monotherapy in patients with BCG unresponsive papillary-only disease demonstrated encouraging high-grade recurrence-free survival rates and a consistent, well-tolerated safety profile
- BOND-003 Cohort P has completed enrollment
- Forthcoming mature data are anticipated to build on these findings and inform future treatment approaches
Presented by: Mark Tyson II, MD, MPH, Urologic Oncologist, Mayo Clinic, Scottsdale, AZ
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Associate Professor of Urology, Georgia Cancer Center, Wellstar MCG Health, @zklaassen_md on Twitter during the 2025 Western Section American Urological Association (AUA) Annual Meeting, Napa Valley, CA, Sun, Nov 2 – Thurs, Nov 6, 2025.