In effect, the biology of IMDC favorable risk patients is often led by angiogenesis, making TKI monotherapy a viable comparator. The phase III trials concerning mRCC showed less significant advantage in terms of survival of ICI combinations compared to sunitinib in this group of patients.
To answer this question, we performed a reconstructed individual patient's data meta-analysis of 1088 favorable-risk patients from the pivotal phase III clinical trials: JAVELIN Renal 101, KEYNOTE-426, CheckMate 214, CheckMate 9ER, and CLEAR.
To obtain individual patients' data, we reconstructed them from the Kaplan-Meier curves. We used the IPDfromKM workflow (URL: https://biostatistics.mdanderson.org/shiyapps/IPDfromKM/). This workflow enables us to obtain individual patients' raw data from the published Kaplan Meier curves.1
Once obtained raw data we were able to compare indirectly the different experimental arm (assuming that the enrolled population was similar in every clinical trial: mRCC with IMDC favorable-risk score); to enhance the strength of our results, we compared the sunitinib arms among each trial to confirm that there weren’t statistically significant differences in terms of outcomes in standard of care arm among all the included clinical trials. Then we compared every ICI-based combination to a sunitinib curve of merged IPD from the five clinical trials. Fig 1.
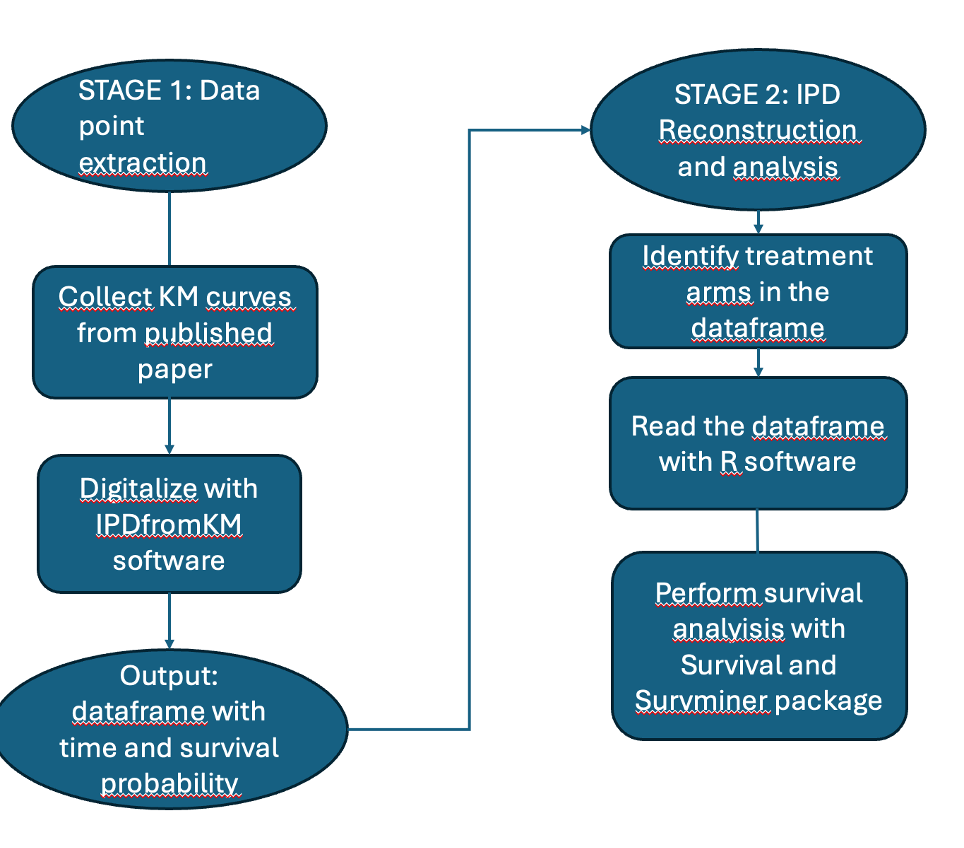
Figure 1. Flow diagram of methods used to obtain individual patients' data (IPD) from the clinical trials.
The aim of the meta-analysis was to determine if the combinations improved outcomes compared to sunitinib and which combination performed better.
The key finding of the analysis in terms of progression-free survival is that Pembrolizumab -Lenvatinib regimen emerged as the better combination with a statistically significant advantage over sunitinib (HR 0.53). (Figure 2)
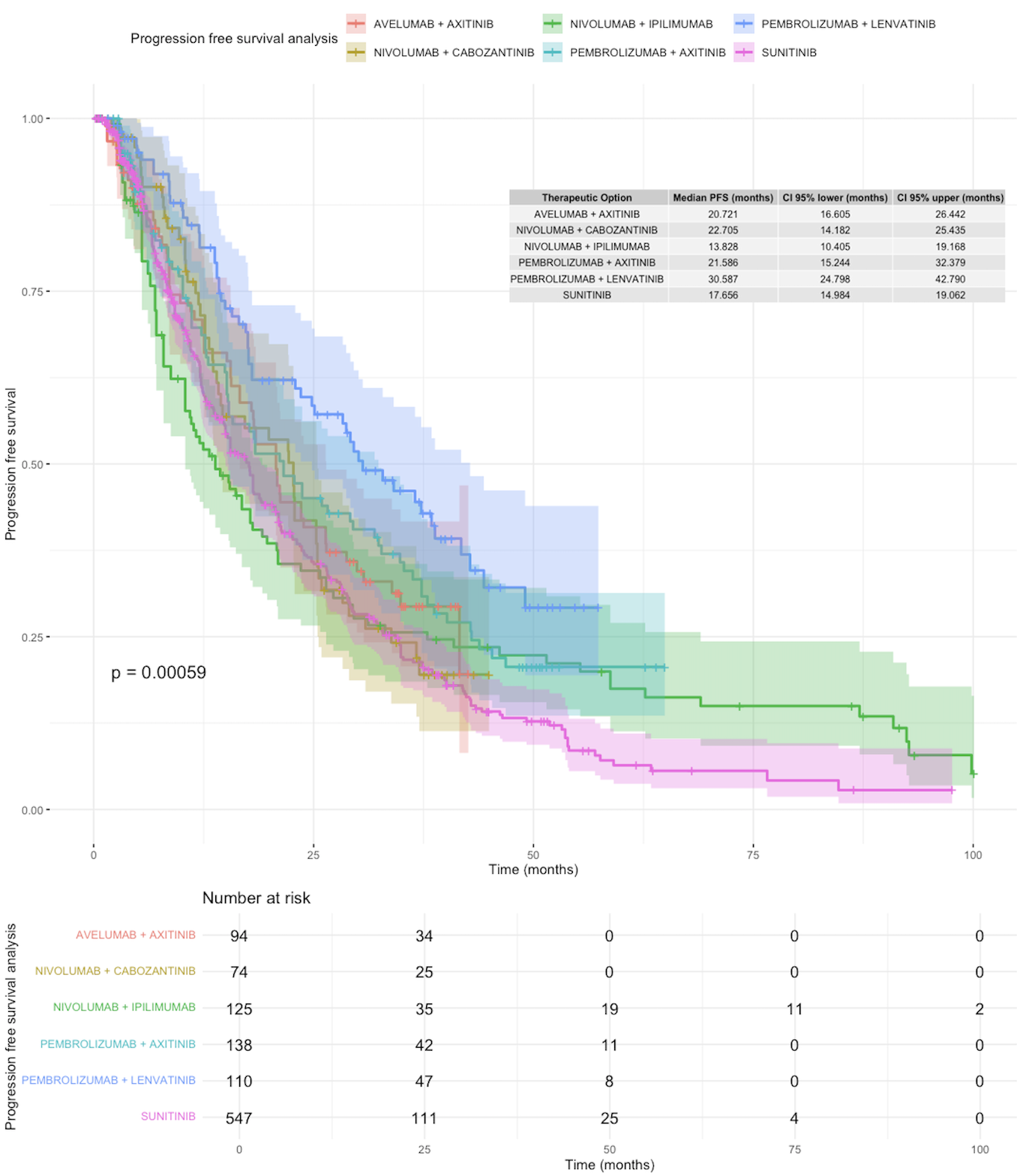
Figure 2: PFS Analysis
On the other hand, none of the ICI-based combinations showed a statistically significant benefit versus sunitinib in terms of overall survival (Figure 3), even if there were benefit trends, even if non-significant from ICI-based combinations.
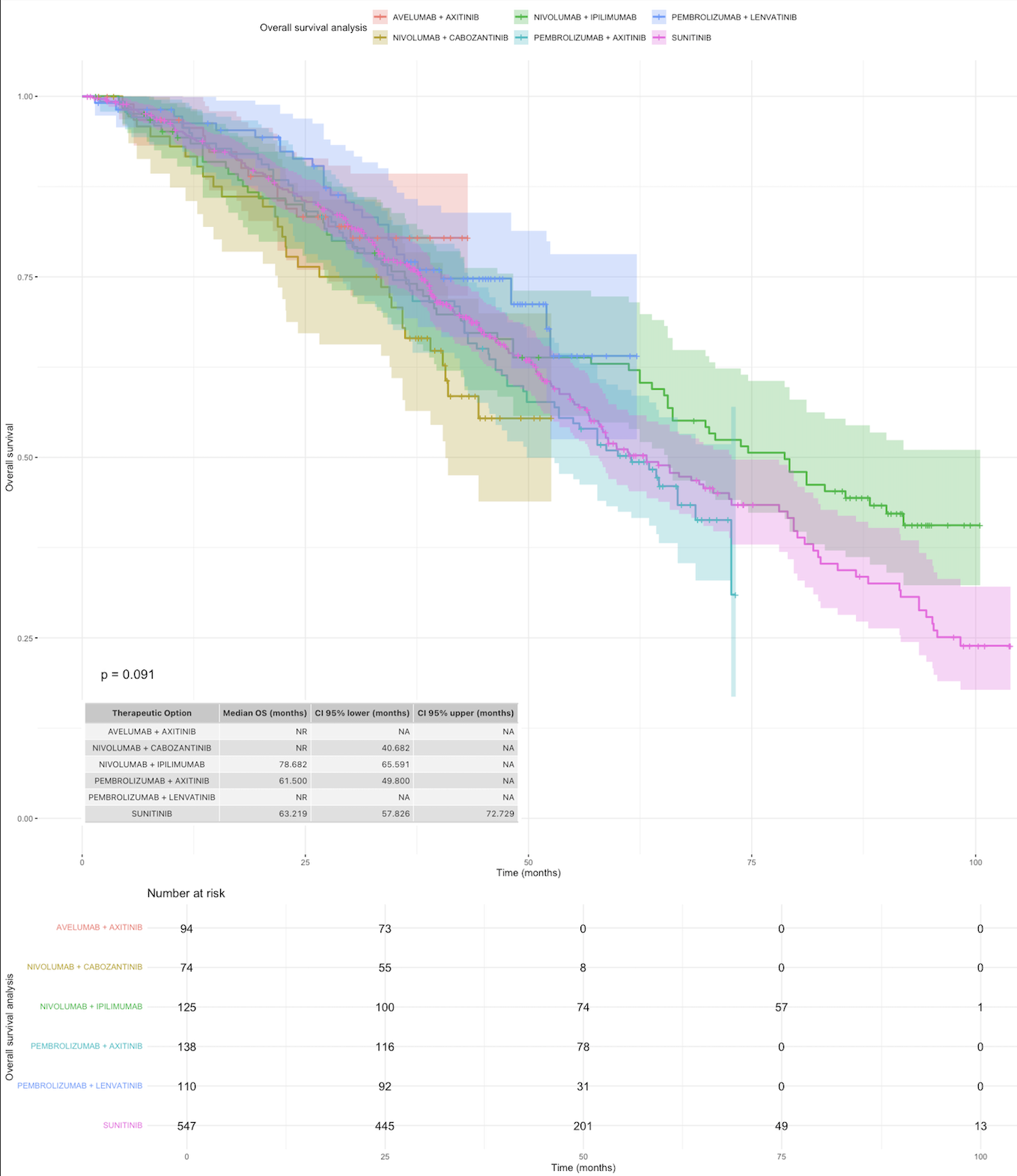
Figure 3: KM OS analysis
Data from our meta-analysis support the evidence that when approaching favorable-risk mRCC, it’s crucial to study the clinical features of every patient, and there is no single answer that works for everyone.
Probably there is a major benefit in using ICI-based combination in patients with a higher disease burden, while the monoTKI option can be viable for the Very Favorable risk patients (IMDC favorable risk characteristic and:2
- Primary diagnosis to systemic therapy ≥3 years
- Absence of brain, liver, or bone metastases
- Karnofsky Performance Status of 90–100%.
Written by: Mattia Alberto Di Civita,1,2 Daniele Marinelli,1 Valerio Marco Michetti,3 Adele Artemi,2,4 Andrea Ballario,2,5 Andrea Torchia,6 Laura Pappalardo,2,4 Martina Pecoraro,2 Iolanda Speranza,5 Alessandro Sciarra,7 Valeria Panebianco,2 Michela Roberto,5 Daniele Santini,4,5,8
- Department of Experimental Medicine, Sapienza University of Rome, Rome, Italy.
- Department of Radiological Sciences, Oncology and Pathology, Sapienza University of Rome, Rome, Italy.
- Sapienza University of Rome, Rome, Italy.
- Division of Medical Oncology B, Policlinico Umberto I, Department of Hematology, Oncology, and Dermatology, Sapienza University of Rome, Rome, Italy.
- Division of Medical Oncology A, Policlinico Umberto I, Department of Hematology, Oncology, and Dermatology, Sapienza University of Rome, Rome, Italy.
- Clinical and Molecular Medicine, Sapienza University of Rome, Rome, Italy.
- Department of Urology, Policlinico Umberto I, Sapienza University of Rome, Rome, Italy.
- Department of Medical-Surgical Sciences and Biotechnologies, Sapienza University of Rome, Rome, Italy.
- Liu, N., Zhou, Y. & Lee, J.J. IPDfromKM: reconstruct individual patient data from published Kaplan-Meier survival curves. BMC Med Res Methodol 21, 111 (2021). https://doi.org/10.1186/s12874-021-01308-8
- Martin Zarba et al. Systemic treatments in favorable and very favorable risk metastatic renal cell carcinoma (mRCC): Real world evidence from the International mRCC Database Consortium (IMDC).. J Clin Oncol 42, 4514-4514(2024) DOI:10.1200/JCO.2024.42.16_suppl.4514