Among them, pelvic nodal metachronous oligorecurrence (PNMOR) represents a common site of relapse.4 The management of nodal relapses has long been considered challenging, due to the lack of prospective evidence on local salvage approaches. Continuous or intermittent androgen deprivation therapy (ADT) long remained a standard of care in this setting, yet it is associated with an increased risk of mortality due to cardiovascular disease, and also has a detrimental effect on quality of life due to both physical and emotional side effects.5,6 With the development of PET/CT and the advent of SBRT, new therapeutic possibilities emerge for patients who experience PNMOR in a previously irradiated territory. The CYGNUS study aimed to assess both toxicity and efficacy of stereotactic body radiotherapy (SBRT) performed as a salvage approach in this population of patients.
Patients with a histological history of proven PCa, locally treated with a radical intent and a biochemical relapse as defined by the European Association of Urology guidelines, were included. All patients had a radiological suspicion of PNMOR, defined as a recurrence occurring in pelvic nodal areas with up to 5 suspect lymph nodes. Reirradiation was defined according to the ESTRO-EORTC consensus on re-irradiation as an irradiation with a geometrical overlap with a previous course of RT (Figure 1). As there is no consensus about the definition of an overlap of irradiated volumes, nodal recurrences outside the previous 20Gy isodose were excluded (27). No minimum time interval between the two irradiations was required. For exploratory subgroup analysis, two types of reirradiation were defined, based on their location relative to previous isodoses, according to a previous definition used in the OLIGOPELVIS trial (10): (1) OR occurring within a high-dose territory: when the Gross Tumor Volume (GTV) at the time of reirradiation is located within an area that already received more than 45Gy and (2) OR occurring within a moderate-dose territory: when GTV is located in an area that already received between 20-45Gy (Figure 1).
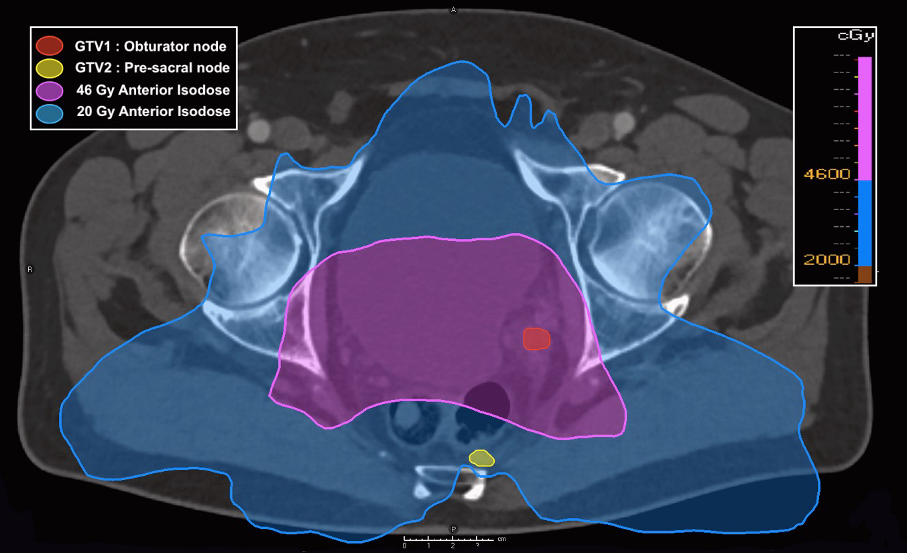
Figure 1: definition of high-dose and moderate-dose territory (according to OLIGOPELVIS)
A total of 150 patients relapsing on 192 nodal sites were retrospectively included, from 13 French centers. The majority of patients (80.7%) received radical prostatectomy as primary treatment. Radiological recurrence was detected with Choline PET/CT in 112 cases (72,3%) and PSMA PET/CT in 39 cases (25,2%). The majority of patients were treated for a single nodal recurrence (81,9%). The median PSA at treatment was 1,8ng/mL (IQR: 1-3,3ng/mL) (Table 2). The median PSAdt was 8 months. At the time of reirradiation, the median D2ccEQD2 and DmaxEQD2 values were 2.6 Gy (IQR: 0,1-6,8) and 5.5 Gy (IQR: 0,3-11,9) for the bladder, 2.4 Gy (IQR: 0,1-7,5) and 4.4 Gy (IQR: 0,1-14,6) for the rectum, and 9.8 Gy (IQR: 2,6-19) and 18.8 Gy (IQR: 5,3-48,8) for the bowels, respectively. Reirradiation was performed concomitantly with a systemic treatment for 65 patients (41.9%), constituted mostly by ADT (89%). The median duration of prescription was 6 months (range: 3-36 months). After a median follow-up of 30.5 months, late grade 2 and grade 3 GI and GU toxicity occurred in 1.9%, 0% and 7.1% and 2.6% of the cases, respectively. The 2-year radiological progression-free survival (rPFS) reached respectively 44.6%. The 2-year androgen deprivation therapy-free survival (ADT-FS) reached 59.8% (95% CI: 51.2% - 69.9%). Previous exposure to ADT was predictive in multivariable analysis of both rPFS (HR:2.02, 95%CI: 1.25-3.26, p=0.004) and ADT-FS (HR:2.49, 95%CI: 1.28-4.72, p=0.006). A PSA doubling time <5months correlated with a shorter ADT-FS (AUC 0.629,p == 0.014).
To our knowledge, this is the first retrospective multicenter study to evaluate both the toxicity and efficacy of SBRT as a salvage approach for PNMOR and hormone-sensitive PCa, occurring in previously irradiated areas. Exceedingly low rates of both acute and late severe GU and GI toxicity were noted, suggesting the safety of the approach even in patients reirradiated in a high-dose territory. Oncological outcomes are encouraging.
Written by: Ewen Anger,1 Stephane Supiot,2 Quentin Josset,3 David Pasquier,4 Loïg Vaugier,2 François-Georges Riet,5 Yoann Pointreau,6 Amandine Ruffier,6 Geneviève Loos,7 Mario Terlizzi,8 Pierre Blanchard,8 Etienne Martin,9 Paul Sargos,10 Marie Guerni,10 Ulrike Schick,11 Guillaume Bera,12 Julien Roman,13 Igor Latorzeff,14 Gilles Créhange,15 Joël Castelli,16 Anais Barateau,16 Renaud De Crevoisier,16 Luca Nicosia,17 Jennifer Le Guévelou,18
- Department of Radiotherapy, Centre Eugène Marquis, Rennes, France.
- Department of Radiation Oncology, Institut de Cancérologie de l'Ouest, Nantes, St-Herblain, France.
- Department of Radiation Oncology, Institut de Cancérologie de l'Ouest, Angers, France.
- Academic Radiation Oncology Department, Centre Oscar Lambret, Lille, France.
- Department of Radiation Oncology, Institut de Cancérologie Régional Bretillien, Saint Grégoire, France.
- Department of Radiation Oncology, Centre Jean Bernard, Le Mans, France.
- Department of Radiation Oncology, Centre Jean Perrin, Clermont-Ferrand, France.
- Department of Radiation Oncology, Gustave Roussy, Université Paris Saclay, Villejuif, France.
- Department of Radiation Oncology, Georges-Francois Leclerc Cancer Center, Dijon, France.
- Department of Radiation Oncology, Institut Bergonié, Bordeaux, France.
- Department of Radiation Oncology, University Hospital, Brest, France.
- Department of Radiation Oncology, Scorff Hospital, Lorient, France.
- Department of Radiation Oncology, Centre Saint Yves, Vannes, France.
- Department of Radiation Oncology, Clinique Pasteur, Toulouse, France.
- Department of Radiation Oncology, Institut Curie, Paris, France.
- Department of Radiotherapy, Centre Eugène Marquis, Rennes, France; LTSI, Universite de Rennes 1, Rennes, France.
- Department of Radiation Oncology, IRCCS Sacro Cuore Don Calabria, Negrar Di Valpoticella, Italy.
- Department of Radiotherapy, Centre Eugène Marquis, Rennes, France; University of Medicine, Department of Radiation Oncology, CHRU Tours, Tours, France.