(UroToday.com) The American Urological Association (AUA) 2025 Annual Meeting held in Las Vegas, NV, between April 26th and 29th, 2025, was host to a non-invasive bladder cancer interactive poster session. Dr. Agustin Perez-Londono presented the results of a study evaluating the performance of the EORTC and CUETO risk prediction models in a contemporary cohort of patients undergoing blue light-guided trans urethral resection of bladder tumor (TURBT)
The EORTC and CUETO risk prediction models are two widely used tools for predicting rates of disease recurrence and progression for NMIBC patients.1,2 The performance of these models in patients undergoing TURBT with blue light cystoscopy (BLC-TURBT) has not been examined. This is particularly relevant given the reduced rates of recurrence observed with BLC-TURBT.3 In this study, Dr. Perez-Londono evaluated the performance of the EORTC and CUETO models in a contemporary cohort of patients undergoing BLC-TURBT.
The study investigators identified adult patients from the multi-institutional Blue Light Cystoscopy with Cysview Registry who underwent BLC-TURBT between 2014 and 2023. Patients with papillary disease (+/- CIS) were included, and those with pure CIS were excluded. They calculated disease recurrence-free and progression-free survivals using the EORTC and CUETO models and estimated observed recurrence-free (RFS) and progression-free (PFS) survivals using Kaplan Meier curves.
The baseline characteristics are summarized below. The median follow-up was 18–24 months.

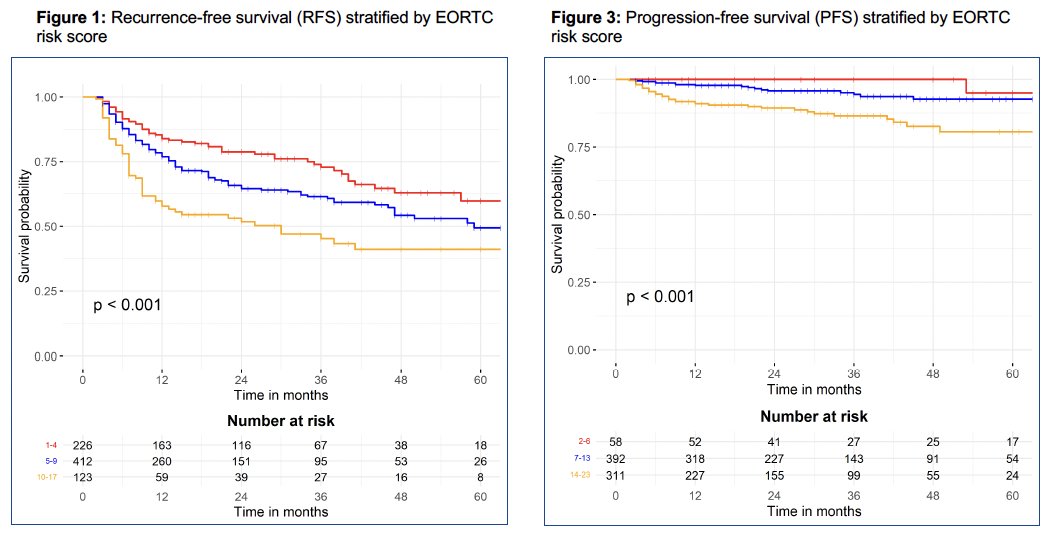
How well did these models discriminate between calculated risk groups? With the EORTC risk model, there were significant differences observed for predicted RFS and PFS between the risk groups.
Notably for the CUETO risk model, there were no significant differences in predicted RFS between the risk groups.
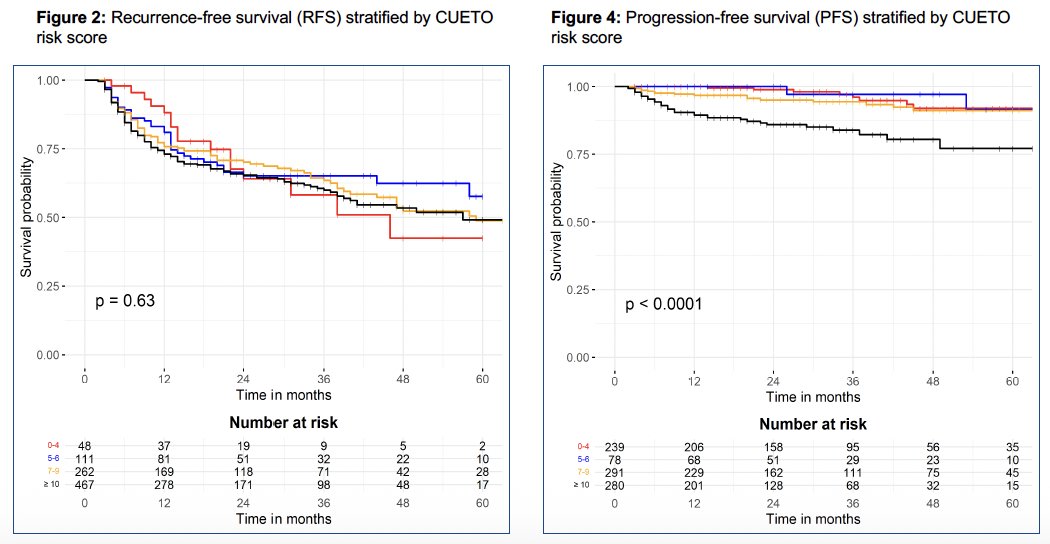
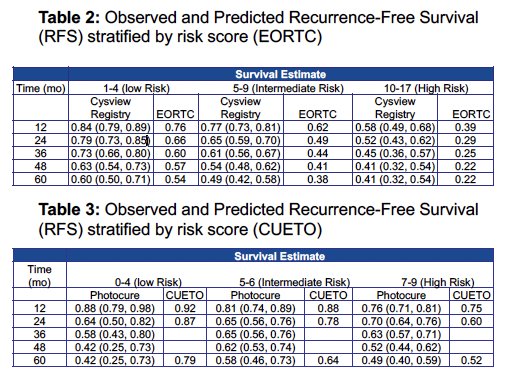
The observed RFS and PFS estimates were generally higher than those predicted by the EORTC risk scores. The CUETO model demonstrated inconsistent results.
Dr. Perez-Londono concluded as follows:
- In a contemporary cohort of patients undergoing BLC-TURBT, the EORTC and CUETO models demonstrated poor performance for predicting RFS and PFS
- The EORTC model generally under-estimated RFS and PFS, particularly for higher risk patients, while the CUETO model demonstrated inconsistent results
- These results underscore the need for the development of more accurate predictive models to guide the risk-adapted management of NMIBC in patients undergoing BLC-TURBT
Presented by: Agustin Perez-Londono, MD, Post-doctoral Research Fellow, Beth Israel Deaconess Medical Center, Boston, MA
Written by: Rashid K. Sayyid, MD, MSc – Robotic Urologic Oncology Fellow at The University of Southern California, @rksayyid on Twitter during the 2025 American Urological Association (AUA) annual meeting held in Las Vegas, NV, Saturday, April 26 - Tuesday, April 29, 2025
References:
- Sylvester RJ, van der Meijden APM, Oosterlinck W, et al. Predicting recurrence and progression in individual patients with stage Ta T1 bladder cancer using EORTC risk tables: a combined analysis of 2596 patients from seven EORTC trials. Eur Urol. 2006; 49(3): 466-465; discussion 475-477.
- Fernandez-Gomez J, Madero R, Solsona E, et al. Predicting Nonmuscle Invasive Bladder Cancer Recurrence and Progression in Patients Treated With Bacillus Calmette-Guerin: The CUETO Scoring Model. J Urol. 2009; 182(5): 2195-2203.
- Daneshmand S, Bazargani ST, Bivalacqua TJ, et al. Blue light cystoscopy for the diagnosis of bladder cancer: Results from the US prospective multicenter registry. Urol Oncol. 2018; 36(8): 361.e1–361.e6.