Results, based on 5 trials and 4,411 participants, were published recently in European Urology.2 For the primary outcome of overall survival, we showed only a small potential absolute improvement of 1.5–2.5% at 8 years when short- or long-course HT was added to postoperative RT. However, we did see improvements of 4% at 8 years in both metastases free survival (MFS) and prostate cancer specific survival (PCSS). Treatment effects were fairly consistent across trials, despite some differences in design and participant characteristics. There was no clear evidence of a difference in effect between short- and long-course HT, for any of the outcomes. Whilst there was no strong evidence of variation in effects by participant or disease characteristics, any benefit of HT on overall survival might be limited to patients with higher pre-RT PSA levels and CAPRA-S scores.
A key strength of this work is that it was ‘done with’ the PIs and statisticians who conducted the included trials. Our collaborative approach allowed us to gain insight into the included trials, obtain consistent and detailed results, and better interpret and understand the implications of the meta-analysis. This is unlike most aggregate-data reviews, which are ‘done to’ trialists, relying solely on data and supporting information provided in trial publications, and which are therefore limited and prone to reporting biases.
As such, our analysis included results based on 96% of participants from 5 trials for the outcome of metastasis-free survival (MFS), and on 95% of participants from 4 trials for overall survival (OS) and for prostate cancer-free survival (PCSS). Importantly, we asked that trial teams supply data according to consistent, agreed definitions. We successfully obtained results by participant subgroups from most trials (Table 1a), allowing us to explore how effects of HT might vary, whilst ensuring that outcome and subgroup definitions were harmonised across trials. Such analyses would have been severely limited if based on reported results (Table 1b).
Table 1a: Subgroup data obtained via the DADSPORT collaboration
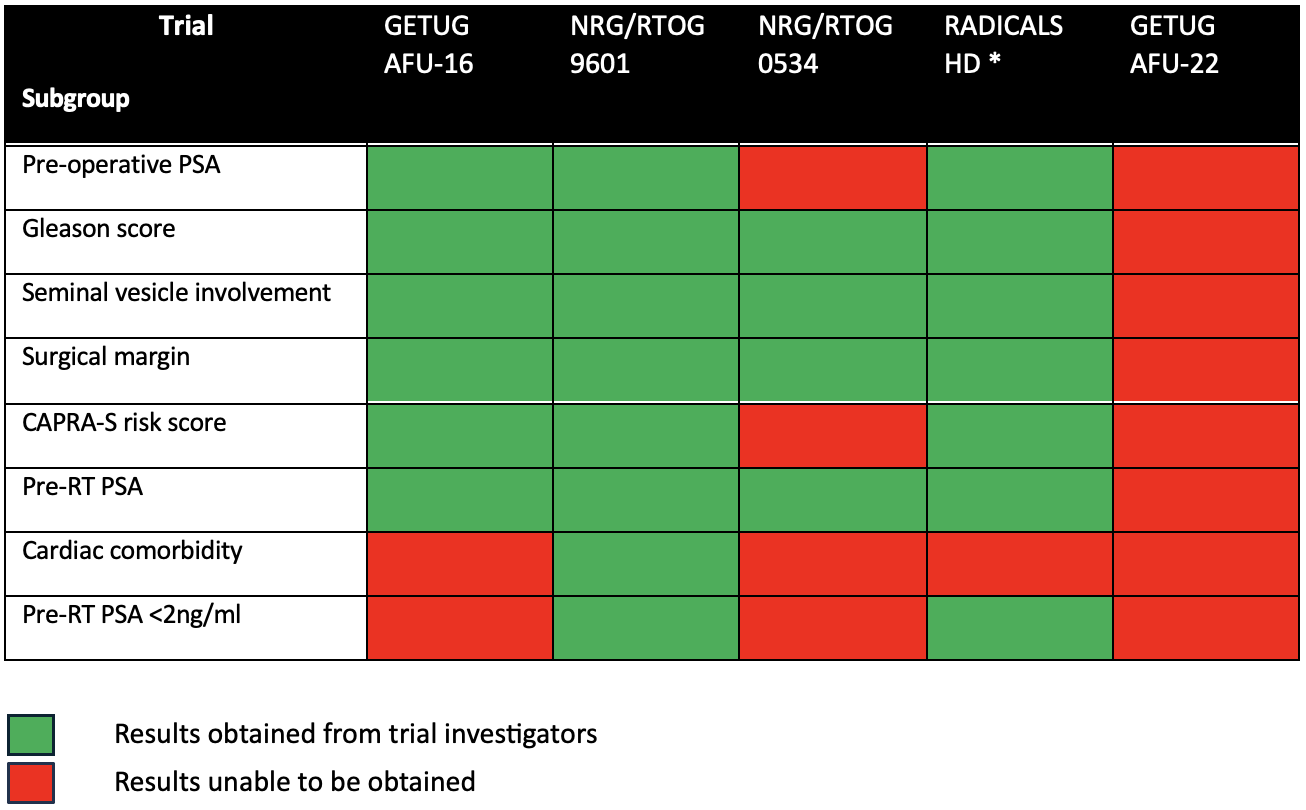
* RADICALS-HD results were made available to DADSPORT prior to the publication of the trial
Table 1b: Subgroup data available from trial publications alone
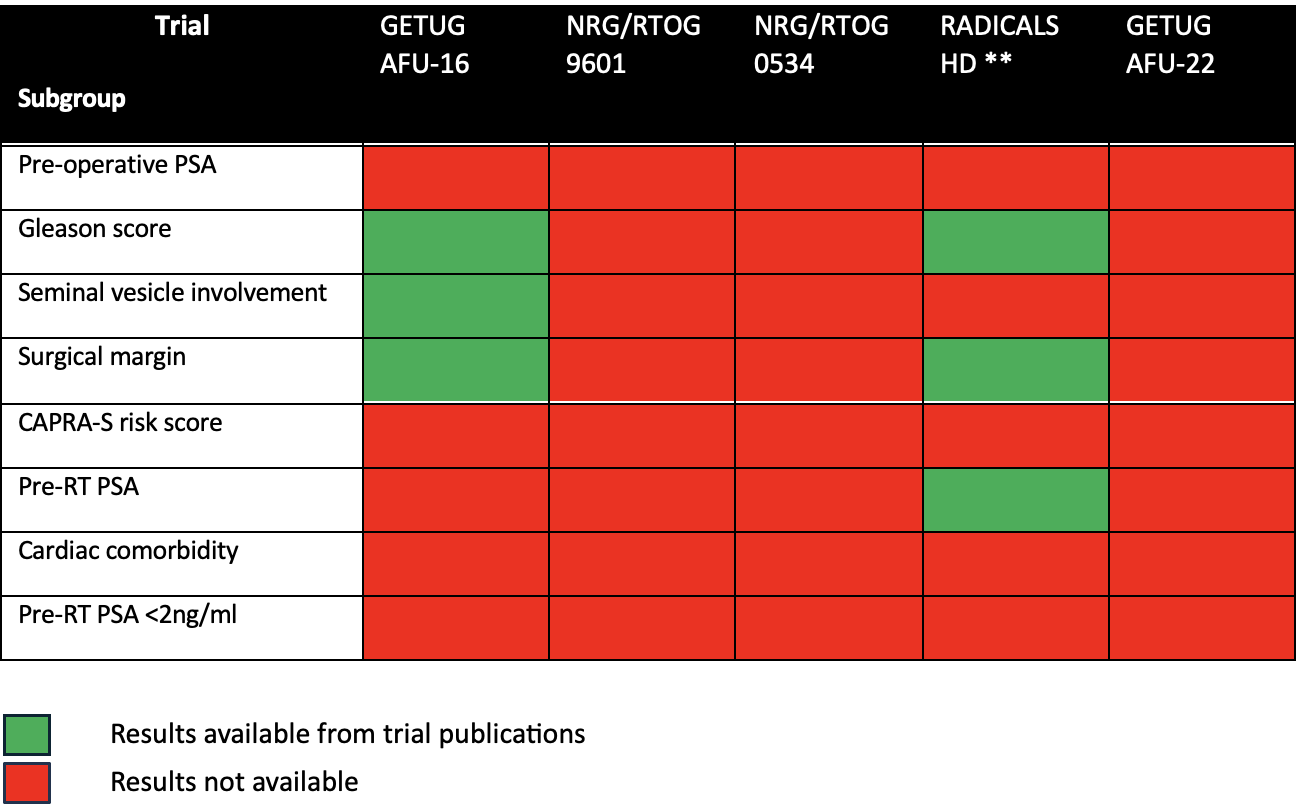
** Based on results available from the RADICALS-HD publications
Given the complex design of the RADICALS-HD trial,3-5 we required bespoke data from the trial team to enable us to perform the analyses specified in our protocol without double-counting participants. In particular, we were able to perform a network meta-analysis that directly and indirectly compared no HT, short-course HR, and long-course HT whilst appropriately including all the available data.
Our collaborative approach also meant we could seek data to address other nuances that might otherwise have been perceived as study limitations. For example, our eligibility criteria stated that participants had to have a pre-RT PSA level of <2 ng/ml, but we noted that some participants in the NRG/RTOG 9601 and RADICALS-HD trials had higher pre-RT PSA levels. Therefore, we requested additional results excluding those participants, enabling us to conduct a sensitivity analysis to check the impact of those data with respect to the original aims of our protocol.
The DADSPORT project demonstrates how, with collaboration, we can push aggregate data to give a level of detail and robustness closer to that achieved with individual participant data (IPD), but in a more timely fashion. In other projects, we have used a collaborative and prospective Framework for Adaptive Meta-analysis (FAME)(6) to achieve similar gains, whilst further reducing bias and increasing timeliness by designing and planning the review before trial results are known.
To date, FAME has been used to provide more timely, reliable, and thorough evaluation of prostate cancer treatments,7-10 with considerable impact on clinical guidelines (Figure 1). This includes providing timely insight into the adverse effects of abiraterone,8 variation in effects of abiraterone and prostate RT by age and number of metastases, respectively8,9 and the effects of RT scheduling on an earlier outcome.10 These clearly demonstrate value to evidence synthesis practice of moving away from the current retrospective, published-data paradigm to prospective and collaborative approaches. We now do this as standard in our reviews, and only then proceed to establish whether there is a need to collect IPD for more detailed analyses, as we did for our reviews of the effects of docetaxel.7,11 The existing collaborations meant that we could proceed quickly with this. Implementing FAME principles within DADSPORT has benefitted us as systematic reviewers, the trialists, and most importantly, patient care.

Figure 1: Impact of FAME in prostate cancer
Written by: Sarah Burdett, David Fisher, Claire Vale, and Jayne Tierney
MRC Clinical Trials Unit at UCL, Institute of Clinical Trials and Methodology, UCL, London, UK
References:
- Burdett S, Fisher D, Parker C, Sydes M, Pommier P, Sargos P, et al. Duration of androgen suppression with post-operative radiotherapy (DADSPORT): a systematic review and meta-analysis of aggregate data. PROSPERO: International prospective register of systematic reviews. 2022;CRD42022325769.
- Burdett S, Fisher DJ, Tierney JF, Cook AD, Spratt DE, Dignam JJ, et al. DADSPORT Meta-analysis Collaboration. Duration of Androgen Suppression with Postoperative Radiotherapy (DADSPORT) for Nonmetastatic Prostate Cancer: A Collaborative Systematic Review and Meta-analysis of Aggregate Data. Eur Urol. 2025;S0302-2838(25)00291-X:doi: 10.1016/j.eururo.2025.05.013.
- Parker CC, Clarke NW, Cook AD, Kynaston H, Catton CN, Cross WR, et al. Adding 6 months of androgen deprivation therapy to postoperative radiotherapy for prostate cancer: a comparison of short-course versus no androgen deprivation therapy in the RADICALS-HD randomised controlled trial. the lancet. 2024;403(10442):2405-15.
- Parker CC, Kynaston H, Cook AD, Clarke NW, Catton CN, Cross WR, et al. Duration of androgen deprivation therapy with postoperative radiotherapy for prostate cancer: a comparison of long-course versus short-course androgen deprivation therapy in the RADICALS-HD randomised trial the lancet. 2024;403(10442):2416-25.
- Parker CC, Clarke NW, Cook AD, Petersen PM, Catton CN, Cross WR, et al. Randomised Trial of No, Short-term, or Long-term Androgen Deprivation Therapy with Postoperative Radiotherapy After Radical Prostatectomy: Results from the Three-way Comparison of RADICALS-HD (NCT00541047). Eur Urol. 2024;86(5):422-30.
- Tierney JF, Fisher DJ, Vale CL, Burdett S, Rydzewska LH, Rogozińska E, et al. A framework for prospective, adaptive meta-analysis (FAME) of aggregate data from randomised trials. PLoS Med. 2021;18(5):e1003629.
- Vale CL, Burdett S, Rydzewska LH, Albiges L, Clarke NW, Fisher D, et al. Addition of docetaxel or bisphosphonates to standard of care in men with localised or metastatic, hormone-sensitive prostate cancer: a systematic review and meta-analyses of aggregate data. Lancet Oncol. 2016;17(2):243-56.
- Rydzewska LHM, Burdett S, Vale CL, Clarke NW, Fizazi K, Kheoh T, et al. Adding abiraterone to androgen deprivation therapy in men with metastatic hormone-sensitive prostate cancer: A systematic review and meta-analysis. Eur J Cancer. 2017;84:88-101.
- Burdett S, Boeve LM, Ingleby FC, Fisher DJ, Rydzewska LH, Vale CL, et al. Prostate radiotherapy for metastatic hormone-sensitive prostate cancer: a STOPCAP systematic review and meta-analysis. Eur Urol. 2019;76(1):115-24.
- Vale CL, Fisher D, Kneebone A, Parker C, Pearse M, Richaud P, et al. Adjuvant or early salvage radiotherapy for the treatment of localised and locally advanced prostate cancer: a prospectively planned systematic review and meta-analysis of aggregate data. Lancet. 2020;396(10260):1422-31.
- Vale CL, Fisher DJ, Godolphin PJ, Rydzewska LH, Boher JM, Burdett S, et al. Which patients with metastatic hormone-sensitive prostate cancer benefit from docetaxel: a systematic review and meta-analysis of individual participant data from randomised trials. Lancet Oncol. 2023;24(7):783-97.