We identified 231,071 patients with localized prostate cancer. 74.2% and 71.9% of patients with private insurance and Medicaid, respectively, had guideline-concordant care. In our patient-level analysis, having Medicaid insurance was associated with higher odds of guideline-concordant care among the subset with low-risk PCa (OR 1.25, 95% CI 1.12-1.40, p<0.01) but lower odds in the high-risk subsets (OR 0.67, IQR 0.62-0.73, p<0.01). Our mixed effects regression model demonstrated that individual Medicaid status, uninsured status, and facility Medicaid share quartile were associated with lower odds of receiving guideline-concordant care (Medicaid: OR 0.95, 95% CI 0.90-0.99, p=0.03; uninsured: OR 0.91, 95% CI 0.84-1.00, p=0.04; Medicaid share: OR 0.96, 95% CI 0.93-1.00, p=0.03). When stratified by clinical risk, Medicaid status was associated with higher odds of guideline-concordant care among low-risk disease (OR 1.25, 95% CI 1.12-1.40, p<0.01), and with lower odds of receiving guideline-concordant care among intermediate unfavorable risk disease (OR 0.61, 95% CI 0.55-0.68, p<0.01) and high-risk disease (OR 0.67, IQR 0.62-0.73, p<0.01).
This finding was supported by Figure 1, which showed that the probability of receiving guideline-concordant care decreased with higher facility Medicaid share among patients in the overall cohort, as well as those with intermediate unfavorable and high-risk disease. In contrast, among patients with low-risk disease, the probability of receiving guideline-concordant care actually decreased with higher facility Medicaid share.
Altogether, our study found that facilities with a higher proportion of Medicaid patients tended towards providing less or no treatment regardless of risk stratification. While this conservative management approach was appropriate in patients with low-risk disease, it was misaligned in those with higher-risk disease. From these findings, we proposed specific policy efforts to bolster the quality of care for patients with Medicaid and address the uneven distribution of care quality demonstrated in this study. For example, we suggested increasing Medicaid reimbursement rates to provide evidence-based treatment, such as definitive therapy in higher-risk patients, as well as increasing oversight of Medicaid exclusion or selective contracting practices to ensure hospitals with nonprofit status equitably serve patients with public insurance.
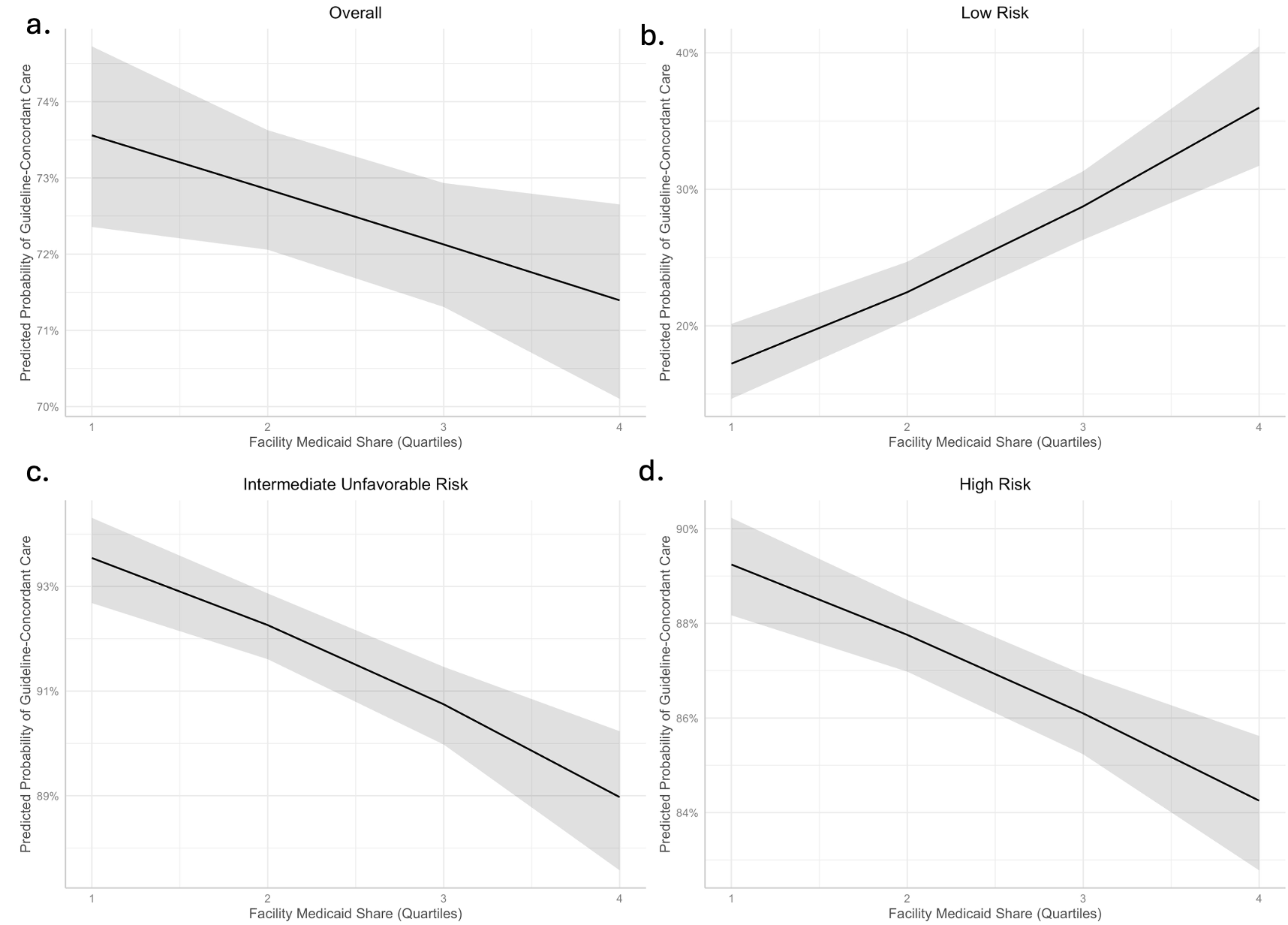
Figure 1. Predicted Probability of Guideline-Concordant Care based on Facility Medicaid Share for a. overall cohort, b. patients with low-risk disease, c. patients with intermediate unfavorable disease, and d. patients with high-risk disease.
Written by: Isaac E. Kim Jr,1 Benjamin I. Chung,1 Dhruv Puri,2 Simon J. C. Soerensen,1 James Nie,3 Walter R. Hsiang,3 Samuel Washington III,3 Michael S. Leapman4
- Department of Urology, Stanford School of Medicine, Palo Alto, RI, USA.
- Department of Urology, UC San Diego School of Medicine, La Jolla, CA, USA.
- Department of Urology, UC San Francisco, San Francisco, CA, USA.
- Department of Urology, Yale School of Medicine, New Haven, CT, USA.
Read the Abstract